
Abstract
A Language-Enriched Exercise Plus Socialization (LEEPS) Program for older adults with Alzheimer’s disease and related disorders (ADRD) was implemented in rural Wisconsin communities. Patterned after a university-based research intervention, 1 the LEEPS protocol entailed ongoing weekly to biweekly sessions with a trained volunteer and an individual with dementia, with exercise and language stimulation sessions interspersed with social or volunteer outings. Of 64 persons with ADRD who enrolled, 29 completed an initial follow-up assessment at an average of 10.65 months, and 8 completed a second follow-up at an average of 20.55 months. Results generally show stability in cognition, mood, and physical performance. Improvement was noted at the initial retest on 1 of the 3 physical fitness measures (arm curls; t = 2.61, P = .015), but self-rated quality of life declined slightly from baseline to the first retest (t = −2.09, P = .048). Change in the Mini-Mental State Examination at the first and second follow-ups (mean = +0.18 and −1.0, respectively) was negligible. The maintenance of function observed with LEEPS is an encouraging outcome, given the progressive nature of ADRD, but controlled investigations are needed to establish the efficacy of LEEPS. Barriers to implementation of an intensive activities-focused intervention in rural communities are discussed.
Introduction
The cognitive, social, and physical consequences of Alzheimer’s disease and related disorders (ADRD) pose enormous challenges to affected individuals, their families, and society as a whole. Currently, at least 4.7 million persons in the United States are living with Alzheimer’s disease (AD) alone and that number is expected to nearly triple by 2030 to an estimated 13.8 million. 2 Costs of caring for persons with ADRD in the United States have been estimated to range between US$41 689 and US$56 290 per year in 2010 dollars. Based on purchased care alone (ie, not including services provided by unpaid family caregivers), dementia ranks as one of the costliest diseases to society, on par with direct health care expenditures for heart disease and significantly more costly than cancer. 3
The high prevalence, progressive nature, and lengthy duration of dementing disorders threaten to overwhelm existing health and long-term care systems, increasing the urgency to develop and validate interventions that can enable affected persons to sustain as high a level of function for as long as possible. Although the search for pharamacotherapies is ongoing, there is currently no pharmacologic or medical therapy that can alter the course of ADRD, and symptomatic relief from medications approved by the Food and Drug Administration is often too subtle to have clinical impact. Nonpharmacologic interventions are now being studied systematically and intensively, and a growing body of evidence suggests potential benefit from such interventions.
Cognitive, physical, and social engagement have all been associated with a reduced risk of developing dementia, 4 and programs providing cognitive training, structured cognitive activities, physical exercise, and focused social engagement have shown benefits for cognitively normal older adults. 5,6 Cognitive training and physical exercise have also been found to improve cognitive performance for persons with mild cognitive impairment. 7,8 For persons diagnosed with dementia, there have been fewer well-controlled studies, 9,10 but some promising models have been developed that are appropriate for persons living with dementia in the community. 11,12 Because multi-modal engagement combining cognitive, physical, and social stimulation is most effective in reducing risk of dementia, 13 there has been interest in developing programs that engage persons with dementia in multiple ways to potentially maximize benefits for sustaining function and slowing decline. Most such programs have been offered in group formats, often in a day care setting. A few individualized multi-modal programs have been developed for community dwellers, 14 of which the Elder Rehab Program 1 developed by Arkin is among the most intensively studied. Elder Rehab combined alternating biweekly sessions of physical exercise with language stimulation and social or volunteer outings. Interventions were implemented with trained volunteers who worked individually with older adults with AD over periods of 1 to 4 years. Results showed improved physical fitness performance, 15 and rate of cognitive decline was slowed for program participants compared to a large normative sample. 1
We recently implemented an adapted version of the Elder Rehab program with older adults residing in several Wisconsin communities. The aim of this study was to evaluate the effects of this program on cognitive performance, physical fitness, and measures of well-being for persons with mild dementia. A detailed description of Language-Enriched Exercise Plus Socialization (LEEPS) procedures has been previously reported 16 together with preliminary outcomes. The present report summarizes results for the sample as a whole, compares findings with those of the original Elder Rehab research, and discusses successes and barriers encountered in translating a complex psychosocial intervention to rural communities.
Method
The LEEPS intervention was patterned closely after Arkin’s original protocol, with variations as needed to accommodate the different participant population and rural environment (eg, low population density, fewer facilities, and services). This intervention was chosen because of its multi-modal nature, individualized programming, and reliance on volunteers to deliver the intervention. It was our hope that multi-modal activities would attract and retain a diverse group of persons with dementia. The individualized delivery format was well suited to rural areas where sparse populations often preclude group programs, and the use of volunteers to deliver the service offered the greatest potential for sustained, cost-effective continuation once initial funding had expired.
This study was a 1-arm trial of the LEEPS intervention (quasi-experimental design), with no control condition. The program was implemented in 9 Wisconsin counties, including an 8-county Southwestern region with a predominantly rural population and an adjacent county with a substantial African American population. Based on the rural–urban classification system developed by the Wisconsin Office of Rural Health using zip codes and 2010 census data, 17 the 8-county region was predominantly R1 (no population center greater than 2500) and secondarily R2 (population centers up to 9999), whereas the adjacent ninth county was predominantly urban. The LEEPS program was a joint effort of the Wisconsin Department of Health Services, the Wisconsin Alzheimer’s Institute of the University of Wisconsin-Madison, and community partners, including regional Aging and Disabilities Resource Centers and the Alzheimer’s Support Center, a local organization providing dementia-related services. The project was supported by the US Administration for Community Living’s Alzheimer’s Disease Supportive Services Program. All study procedures were approved by the institutional review board of the University of Wisconsin-Madison.
Participants and Volunteers
Community-residing persons with mild dementia were eligible for LEEPS. Participation as a LEEPS volunteer was open to anyone older than the age of 18 years who passed a background check, provided appropriate personal references, and committed to a minimum of 3 months of involvement after training. Recruitment and screening of participants and volunteer training procedures are described in Appendix A.
Assessment
The original Elder Rehab program tracked outcomes with annual assessments. In LEEPS, reassessments were scheduled as close as possible to 1-year intervals (minimum interval = 8 months). Cognition, physical fitness, mood, and quality of life were assessed at baseline and follow-ups with the measures shown in Table 1 (see Appendix A for information on assessment tools). The Mini-Mental State Examination (MMSE) 18 was considered the primary cognitive measure in light of its widespread recognition as a clinical tool and the breadth of skills assessed.
Initial Follow-Up Results.a
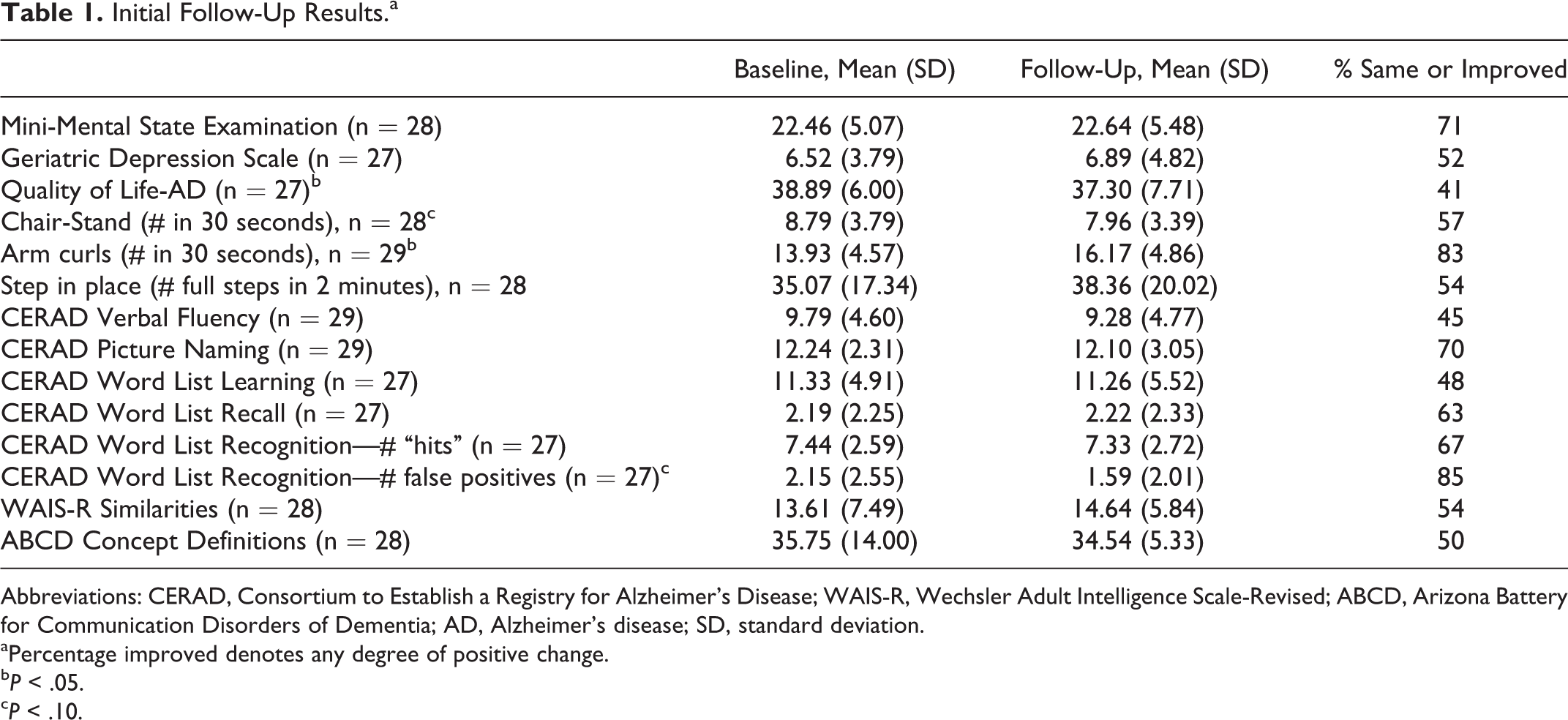
Abbreviations: CERAD, Consortium to Establish a Registry for Alzheimer’s Disease; WAIS-R, Wechsler Adult Intelligence Scale-Revised; ABCD, Arizona Battery for Communication Disorders of Dementia; AD, Alzheimer’s disease; SD, standard deviation.
aPercentage improved denotes any degree of positive change.
b P < .05.
c P < .10.
Intervention Methods
The intervention plan called for each participant and volunteer pair to meet on a twice weekly basis, once for exercise plus language stimulation and once for a social outing (eg, eating out) or volunteer work (eg, reading to school children). Illness, vacation, or scheduling difficulties reduced the number of visits on some occasions. Volunteers logged activities completed at each session.
Physical exercise procedures followed a manual developed by Arkin 19 wherever possible, with adaptations as needed to allow for in-home exercise and to accommodate participants with balance problems or other physical limitations. Exercise training was embedded in weekly exercise plus language stimulation sessions lasting an average of 1½ hours. Individualized exercise protocols were developed through consultation with a physical therapist, taking into account any restrictions specified by the person’s physician. Language exercises were designed to promote sustained attention, deep processing of language and semantic content, and production of verbal responses on demand and are described in detail elsewhere. 1,16,19 Although the protocol also called for weekly social or volunteer outings, due to limitations in volunteer availability, these outings occurred less frequently for some participants in LEEPS. Selection of outings and volunteer opportunities varied with participant preferences and local availability. Additional information on the intervention methods is provided in Appendix A.
Statistical Procedures
Because there was no control or comparison condition, analyses focused on examining change from baseline to first and second follow-ups. Paired t tests were used for longitudinal comparisons. Although decline would be the generally expected direction of change for persons with ADRD over the time period of this investigation, we used 2-tailed tests of significance to allow for the possibility that performance might improve on some measures over the course of intervention. Comparisons of baseline characteristics between participants with follow-up data and those with no follow-up used F tests for continuous measures and chi-square or Fischer’s exact tests for categorical variables. Level of statistical significance was set at P < .05, but in light of the exploratory nature of the study, marginally significant effects (P < .10) were also examined where appropriate. Findings were descriptively compared to changes observed over similar time periods in the original Elder Rehab research, and for the MMSE, with published normative outcomes. 20,21
Results
Language-Enriched Exercise Plus Socialization Participants and Volunteers
Sixty-four older adults with ADRD completed baseline assessments. The sample was predominantly non-Hispanic white, advanced in age (61% were 80 years or older), and included dementia diagnoses in addition to AD. Thirty-one trained volunteers of diverse ages and backgrounds were paired with LEEPS participants in their areas. Details of participant and volunteer characteristics are provided in Appendix A.
Attrition Effects
Of the 64 participants who completed baseline assessments, 29 participants remained active in the study through the first follow-up (average interval = 10.65 months, standard deviation [SD] = 2.00, range = 7.12-15.15) and 19 started the intervention but withdrew from the study before a follow-up was completed. In all, 10 who withdrew entered long-term care facilities, 3 stated that they lost interest in the program, 2 had worsening medical conditions (including rapid progression of dementia in 1 case), 2 died, and 2 withdrew for other reasons. Sixteen additional persons completed baseline testing but did not begin the intervention (eg, disenrolled because of health issues, n = 9) or enrolled too late for follow-up to be completed (n = 7).
The active cases and the withdrawers did not differ significantly on demographics, baseline Functional Assessment Staging of Alzheimer’s Disease (FAST)/Global Deterioration Scale (GDS), quality-of-life (QoL) scores, or physical fitness measures (Ps > .15). Compared to those who completed the first follow-up, withdrawers had a lower mean MMSE score at baseline (19.44 vs 22.72, P = .029) and tended to have higher mean depression scores (9.06 vs 6.54, P = .085). The 16 additional participants who did not begin the intervention or who enrolled too late for follow-up had higher mean baseline depression scores (9.80 vs 6.54, P = .026) and lower mean baseline QoL ratings (35.60 vs 39.79, P = .045) compared to those who completed the first follow-up, but there was no differences between these subgroups in initial MMSE scores, FAST/GDS scores, or physical fitness measures.
First Follow-Up
The mean number of exercise plus language stimulation sessions prior to the first follow-up was 27.45 (SD = 9.77, range = 4-42), and the mean number of social or volunteer outings was 6.86 (SD = 9.14, range = 0-28). Exercise plus language sessions included an average of 17.74 (SD = 10.97, range = 5.60-50.93) minutes of endurance exercise, 9.33 (SD = 1.97, range = 5.00-12.65) minutes of strengthening exercise, 9.97 (SD = 2.56, range = 5.42-13.53) minutes of flexibility training, and 21.06 (SD = 8.24, range = 5.89-46.79) minutes of language stimulation. Four participants reported exercising on their own or with their caregivers in addition to their sessions with LEEPS volunteers. Ten participants had no study-related social outings due to limitations in the availability of trained volunteers, and only 5 engaged in volunteer activities as part of the socialization component of the intervention.
Table 1 summarizes baseline and initial follow-up scores on measures of global mental status, depression, quality of life, physical fitness, and cognition and language. In general, scores remained stable over time. The only statistically significant differences at baseline versus follow-up on standardized outcome measures were an increase in number of arm curls (t = 2.61, df = 28, P = .015, 95% confidence interval (CI) = 0.48 to 4.00) and a decrease in Quality of Life in Alzheimer’s Disease scale (QoL-AD) ratings (t = −2.09, df = 26, P = .048, 95% CI = −0.40 to −5.15).
The modal change in the MMSE was a 1-point improvement, and there was no significant change in mean MMSE scores (t = 0.35, df = 27, P = .731, 95% CI = −0.99 to 1.23). However, 25% of the participants improved on the MMSE by 2 or more points, compared to 15% who declined by that amount. At baseline, 61% of participants scored 23 or lower on the MMSE (a range commonly associated with dementia), compared to 39% at retest. As a secondary analysis, an expected MMSE score at first follow-up was computed by subtracting the mean annual rate of decline (−3.3 points) observed in a meta-analysis of longitudinal studies of persons with AD 21 from the baseline score; the observed mean MMSE at follow-up (22.64, SD = 5.48) was significantly greater than the expected mean MMSE score (19.16, SD = 5.07) calculated in this manner (t = 6.76, df = 27, P < .0001, 95% CI = 2.42-4.53).
There was no change in depression symptom scores. All participants with data on the depression questionnaire scored in the normal or mildly depressed range at baseline, compared to 96% at the first follow-up. On the QoL scale, although the median change was a 1-point decline and two-thirds of the sample improved, remained stable, or declined by less than one-half of a SD, there were 3 individuals whose QoL-AD scores declined by 12 or more points, equal to 2 or more SDs. When the analysis of variance was repeated with these 3 cases excluded, the change from baseline to first follow-up was no longer significant, suggesting that these individuals with unusually sharp declines contributed disproportionately to the downward trend for the group as a whole.
There was a marginally significant decrease in the chair-stand test (t = −1.91, df = 27, P = .067, 95% CI = −1.71 to 0.06) but no significant change in the 2-minute step test. One participant was unable to complete either the chair-stand or step tests due to instability and fear of falling.
As an index of success in implementing the physical exercise component of the intervention, we compared the average duration of endurance exercise in the first month of the intervention to the month with the longest mean duration of endurance exercise prior to the first follow-up. This is similar to a procedure used by Arkin 15 to compare baseline versus best endurance duration findings in the Elder Rehab sample. For LEEPS participants, there was a highly significant increase in the amount of time they performed endurance exercises in their initial month compared to their best exercise month prior to the first follow-up (mean = 14.23 ± 8.04 minutes and 31.29 ± 22.52 minutes, respectively; t = 4.73, df = 28, P < .0001, 95% CI = 9.68-24.45). All participants showed some increase in endurance exercise duration as the intervention progressed. In the first month, 7 (24.1%) participants averaged 20 minutes or more of endurance exercise across sessions, compared to 17 (58.6%) participants with this average level of endurance exercise during the peak performance month.
Performance was stable on standardized tests of cognition and language with the exception of a decreasing trend in the number of false-positive errors on word list recognition at follow-up (t = −1.99, df = 26, P = .057, 95% CI = −1.13 to 0.02). Two participants declined to attempt word list learning at baseline.
With n = 29 at follow-up and α = .05, this study could detect paired difference effect sizes between .47 and .56 with 80% to 90% power.
Second Follow-Up
Eight participants were scheduled for a second follow-up assessment. The mean interval from first to second follow-up was 8.64 months (SD = 2.55, range = 5.72-12.02), and the mean interval from baseline to second follow-up was 20.87 months (SD = 2.80, range = 17.51-26.15). One individual could not comprehend instructions at the second follow-up, leaving data for 7 participants. Participants with 2 follow-ups did not differ significantly (Ps > .20) from those with a single follow-up on demographics, baseline FAST/GDS, or baseline MMSE, depression, QoL, or physical fitness scores.
The mean number of exercise plus language stimulation sessions between the first and second follow-ups was 19.00 (SD = 6.53, range = 13-32), and the mean number of social or volunteer outings was 4.28 (SD = 6.32, range = 0-18). Exercise plus language sessions included an average of 24.19 (SD = 18.17, range = 9.76-58.78) minutes of endurance exercise, 9.14 (SD = 2.55, range = 5.38 – 12.31) minutes of strengthening exercise, 10.89 (SD = 2.06, range = 7.78-13.44) minutes of flexibility training, and 26.50 (SD = 9.19, range = 16.63-40.19) minutes of language stimulation. Two participants had no study-related social or volunteer outings due to limitations in the availability of trained volunteers.
Table 2 shows results from the 3 test occasions. There were no statistically significant differences between baseline scores and performance at the second follow-up on measures of cognition, physical fitness, or well-being (Ps ≥ .15). Similarly, mean minutes of endurance exercise at the peak month during the second intervention year did not differ significantly from average minutes of endurance exercise during the initial month of the intervention (34.38 vs 18.06, respectively). At the second follow-up, with n = 7 and α = .05, this study could detect only large paired difference effect sizes (1.1- 1.3) with 80% to 90% power.
Results for 7 Participants With 2 Follow-Ups.
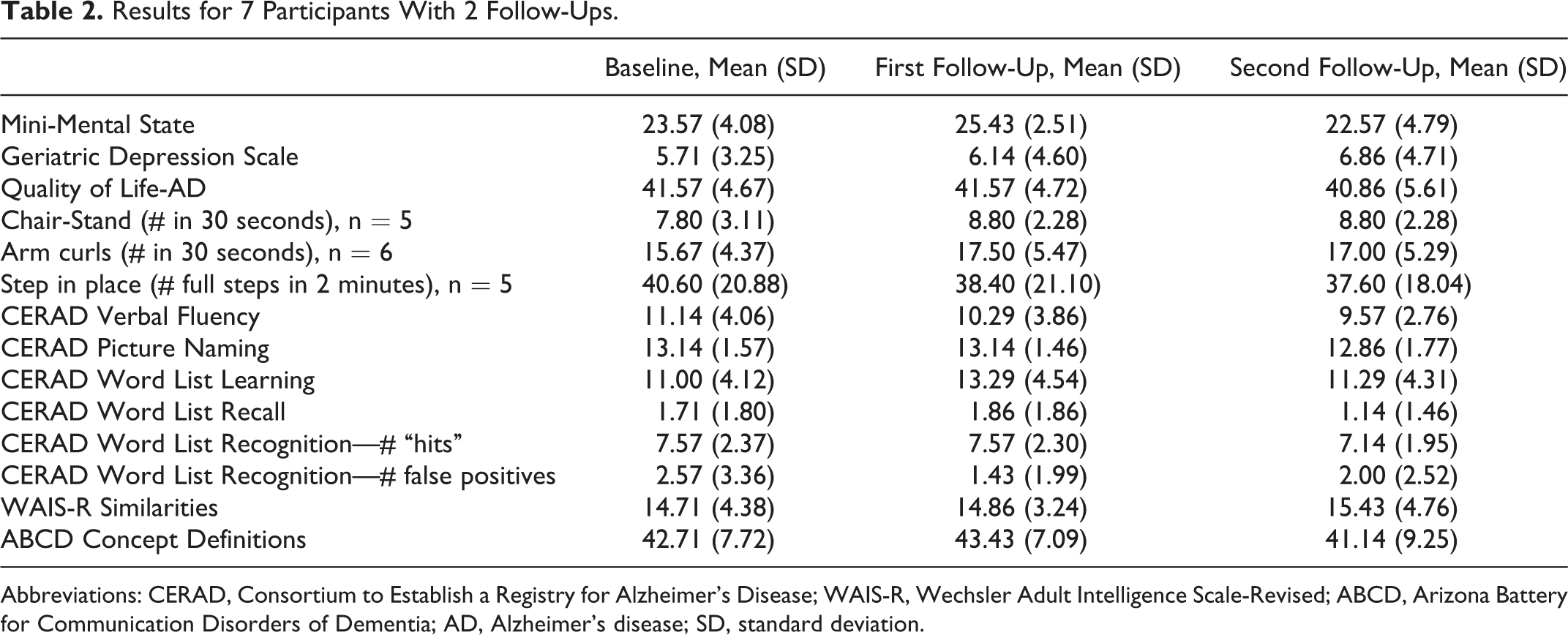
Abbreviations: CERAD, Consortium to Establish a Registry for Alzheimer’s Disease; WAIS-R, Wechsler Adult Intelligence Scale-Revised; ABCD, Arizona Battery for Communication Disorders of Dementia; AD, Alzheimer’s disease; SD, standard deviation.
Discussion
The LEEPS participants generally remained stable in cognitive function, mood, and physical fitness through an initial follow-up at nearly 11 months. A small subgroup that completed a second follow-up at an average of 20 months continued to perform near baseline levels. The minimal levels of observed decline are potentially noteworthy, given the progressive nature of AD and related dementias included in the LEEPS sample.
The aim of LEEPS was to translate the Elder Rehab program, a university-based research intervention, for application in rural communities. Although modifications in some procedures were required for application to a new population and setting, outcomes for LEEPS and Elder rehab were similar in many respects. The current project is an initial step in addressing the critical need to translate results from research trials to everyday practice in community settings, with the goal of enhancing the adoption of best practices to improve the lives of older persons with early-stage dementia.
In LEEPS, the negligible changes in MMSE scores observed at first and second follow-ups (mean = +0.18 and −1.0 points, respectively) compare favorably to the estimated annual rate of decline of 3.3 points reported in a meta-analysis of studies focused primarily on mild to moderate AD. 21 In the Elder Rehab Program, MMSE scores declined an average of 2.9 points in the first year and 5.1 points from baseline to the second year, 1 which was less than the average 2-year decline in the Consortium to Establish a Registry for Alzheimer’s Disease sample used for normative comparison. 20 A similar pattern was noted on other standardized cognitive tests. For example, 1-year completers in the Elder Rehab Program had statistically significant declines in performance on several of the additional cognitive measures, whereas in LEEPS, there was little change in other cognitive measures at either follow-up.
The absence of decline in LEEPS on mean MMSE scores cannot be attributed to higher baseline performance compared to Elder Rehab, but the slightly shorter retest intervals and greater attrition in LEEPS could have contributed to these results. The fact that cognitive assessment batteries only partially overlap between the 2 studies limits more specific outcome comparisons, and the small number of participants reduced statistical power in both investigations. Nonetheless, the main cognitive message of LEEPS is relative stability in performance up to an interval of nearly 2 years, which is not the usual longitudinal outcome for persons with ADRD. Moreover, the LEEPS translation appeared to have at least as much effect on cognitive performance through 2 rounds of follow-up as the original Elder Rehab program.
Regarding physical fitness, the LEEPS intervention succeeded in increasing participants’ duration of endurance exercise, paralleling similar findings for the Elder Rehab. 15 These are encouraging outcomes, in light of exercise research documenting that activities that increase heart and respiration rates have the most pronounced benefit for brain function and cognitive performance. 5 Another important finding observed in both the original study and the present translation was the absence of exercise-related injuries. This is especially noteworthy in LEEPS, where a substantial portion of the participants had compromised gait or balance and other physical limitations common among persons with dementia and advanced age. Securing input from a physical therapist about individuals’ exercise plans and developing options for seated exercises were among the steps taken in LEEPS to minimize the risk of falls or other injuries.
Limitations and Strengths
There are important limitations in this study. As a translational project focused on intervention, there was no control or comparison condition, and we cannot conclude that stability or improvement in outcomes over time is attributable to the intervention. The sample was relatively homogenous demographically, and findings may not be generalizable to other groups with differing characteristics. The high attrition rate also limits conclusions, although it should be noted that attrition was generally due to circumstances other than loss of interest in the program (eg, worsening health of the participant or caregiver or entry into long-term care). The fact that the sample was limited to persons with mild levels of dementia is an additional and important restriction that may have contributed to the minimal decline observed at the initial follow-up. Finally, in some cases, project staff members who performed the baseline and follow-up assessments also provided the activities intervention, which could potentially have biased outcomes. Assessments were standardized, however, so opportunities for bias were minimized.
A notable strength of the project was its implementation in a rural underserved region, where community supports for persons with dementia were nonexistent or very limited. The project also successfully adapted the original protocol to increase its feasibility and appropriateness for this population (eg, incorporated nonstudent volunteers and developed structured exercise regimens suitable for in-home use). Our translation also shared the strengths of Elder Rehab, including activities that are simple and easy for volunteers to learn, promote social interaction, and are engaging and enjoyable for participants.
Translational Challenges and Looking Ahead
The LEEPS intervention was a translation, not a replication, of the Elder Rehab program. Procedures were adapted to local circumstances and needs while retaining as much of the original assessment and intervention methods as possible. The LEEPS sample was primarily rural as opposed to urban and included a wider range of progressive dementias than Elder Rehab, which was restricted to persons with AD. The great majority of LEEPS participants elected to exercise at home, in a variety of ways, whereas exercise sessions in the Elder Rehab Program were conducted at a university rehabilitation gym with standard equipment. Although all volunteers in the Elder Rehab Program were undergraduate students who received course credit for participating, LEEPS engaged a more diverse set of volunteers, including retired persons and working adults in addition to students. In LEEPS, intervention programming was provided on an ongoing basis, with gaps due to illness, vacations, inclement weather, schedule conflicts, and so on, whereas in Elder Rehab, 2 semesters of activities constituted a year’s worth of intervention. Finally, the total amount of intervention programming varied more widely between participants in LEEPS than it did in Elder Rehab. The main factor that affected compliance with the program was limited availability of volunteers, which reduced the number of social and volunteer outings below the initially planned level. Each of these procedural differences could potentially affect outcomes (eg, fewer social outings may have curtailed benefits for mood or perceived quality of life). Nonetheless, LEEPS preserved the multifaceted, volunteer-assisted intervention model of the Elder Rehab Program, used many of the same assessment tools, and implemented longitudinal retests as close as possible to the original schedule. For both programs, it is important to recognize that the multi-modal nature of the intervention, while a potential strength in terms of overall impact, makes it difficult to determine whether certain elements of the intervention have greater effects than others.
There were several notable challenges to implementing this relatively intensive activity-focused intervention. Foremost among these challenges were difficulties in recruiting enough volunteers and problems with matching locations of volunteers and LEEPS participants. Rural and minority communities may rely more heavily than urban centers on face-to-face familiarity as a basis for becoming involved, and, as a result, stimulating interest in new volunteer opportunities may proceed slowly. As LEEPS progressed, greater numbers of potential volunteers expressed interest, and at times, there were trained volunteers but no study participants within a reasonable driving distance. Although maintaining an adequate volunteer base is likely to remain a challenge in the future for similar programs, the advantages of a volunteer-based intervention (eg, benefits to volunteers as well as program recipients 1 and potential cost-effectiveness) must be kept in mind, and results of the Elder Rehab Program, LEEPS, and other programs for older persons with cognitive changes demonstrate that volunteers can be effective providers of educational and activities interventions. 22,23 A second important challenge faced by LEEPS was recruiting minority participants. Outreach efforts were varied and sustained, but minority enrollment was smaller than we had hoped. Hiring volunteer coordinators from minority backgrounds and continuing outreach for extended periods of time may help in achieving more representative samples in the future. Another challenge that was only partially met in LEEPS was identifying options for volunteer work that are meaningful and appropriate for older participants with dementia, particularly in rural settings where there may be fewer volunteer programs. Improving on this may require changing perceptions in communities about the preserved skills and contributions of older persons with early-stage dementia, in addition to developing databases of organizations in each community that welcome and encourage volunteers. Minimizing attrition was a final ongoing challenge. In future studies, shortening the interval for reassessments could provide more complete outcome data, provided that control or comparison data are available for interpretation. Further research comparing LEEPS and similar programs with usual care or other types of intervention is needed to establish the utility of individualized activities-based approaches for supporting persons with early-stage dementia in the community. It will be important to determine whether interventions like LEEPS extend the time that persons with dementia can safely and beneficially remain in their homes. A recent study from Minnesota has estimated that a systematic program of supportive counseling for caregivers would result in an additional 5% of persons with dementia being able to remain in the community over a 15-year period, with an associated cost savings of 100 million to 2.64 billion statewide. 24 We do not know yet whether community-based programs such as LEEPS, provided directly to persons with early-stage dementia, would have similar projected benefits, once efficacy has been more clearly established.
Footnotes
Appendix A
Acknowledgments
This project was supported in part by grant number 90AE0346 to the Wisconsin DHS from the US Administration on Aging, Department of Health and Human Services, Washington, DC 20201. Grantees undertaking projects under government sponsorship are encouraged to express freely their findings and conclusions. Points of view or opinions do not, therefore, necessarily represent official Administration on Aging policy. We thank the following individuals and organizations for their advice on study procedures or assistance with recruitment and implementation: Sharon Arkin, PhD, Kathie Duschene, BS, Dana MacFarlane, BS, Susan Price, Suanne Zimmerman, BS, Stephanie Hafez, BS, Todd Nierman, PT, DPT, CSCS, Sarah Riedeman, BS, Becky Dahl, BS, CSW, Mary Mezera, BS, Mary Frederick, BS, MS, the Aging and Disability Resource Centers of Eagle Country and Southwest Wisconsin, the Alzheimer's Support Center, the Wisconsin Alzheimer’s Institute at the University of Wisconsin-Madison, the Greater Wisconsin Agency on Aging Resources, and the Alzheimer's and Dementia Alliance of Wisconsin. We especially thank LEEPS participants and volunteers for their time and efforts.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by grant number 90AE0346 from the US Administration on Aging, Department of Health and Human Services, Washington, DC 20201.