
Abstract
This study assessed the feasibility of conducting 3 nonpharmacological interventions with older adults in dementia, exploring the effects of chair yoga (CY), compared to music intervention (MI) and chair-based exercise (CBE) in this population. Using a cluster randomized controlled trial (RCT), 3 community sites were randomly assigned 1:1:1 to CY, MI, or CBE. Participants attended twice-weekly 45-minute sessions for 12 weeks. Thirty-one participants were enrolled; 27 safely completed the interventions and final data collection (retention rate of 87%). Linear mixed modeling was performed to examine baseline and longitudinal group differences. The CY group improved significantly in quality of life compared to the MI group (CY mean = 35.6, standard deviation [SD] = 3.8; MI mean = 29.9, SD = 5.3, P = .010). However, no significant group differences were observed in physical function, behavioral, or psychological symptoms (eg, for mini-PPT: slopetime = 0.01, standard error [SE] = 0.3, P = .984 in the CBE group; slopetime = −0.1, SE = 0.3, P = .869 in the MI group; slopetime = −0.3, SE = 0.3, P = .361 in the CY group) over the 12-week intervention period. Overall, this pilot study is notable as the first cluster RCT of a range of nonpharmacological interventions to examine the feasibility of such interventions in older adults, most with moderate-to-severe dementia. Future clinical trials should be conducted to examine the effects of nonpharmacological interventions for older adults with dementia on health outcomes.
Introduction
Dementia is associated with decline in memory, language, executive function, and other cognitive functions. 1 In addition to cognitive impairment, dementia negatively affects physical function, including strength, balance, and motor function. 2 Limits in physical activity are likely to lead to diminished muscle mass and strength, and deconditioning, which is related to increased risk of falls. 3 Dementia is a risk factor for falls due to its associated impairment in judgment, gait, visual–spatial perception, and ability to recognize and avoid hazards. 4 Thus, falls and bone fractures are common in persons with dementia, which is a major cause of functional dependence and contributes to institutionalization. 5 In addition, sleep disturbance has been frequently observed in patients with dementia, with 45% reporting sleep problems such as insomnia, sleep fragmentation, and excessive daytime sleepiness. 6,7
Progressive deterioration in activities of daily living (ADLs) in older adults with dementia is associated with difficulty in expressing feelings and assistance, which may lead to emotional distress and behavioral symptoms. 8 There has been increasing awareness of the importance of behavioral and psychological symptoms of dementia (BPSD), including aggressiveness/agitation, wandering, restlessness, and pacing, among older adults with dementia. Behavioral and psychological symptoms of dementia can lead to premature institutionalization, decreased quality of life (QoL), increased caregiver burden, 9 and increased health-care costs. 10
Pharmacological treatment is often used to manage cognitive symptoms and to reduce the frequency and severity of BPSD. 11,12 Although psychotropic medications are commonly prescribed for BPSD, 13 high risks for drug-adverse events (AEs; eg, oversedation, dizziness, Parkinsonism, extrapyramidal effects) 13,14 from antipsychotic medications, including risperidone and haloperidol, could increase risk of falls, which increases hospital admission and mortality. 15
Current research has demonstrated that nonpharmacological interventions have positive effects in managing BPSD symptoms 16 and in contributing to QoL in persons with dementia. 17 Several nonpharmacological interventions, such as exercise/physical activity, have shown positive effects in managing dementia symptoms in older adults. 18 Recent meta-analysis has shown overall benefits of various types of exercise on functional outcomes, mood, behavioral symptoms, and cognition in older adults with mild cognitive impairment (MCI) or mild dementia. 16 However, the ability to participate in exercise programs declines with progression of symptoms of dementia, and compliance is low due to impaired cognition, mobility issues, or risk of falls and fractures. 19 In particular, some regimens (eg, aerobics) 20 are quite complex and require a high degree of physical activity that would impede many older adults with complex physical problems and moderate or profound dementia from performing them.
Although several studies have focused on the effects of physical activity, a majority have focused on older adults with MCI or mild dementia who were able to participate in standing and/or strenuous exercise (aerobic/endurance exercise, strengthening, walking). Few exercise or mind–body studies 17, 19, 21, 22 included persons with moderate-to-severe dementia. Therefore, less is known about the effects of gentle types of exercise or other movement therapies in older adults in advanced stages of dementia. More research on the effects of exercise programs on dementia symptoms in persons with various types of dementia is required. It is essential to identify evidence-based, safe, and effective nonpharmacological treatments to manage dementia symptoms in older adults with dementia.
Chair yoga (CY) provides a safe environment for stretching, strengthening, and flexibility, as well as breathing and relaxation techniques 19 through stationary poses that use isometric contraction and guided relaxation of various muscle groups,23 while decreasing the risk of falls by using a chair. 19 The current study was designed to demonstrate the effects and safety of CY compared to other nonpharmacological interventions (chair-based exercise [CBE] and music intervention [MI]) for older adults at all levels of dementia, including advanced dementia.
A pilot study 19 was conducted by our research team to test the effects of CY in managing physical function for 9 older adults with moderate or severe dementia. Using a quasi-experimental single-group design, the study assessed the feasibility of older adults with Alzheimer disease (AD) completing a CY program. The study measured only physical function; BPSD was not measured. The study was marked by the absence of randomized controlled design and control groups. It was recommended that further studies be conducted using randomization to examine the effects of CY when compared to standard nonpharmacological interventions. 19 There is currently no evidence-based CY program in randomized controlled trials (RCTs) for older adults with dementia who are unable to do standing exercise.
Objectives of the Study
The primary objective of this study was to determine the feasibility of conducting the 3 nonpharmacological interventions with older adults in various stages of dementia (mild, moderate, or severe). As the secondary objective, we explored the effects of CY, compared to MI and CBE, on improving physical function, BPSD, QoL, and sleep problems in older adults with dementia. It was anticipated that the mechanisms that underlie the physical benefits of yoga practice for persons with dementia involve the simple, repetitive movements in yoga practice that provide a sense of familiarity and the active attentional and mindfulness components that are inherent in yoga practice. 23 The following objectives guided the study.
Methods
Design
A single-blind and 3-arm cluster RCT design was used to minimize contamination among participants, with participating sites as the unit of randomization. This design also reduced differences in attrition rates among CY, MI, and CBE. We cluster randomized each research site 1:1:1 to CY (experimental group), MI (attentional control group), or CBE (activity control group), using a random numbers table. Participants were blind to the intervention at other sites (eg, those in MI did not know about CY and CBE). While the unit of randomization was the site, the unit of analysis was the individual participant. We used mixed-model statistical methodology to account for the cluster RCT’s effect for analyzing data.
Participants
Inclusion criteria were (a) 60 years or older; (b) living in the community, not institutionalized; (c) diagnosed with dementia (eg, AD, Lewy body dementia [LBD], Parkinson disease dementia) by a health-care provider; (d) at any stage of dementia (mild, moderate, or severe; Mini-Mental State Examination [MMSE] 24 ≤24; (e) a supportive and knowledgeable caregiver to accompany the participant; (f) speaks English; (g) if on dementia drugs, stable on the drugs for more than 1 month; (h) unable to participate in a regular exercise or standing yoga due to the problems with balance, cognitive impairment, or fear of falling; and (i) willing to be videotaped for fidelity check in the CY group.
Exclusion criteria were (a) MCI; (b) serious comorbidity that precludes participation in the CY or CBE intervention (eg, heart failure causing shortness of breath on exertion); and (c) refusal by the individual and/or primary caregiver.
Interventions
Participants in each of the 3 interventions (CY, MI, and CBE) attended twice-weekly 45-minute sessions for 12 weeks (24 sessions).
Chair yoga
The CY intervention is a safe mind–body therapy for older adults who are unable to participate in standing exercise; it fosters focused mental control over body movement. The CY program for this study was based on traditional Hatha yoga postures, practiced in a chair or standing and using a chair as support. The CY intervention was led by a certified yoga instructor. The CY intervention, as designed for older adults with dementia, consists of 3 components: breathing (10 minutes), physical postures (25 minutes), and guided relaxation (10 minutes). Chair yoga was designed to incorporate balance, strength, flexibility, breathing, and guided relaxation through a series of poses that use isometric contraction and relaxation of various muscle groups to develop specific body alignments. 23
The potential AEs related to participating in CY could include increased pain, muscle soreness, fatigue, or any combination of these conditions.
Music intervention
A customized participatory MI was provided to participants in the attentional control group. Sessions were led by a licensed music therapist. There were 4 components in the program: (a) welcome song and orientation to self and group (5 minutes); (b) music-facilitated movement (10 minutes); (c) cognitive/sensory stimulation (25 minutes), and (d) goodbye song (5 minutes). Although the music sessions were designed to be very general in nature and not personal or prescriptive, participants could become uncomfortable while listening to certain songs.
Chair-based exercise
Chair-based exercise is a gentle exercise regimen designed for older adults with dementia. It was developed by a physical therapist for older adults with dementia. The sessions were led by a certified fitness instructor. Participants were instructed in a CBE consisting of 3 components: warm-up and stretches (15 minutes), resistant chair exercises with a Theraband (Tband; 20 minutes), and cool down exercises (10 minutes). Adverse event from CBE participation could include pain, muscle ache, cramping, fatigue, or any combination of these conditions.
Research Sites
The CY intervention was conducted at the College of Medicine Clinical Skills Training Center at the Florida Atlantic University (FAU), Florida. Physical assessments were conducted at the Center for Comprehensive Brain Health in office space designated for this activity, equipped with a functional assessment laboratory and neuropsychological testing rooms. Both MI and CBE interventions were conducted at 2 community-based day-care centers for AD or other dementia. Both centers offer a secure, supervised environment where members spend the day engaged in meaningful and therapeutic activities. Despite variation among the research sites, each site provided services or treatment for older adults with dementia.
Study Procedure
The institutional review board of FAU approved the study protocol. A recruitment coordinator scheduled times to conduct information sessions at caregiver support groups and other community meetings to describe the study and explain research procedures to potential participants and their primary caregivers. Once a person showed interest in participating, the coordinator assigned a research assistant (RA) to call the caregiver to schedule screening, consent, and collection of baseline data. Prior to recruiting participants, the 2 RAs completed a training program in screening and data collection using the specific measures to be used in the study. They were monitored by the researchers for data collection and screening. The participants and their caregiver who was legally authorized to sign were asked to sign informed consent if they agreed to participate in the study. The RAs reviewed the consent form with caregivers of potential participants.
Prior to each intervention session, each participant was assessed on agitation level using the Richmond Agitation-Sedation Scale (RASS) 25 ; the assessment was conducted by 2 RAs with professional crisis management certificates. Scores can range from −5 (unarousable) to +4 (combative). If the score was higher than +2 (agitated) or lower than −3 (moderate sedation), participation in that session was considered to be inappropriate. The RAs also observed whether the participant was wandering prior to the session and recorded that in the checklist. If the participant was agitated or wandering prior to the session, the RAs assessed the participant’s agitation again in a private room (next to the intervention room). The RAs were instructed to talk to the participant to achieve a level of calm to be able to attend the session. If the behavior persisted, with no indication of symptom relief, the RAs were instructed to ask the caregiver in the waiting room in the same building to leave the session with the participant and return to the next session.
The RAs observed each intervention session to determine whether any AEs occurred. If a participant needed additional help regarding the behavioral symptom(s), the participant and the caregiver were referred to the participant’s health-care provider for assessment and treatment. After the 12-week intervention and data collection, each participant and caregiver received a gift card as thanks for their time and efforts.
Recruitment and Retention
Adherence to each intervention was defined as attending at least 18 of the 24 sessions of the intervention. Thirty-seven participants were contacted and screened for eligibility; 31 met inclusion criteria and 6 were excluded due to (a) MMSE 24 score >24 (n = 4); (b) caregiver was not available to provide transportation for the participant to attend the intervention (n = 1); and (c) the person with dementia declined participation (n = 1). Thirty-one participants were enrolled for the study (n = 10 [CY], n = 10 [MI], n = 11 [CBE]); 2 persons in CBE were dropped after baseline data collection but prior to start of the intervention session due to moving to the assisted living facility or caregiver’s issue. Thus, 29 participants started the interventions; 2 did not complete the CY intervention. In all, 27 participants completed the interventions and final data collection, for a retention rate of 87% (see CONSORT flow diagram, Figure 1). However, with an intent-to-treat approach, the 31 participants were included in the data analysis.
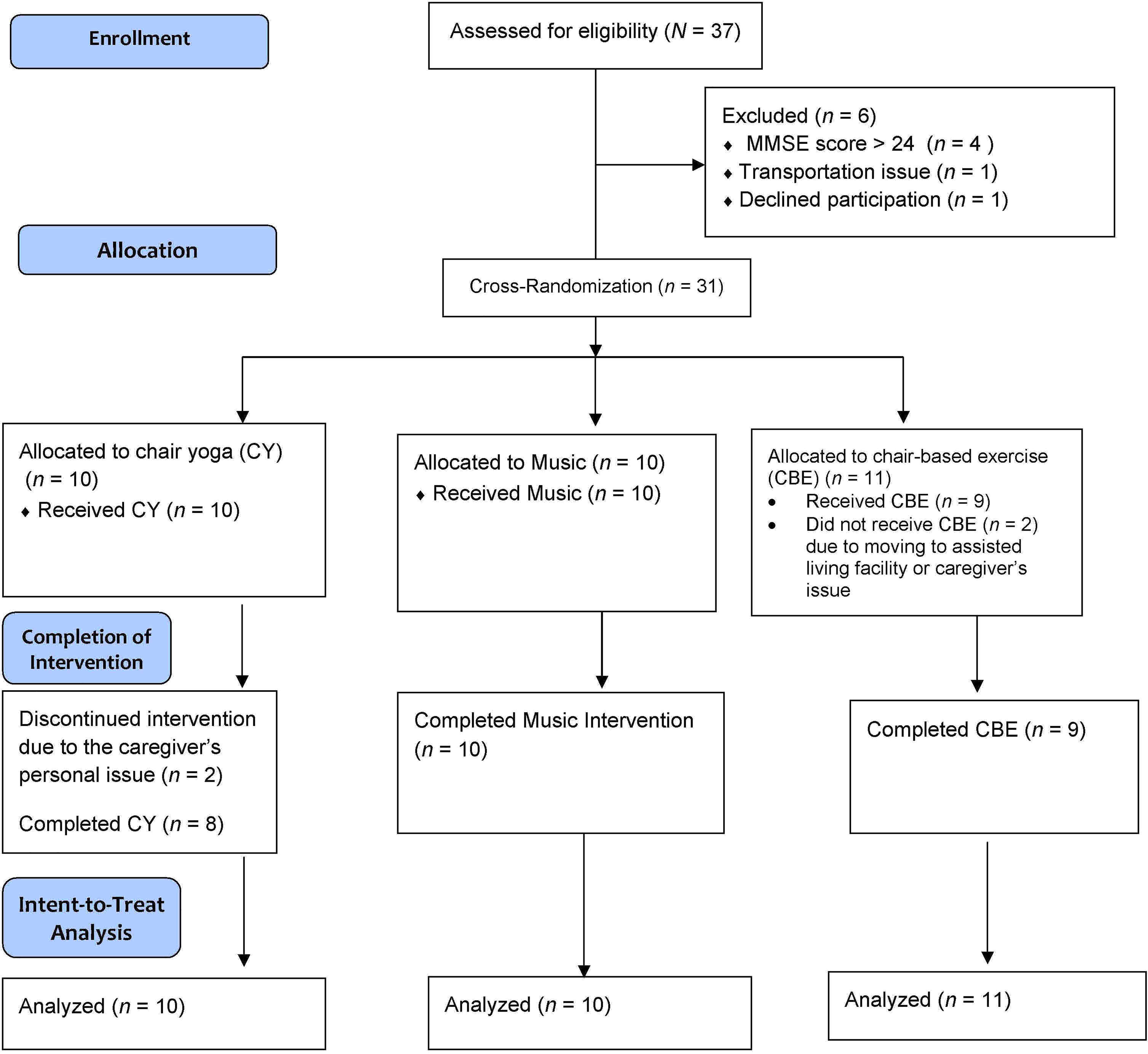
Flow of participants through the study.
Measures and Data Collection
Data were collected for each group at baseline, after 6 weeks (after 12 sessions), and after 12 weeks (at completion of the intervention). The RAs read the questions; each participant’s caregiver responded verbally because most participants did not comprehend the questions due to cognitive impairment. Baseline evaluation included the demographic questionnaire (eg, age, gender, race/ethnicity, marital status), health information questionnaire (eg, medical history, current medications), physical assessment measures, psychological assessment measures, behavioral measures, and sleep measures. Follow-up data (after 6 weeks and after 12 weeks) included only physical assessment measurements and application of psychological and behavioral tools.
After data collection was completed (baseline, after 6 weeks, and after 12 weeks), the data were entered into the REDCap database (secure cloud and isolated network infrastructure managed by the participating university’s Office of Information Technology), which has built-in security.
Mini-PPT
A 4-item version of the mini-PPT 26 has been shown to be useful for screening physical performance change in older adults with AD. The mini-PPT includes picking up an item from the floor, 50-feet walk, rising from a chair, and the progressive Romberg test. The mini-PPT includes 4 items: (a) test of standing balance (standing with feet in the tandem, semi-tandem, and side-by-side positions), (b) chair rise (sitting in and rising from a chair 5 times), (c) picking up a coin from the floor, and (4) timed 15-m walk (walking 7.5 m back and forth at maximal or habitual speed). Scores are summed to a maximum score 16, with higher scores indicating better physical performance. A score of <12 on the scale was used as an indicator of impaired lower extremity performance.
Short physical performance battery
Short physical performance battery was used to measure lower extremity function, using 3 subscales: performance-based balance, gait speed, and a short walk at usual pace and standing up from a chair 5 times in succession. Short physical performance battery has been utilized as a predictive tool for potential disability and monitoring function in older adults. Low scores on the SPPB have a high predictive value for a wider range of health consequences, including disability and loss of mobility. 27 Reliability was high at 0.87 and correlation coefficient ranged from 0.88 to 0.92.
Timed Up and Go Test
Timed Up and Go Test was used to measure mobility. 28 Participants were timed to stand up from the chair, walk 10 feet, turn, walk back, and sit down. Participants were allowed one trial to become familiar with the test. If the participant used an assistive device (eg, walker, cane) to ambulate every day, the participant was allowed to use this device to perform this test. It was ensured that the participant used the same device on the subsequent TUG. A 2- or 3-minute break between trials allowed participants to recover, depending on the participant’s condition. The average of 3 tests was calculated in seconds, timed with a stop watch. The mean time of 2 trials was used for analyses. Interrater (intraclass correlation [ICC] = 0.99) and interrater (ICC = 0.99) reliability are high for the TUG, and construct validity for mobility has been correlated with gait speed (r = −0.61) and Barthel Index (r = −0.78). 28
Body mass index
Height, weight, and waist circumference were measured. Body mass index, calculated as weight (kilograms) divided by height (square meters), was used as the outcome measure in analyses. InBody BSM170 (InBody Co, Ltd, Cerritos, California) was used to measure height and InBody (InBody 770, InBody Co, Ltd) was used to measure weight. Both weight and height were measured fully clothed without shoes. The waist circumference was measured using a standard tape.
Handgrip
A handheld dynamometer (Baseline Digital Smedley Spring Dynamometer; Patterson Medical, Warrenville, Illinois) was used to estimate handgrip strength. Maximum handgrip strength was measured in each hand with the elbow fixed at 90 degrees and the arm unsupported. The test was administered 3 trials in each hand, with the average measurement used in data calculations. No time was allowed between trials, but we alternated hands to allow some rest.
Hospital Anxiety and Depression Scale
Participants’ psychological state was assessed using the Hospital Anxiety and Depression Scale (HADS). Responses were given by the participant’s caregiver. The HADS consists of 14 questions: 7 measure anxiety (HAD-A) and 7 assess depression (HAD-D); they are summarized separately. Each item is rated on a 4-point Likert-type scale (0-3). Total scores range 0 to 21 for each anxiety and depression subscale. A sum score of 0 to 7 points is interpreted as normal, 8 to 9 points as mild, and 11 to 21 points as severe difficulty with regard to each subscale. 29 The internal consistency coefficient (Cronbach α) was .81 for the HADS and .78 and .71 for the anxiety and depression subscales, respectively. 30
Cohen-Mansfield Agitation Inventory-Short Form
Frequency of behavioral disturbance in participants was measured by the Cohen-Mansfield Agitation Inventory-Short Form. The modified 14-item short form, addressing agitation and aggression, was used in the current study to minimize risk of incomplete data. Each participant’s caregiver was asked to rate, on a 5-point scale from never to a few times an hour or continuous for half an hour or more, how often the participant had demonstrated any of the 14 agitated behaviors in the previous 2 weeks. Four subtypes of agitation (physical and verbal aggression and physical and verbal nonaggression) were summated. Higher scores indicated more frequently displayed behaviors. The internal consistency (Cronbach α) of this instrument is high (.85). 31
Quality of Life–Alzheimer’s Disease
Participants’ QoL was measured using the Quality of Life–Alzheimer’s Disease. The scale is composed of 13 items that measure the domains of physical condition, mood, memory, functional abilities, interpersonal relationships, ability to participate in meaningful activities, financial situation, and global assessment of self. These are scored on a 4-point Likert-type scale ranging from 1 (poor) to 4 (excellent). Scale scores range from 13 to 52, with higher scores indicating more positive QoL. 32
Pittsburgh Sleep Quality Index
Global sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI), a well-validated and widely used measure of global sleep quality. 33 The 19-item tool measures 7 domains, including sleep disturbance and use of sleep medication. Scores range from 0 to 21; a score of 5 or higher indicates poor sleep quality. 33 Internal consistency of the PSQI ranges from .80 to .83, with good test–retest reliability (0.87), 34 high sensitivity (99%) and specificity (84%), and good convergent validity with the sleep log. 35
Epworth Sleepiness Scale
Participants’ daytime sleepiness was measured using the Epworth Sleepiness Scale. This validated 8-item questionnaire measures subjective sleepiness. Participants were asked to rate how likely they are to fall asleep in 8 situations. Total scores range from 0 to 24, with higher scores reflecting more severe sleepiness. Scores >10 are considered indicative of significant sleepiness. 36 The Epworth Sleepiness Scale has shown adequate psychometrics in older men, α = .70, and corrected item-total correlations ≥0.30. 37
Data Analysis
Collected data were entered into a statistical software program (SAS, version 9.4). Descriptive data analyses (mean, standard deviation [SD], range, and frequencies) were conducted to identify characteristics of the study sample. To address the feasibility of recruitment, having the participants with dementia safely adhere to the intervention, and conducting the assigned interventions to examine the effects of each intervention, we used mean and range of total attendance of the participants in each group. An effect size (ES; Cohen d) was calculated for comparison of strengths of effects based on recommendations by Cohen. 38
Repeated measures analyses using a linear mixed effect modeling (LMM) approach were conducted to examine the effects of the interventions on physical, psychological, and behavioral symptoms; QoL; and sleep at baseline and over the study period. An intent-to-treat approach was employed in data analysis. The LMM approach via maximum likelihood was selected because of its ability to incorporate both fixed and random effects. This analysis modeled mean response as a combination of population characteristics (fixed effects) and participant-specific characteristics (random effects). Linear mixed effect modeling is flexible in terms of repeated measures and missing data, incorporating all available data rather than deleting records with incomplete data 39 and having malleable specifications of the covariance structure of the repeated measures. Differences between interventions were tested with a time–intervention interaction term and intercepts were included as random effects. All P values below .05 were considered indicative of statistical significance.
Results
Sample Characteristics
Table 1 displays the sample characteristics. A total of 31 participants were included in the data analyses. More participants were male (58.1%, n = 18) and a majority were non-Hispanic white (77.4%, n = 24); mean age was 84.3 years (SD = 7.7, minimum = 61 years, maximum = 100 years). The largest diagnostic group was AD (61.3%, n = 19), followed by mixed dementia (22.6%, n = 7) and LBD (9.7%, n = 3). Regarding professional assistance other than seeing primary care physician or specialists, 67.7% (n = 21) received day-care services/day health center and 19.4% (n = 6) received housekeeping services.
Demographic Characteristics of the Participants (N = 31).

Demographic and health information was collected, and standardized assessment measures were administered. There were no significant demographic differences among intervention groups. Mean MMSE score was 14.7 (SD = 5.65, minimum = 1, maximum = 23, mode = 19). Regarding level of independence, 45.2% (n = 14) were completely dependent and required caregiver assistance. Fifty-one percent (n = 16) were currently living with a spouse and 32.3% were living with their children. More than half of the participants (67.7%, n = 21) were taking medication(s) to manage symptoms associated with dementia. Of the participants who were on dementia medications, more than one-third (38%) were taking Namenda. The mean of duration of dementia was 4.75 years (SD = 2.7 years).
Primary Objective: Adherence and Feasibility of the Study
Adherence to each intervention was assessed by maintaining attendance records and calculating the percentage of total sessions attended. Adherence to each intervention was defined as attending at least 18 of the 24 sessions of the intervention. Twenty-nine participants started the interventions, 2 left due to moving to a higher level of care or the caregiver’s personal issues, and 27 (87%) completed the interventions (23 of whom completed at least 18 sessions; Figure 1). Mean numbers of sessions attended were as follows: CY = 18.3 (SD = 4.7), MI = 23 (SD = 0.8), and CBE = 18.7 (SD = 2.9). The main reasons for nonattendance were doctor’s appointments, illness, or caregiver’s personal schedule. More than 97% of the participants fully engaged in each session. No AE associated with participation in the intervention occurred. Research assistants assessed each participant’s agitation level and recorded the score based on RASS prior to each intervention session. Most participants were assessed as alert (score 0 using RASS) 25 prior to each intervention session; 1% were assessed as slightly agitated. For those who were agitated prior to the session, 2 RAs (holding professional crisis management certificates) assessed the participant’s agitation in a private room next to the intervention room. The participants became calm after the RAs talked to them and attended the session without signs of agitation during the session. The RAs also observed each session to respond to an emergency situation if any participant became agitated or wandered. No participant showed any indication of such symptoms during the sessions. All 3 interventions were assessed to be safe; none of the participants was physically injured, agitated, wandering, or crying during the interventions.
Effect size of outcomes between interventions ranged from 0.10 (small ES) to 1.39 (large ES), with most of the outcomes of moderate size (eg, ES = 0.66; Table 2.) The largest ES was observed in depression at mid-intervention and the smallest ES was in physical performance change between CBE and MI at baseline. Effect size of all outcomes between 2 interventions: (a) ES (CY:MI), (b) ES (CBE:MI), and (c) ES (CY:CBE) are presented in Supplemental Appendix A.
Mixed-Effects Models Assessing Group Differences in Physical and Psychosocial Outcomes by Assessment Time.

Abbreviations: BMI, body mass index; CBE, chair-based exercise; CI, confidence interval; CY, chair yoga; Epworth, Epworth Sleepiness Scale; ES, effect size; MI, music intervention; mPPT, mini-PPT; PSQI, Pittsburgh Sleep Quality Index; QoL, quality of life; SD, standard deviation; SPPB, Short physical performance battery; TUG, Timed Up and Go Test.
a Bold shows significance level. Reference group = MI.
Secondary Objective 2.1: Effect of Intervention on Physical Function
No between-group differences were observed at baseline, with the exception of handgrip strength, which was significantly higher in the CY group (mean = 26.4, SD = 7.8, P = .010) than in the MI group (mean = 14.7, SD = 9.5). However, nonsignificant increase in the CBE group was observed (mean = 20.9, SD = 9.4, P = .161; Table 2) compared to the MI group. Significance was reached only for mini-PPT scores (Figure 2; mean = 8.8, SD = 3.8, P = .030), and no significance was found for SPPB scores (mean = 6.7, SD = 2.9, P = .055) at mid-intervention. For comparison, means for the MI group were 4.7 (3.7) for mini-PPT and 4.0 (2.8) for SPPB. However, longitudinal analyses revealed no significant differences among the 3 groups. None of the 3 groups declined significantly in any of the investigated physical functional measures (eg, for mini-PPT: slopetime = 0.01, standard error [SE] = 0.3, P = .984 in the CBE group; slopetime = −0.1, SE = 0.3, P = .869 in the MI group; slopetime = −0.3, SE = 0.3, P = .416 in the CY group; Table 3).

Mean scores of mini-PPT by nonpharmacological Intervention.
Mixed-Effects Models Assessing Longitudinal Differences in Physical and Psychosocial Outcomes Between Intervention Groups.

Abbreviations: BMI, body mass index; CBE, chair-based exercise; CI, confidence interval; CY, chair yoga; Epworth, Epworth Sleepiness Scale; ES, effect size; MI, music intervention; mPPT, mini-PPT; PSQI, Pittsburgh Sleep Quality Index; QoL, quality of life; SD, standard deviation; SE, standard error; SPPB, Short physical performance battery; TUG, Timed Up and Go Test.
a Bold shows significance level. Reference group = MI.
Secondary Objective 2.2: Effect of Intervention on Psychological Symptoms
No significant between-group differences in anxiety were observed at any time point. Both the CY and CBE groups, compared to the MI group, showed lower depression across all 3 time points (eg, at postintervention: meanCY = 8.4, SD = 4.1; meanCBE = 8.3 [5.0]; meanM I = 12.3 [4.8], P CYvsMI = .088, P CBEvsMI = .076). There was a statistically significant difference in depression between CY and MI at mid-intervention (meanCY = 6.8, SD = 3.1 vs meanMI = 11.8, SD = 4.1, P = .018). However, no significant differences were noted for CBE at data collection points (baseline, mid-intervention, and postintervention) except at baseline (P pre = .049; P mid = .083; P post = .076 and for CY P pre = .065; P post = .088). There were no significant between-group differences in change in depression and anxiety (Table 3). Although a significant increase in depression was observed in the MI group (slopetime = 1.5, SE = 0.4, P = .002) and in the CBE group (slopetime = 1.0, SE = 0.5, P = .037), no significant change was noted for the CY group (slopetime = 0.8, SE = 0.5, P = .118). Similar results were observed for anxiety (slopetime = 1.1, SE = 0.6, P =.053 for MI; slopetime = 1.2, SE = 0.6, P = .034 for CBE; while slopetime = 0.9, SE = 0.6, P = .144 for the CY group).
Secondary Objectives 2.2 and 2.3: Effect of Intervention on Behavioral Symptoms and Sleep Problems
No significant group differences among the 3 intervention groups were observed for agitation level or sleep quality at any of the 3 time points. Also, no differences were observed among the 3 intervention groups in terms of change in behaviors over the study period. However, it is noteworthy that agitation increased significantly in the CY group (slopeCY = 3.7, SE = 1.5, P = .001), although no similar results were observed in the CBE or MI groups (Table 3).
With regard to QoL, higher scores were found in the CY group (mean =35.0, SD = 3.3, P = .069) compared to the MI group (mean = 31.2, SD = 4.1) at mid-intervention. These scores reached statistical significance at postintervention (meanCY = 35.6, SD = 3.8, meanMI = 29.9, SD = 5.3, P = .010; Table 2 and Figure 3). There was also a higher score in QoL in the CBE group (mean = 33.9, SD = 3.4, P = .056) than in the MI group at postintervention (Table 2). In mixed-effects models, while the MI group significantly declined in QoL over the study period (slopetime = −1.5, SE = 0.7, P = .032), the rate of decline was significantly slower in the CBE group (slopetime = 2.1, SE = 0.9, P = .029) and particularly in the CY group (slopetime= 2.4, SE = 0.9, P = .015) as compared to the MI group. The rate of decline in QoL was significantly steeper in the MI group (slope MI × time = −2.1, SE = 0.9, P = .029; Table 3) when compared to the CBE (slopetime = 0.6, SE = 0.7, P = .333).

Mean score of quality of life scores by Intervention.
Discussion
The current study determined that it was feasible to recruit and have participants with dementia adhere safely to the 3 interventions, which was the main focus of this article. The fundamental findings demonstrated that, participants at all levels of dementia (most with moderate-to-severe dementia) completed CY, CBE, or MI without falling or being injured and with becoming agitated during the intervention. Safety is an appealing aspect of the 3 interventions as complementary therapy for many dementia populations since no injury or other advents (including muscle soreness) occurred.
It is important to highlight a relatively low attrition rate of the participants with dementia during the 12-week interventions, which supports the idea that older adults in all types and at all stages of dementia can complete the interventions. Although some participants showed mild levels of agitation or wandering in the classroom prior to the session, they became calm after they were assessed by the RAs. Once a session started, these participants engaged in the intervention and followed the interventionist’s instructions.
The study findings indicated that QoL improved more in participants in the CY and MI groups after the 12-week intervention than those in the MI group; both exercise groups (CY more so than CBE) showed improvement over time, while a decline was seen for the MI group. It is plausible that physical poses in CY or CBE can improve QoL because stretching, strengthening, and flexibility through poses that use isometric contraction and relaxation of various muscle groups 23 could lead to experiences of bodily sensation and could reduce current tension and improve relaxation, 40 which may be related to improvement in QoL. However, findings regarding QoL were mixed from the previous studies in older adults with cognitive impairment after they attended physical activity or exercise studies. 41 -43 For example, (a) 90-minute, 3 times weekly adapted physical activity sessions for 6 months 41 were provided to older adults with AD, (b) older adults with MCI received 16-week moderate-intensity aerobic stepping exercise program with 3 times a week for 16 weeks. 42 Contrary to the positive findings in QoL, more intensive exercise such as cycling for 10- to 45-minute 3 times for 6 months was conducted, the change in QoL was not statistically significant from baseline to 6 months 42 among patients with AD. However, no studies focused on older adults with moderate-to-severe dementia who are unable to attend standing or rigorous exercise. The major difference from the previous studies is that both CY and CBE were able to accommodate patients with dementia who could not participate in strenuous exercise program due to the problems with balance, cognitive impairment, or fear of falling.
Except for QoL, no significant between-group differences in physical function (balance and mobility), behavioral (nocturnal agitation behaviors), psychological (anxiety, depression), or sleep problems and daytime sleepiness were found longitudinally. The findings were consistent with previous findings from a 10-week CY study of older adults with AD, where no significant change in balance or anxiety was observed after the intervention 12 but ADLs improved significantly (P = .02). In another CY study, 19 balance was significantly improved (P = .034) from baseline to 4 weeks, postintervention, and 1-month follow-up.
A significant increase in depression scores was seen in all 3 intervention groups over the study period, which means that depression in older adults with dementia, particularly those at an advanced level (mean MMSE score = 14.7) worsened after participation in each of the interventions. This result is consistent with the finding from a previous CY study of older adults with AD 21 and physical exercise with MCI or mild dementia, 8 in which depression significantly worsened, mainly in older adults with moderate-to-severe AD (the same target population as the current study). In a similar type of exercise program study, 44 effects of aquatic and land-based exercise programs were compared; no significant difference in participant behavior or mood was observed in either group. 42
However, contradictory to the findings from the current study, it is interesting to note that depression significantly decreased in most of yoga studies for older adults with MCI or mild level dementia. It is possible that yoga practice can improve mood and neuropsychiatric symptoms in older adults with MCI or mild dementia; however, depression does not seem to be improved after yoga practice in those with advanced dementia. A slower rate of increase was found in the CY group than in the MI group. As another explanation, it is plausible that 45-minute, twice-weekly CY sessions for 12 weeks may not have been sufficient to elicit a meaningful change in terms of intensity and duration of CY provided to the participants.
Agitation increased in all 3 groups over the study period, with the highest increase observed in the CY group, as measured on the RASS 25 prior to each intervention. Those who were slightly agitated became calm after the RA talked to them. It is possible that, because participants’ agitation behaviors were observed and reported by caregivers, the caregivers did not have an opportunity to observe the participants’ behaviors during the intervention and the participants may have been more agitated at home than they were in the intervention group. Contradictorily, although the CY group showed the highest increase in agitation, the group reported a higher QoL score, including physical condition, mood, functional abilities, interpersonal relationships, ability to participate in meaningful activities, and final situations. Quality of life is a more comprehensive approach to biopsychosocial and behavioral function than a mere measure of agitation. Bringing attention to the body during the meditation (mind–body connection) component of the program may have increased QoL. 19 This would be consistent with our earlier work in which we found that a targeted approach was successful in increasing QoL in patients with dementia.
Limitations and Implications
A cluster RCT was used to avoid risk of cross-contamination and to reduce risk associated with factors that influence outcomes. Although a rigorous design was used, the current study has acknowledged limitations. Data collectors were not blind to site assignment; they were aware of interventions at other sites, although participants were blind to the interventions at other sites. No pure control group (eg, wait-list control group) was included to compare the effects of each of the 3 nonpharmacological interventions. Measurement errors were possible, as measures of BPSD, sleep problems, and QoL (except physical function) were collected from the primary caregivers, not from the participants with dementia due to their cognitive impairment. Although the cluster RCT prevented cross-contamination, individual differences were less likely to be controlled, compared to a pure RCT, because individuals were not the unit of randomization.
Since the current study showed that it is feasible to conduct these 3 nonpharmacological interventions without injury, CY or CBE could be practiced in nursing homes or assisted living facilities under supervision of staff for their older patients with dementia, even those in advanced stages. Based on the feasibility data from this study, power analysis and sample size with the ES of the outcomes can be estimated; future clinical trials should be conducted to examine the effects of nonpharmacological interventions for older adults with dementia on health outcomes, including physical function, psychological and behavioral symptoms, and sleep disturbance. In addition, it would be important to identify evidence of the appropriate length, intensity, and frequency of the interventions to produce benefits for older adults with advanced levels of dementia.
It is suggested that CY and CBE interventions be provided to caregivers along with their patients with dementia. It would be beneficial to provide caregivers effective strategies and resources to assist participants to engage in the intervention and obtain the sustained effects of such interventions. Patients with dementia and their caregivers could attend CY or exercise together, and patients with dementia could be encouraged to practice the CY or exercise routine at home with the caregiver’s assistance. Future research should collect follow-up data to measure the sustainability of the interventions. It is important that future research determine whether CY participants reduce use of psychotropic medications and reduce risk of drug AEs.
Conclusion
Overall, the current pilot study is notable as the first cluster RCT of a range of nonpharmacological interventions to examine the feasibility of such interventions and potential effects in improving dementia symptoms. It was concluded that twice-weekly 45-minute sessions for 12-week interventions are safe and feasible for persons with various stages of dementia, even those in later stages, who are unable to participate in regular exercise that requires standing without support. More research is necessary to demonstrate positive clinical outcomes and to provide more options for an evidence-based intervention that could be used for this vulnerable population.
Supplemental Material
Supplemental Material, Nonpharm_Dementia_Supplementary_Material_7-7-19_FINAL - Feasibility of Conducting Nonpharmacological Interventions to Manage Dementia Symptoms in Community-Dwelling Older Adults: A Cluster Randomized Controlled Trial
Supplemental Material, Nonpharm_Dementia_Supplementary_Material_7-7-19_FINAL for Feasibility of Conducting Nonpharmacological Interventions to Manage Dementia Symptoms in Community-Dwelling Older Adults: A Cluster Randomized Controlled Trial by Juyoung Park, Magdalena I. Tolea, Diane Sherman, Amie Rosenfeld, Victoria Arcay, Yve Lopes and James E. Galvin in American Journal of Alzheimer's Disease & Other Dementias
Footnotes
Acknowledgments
The authors thank the study participants and their dedicated family caregivers.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Juyoung Park is a member of the faculty of the Florida Atlantic University School of Social Work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Florida Atlantic University, Division of Research, Institute for Healthy Aging and Lifespan Studies.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.