
Abstract
We examined whether grounded optimism and external locus of control are associated with admission to dementia day care centers (DCCs). A total of 130 informal caregivers were recruited from the Alzheimer’s Association in Salamanca (northwest Spain). All caregivers completed an assessment protocol that included the Battery of Generalized Expectancies of Control Scales (BEEGC-20, acronym in Spanish) as well as depression and burden measures. The decision of the care setting at baseline assessment (own home vs DCC) was considered the main outcome measure in the logistic regression analyses. Grounded optimism was a preventive factor for admission (odds ratio [OR]: 0.34 and confidence interval [CI]: 0.15-0.75), whereas external locus of control (OR: 2.75, CI: 1.25-6.03) increased the probabilities of using DCCs. Depression mediated the relationship between optimism and DCCs, but this effect was not consistent for burden. Grounded optimism promotes the extension of care at home for patients with dementia.
Introduction
There are approximately 600 000 people with dementia (PWD) in Spain, and families are an essential part of the provision of care. 1 –3 The challenges associated with providing care for PWD are particularly demanding, and therefore, caregivers who take on the responsibility of caring PWD usually show high rates of burden, depression, and decreased quality of life. 4 In this context, adult day care centers (DCCs) for PWD are conceived as out-of-home social-health services to delay long-term institutionalization, providing caregivers time away from their care responsibilities to help reduce levels of caregiving-related stress and to restore their own well-being. 5 –7 Essentially, the organization and publicizing of these programs for PWD in Spain are carried out from Alzheimer Associations, but commonly, day care programs for PWD are scarcely used. 6 –11 In fact, caregivers’ decision to use specialized DCCs for PWD is made late and probably reflects a preliminary step toward placement. 9
Different factors have been proposed to explain low use of community services. Patients’ refusal, caregivers’ lack of knowledge or negative beliefs about the outcomes, feelings of guilt, possibilities of using paid help, doubts about recipients’ safety, and stigmatization of services are some of them. 3,6,10,12,13 Additionally, wives of care recipients use adult day care less and also delay their use 14,15 ; therefore, patients usually show a clear impairment in the first place. 16,17 However, the relevance of some factors, such as burden, as determinants of using day care services seems controversial. 14,17 Interestingly, some caregivers do not use support services mainly because they are unaware of the need for their use. 11 In this regard, Andersen’s health service use model 18 claims that perceived need is the most immediate cause of health service use.
Following the argument of this model, Robinson et al 14 suggested that caregivers who usually feel strong enough to cope with the caring situation keep the patients at home for a longer time. In contrast, low perceived control over life circumstances may result in poor adaptation, leading to seeking community help. These explanations are consistent with the relationship between generalized beliefs of control, 19,20 stress response, and coping. In this area, Pearlin et al 21 proposed a conceptual model for Alzheimer caregivers’ stress. Briefly, they considered the existence of objective (eg, care recipient’s problematic behavior) and subjective (eg, overload) indicators related to primary stress, which directly influence the intrapsychic strains (eg, mastery or self-esteem). These intrapsychic strains mediate the relations between caregiving primary stress and negative outcomes (eg, depression). Importantly, these intrapsychic constructs would be genuine strains when they focus on the negative aspect (ie, reduced sense of personal mastery), but they could also be positive, a psychological resource (ie, high personal mastery), for coping with stress.
Considering the situation of caring for a PWD, primary objective stressors (eg, severity of dementia) are more difficult to modify, and they explain less variance in burden than caregivers’ subjective factors. 22,23 Consequently, studies focusing on caregiver-related stress and the protective role of some psychological resources in the negative consequences of caring for a PWD have awakened increasing interest. 24 Diverse studies have claimed that positive psychological resources related to the concepts of control (eg, mastery, self-efficacy, and resilience) and optimism (eg, expectancies of outcomes) play an important role in the management of the adverse effect of stress (eg, depression and burden) on caregivers’ well-being. 23,25 –28 Exceptionally, some control-related psychological resources, such as sense of mastery, resilience, and self-efficacy, have been associated with placement. 29 –32 However, the association between generalized expectancies of control (GEC; “beliefs of control oriented toward the future”) and the use of community-based services for PWD has not yet been explored.
The current study is based on the integrated, multidimensional approach to GEC proposed by Palenzuela 33,34 : (1) self-efficacy (the belief in one’s ability to perform actions and to function effectively in a challenging environment that demands one’s personal skills); (2) contingency or internal control (the personal belief that whatever happens will be the result of one’s own actions); (3) success or outcome expectations (the subjective estimation of the probability of achieving a desired goal or outcome); (4) helplessness or no-contingency (the belief that there is no relationship between the occurrence of events and one’s actions); and (5) luck or chance (the extent to which one expects that the events of one’s life are the result of random or chance factors). In summary, these expectancies are clearly different from a theoretical point of view, but they can be combined exceptionally in 2 higher order constructs such as grounded optimism (self-efficacy, contingency, and success) and external locus of control (helplessness and luck).
This perspective states that optimism is conceived as a multidimensional construct composed of 3 positive expectancies derived from the theories of Bandura 35 and Rotter, 36 rather than 1 unidimensional dispositional construct supported primarily by Rotter’s expectations of success or outcomes. 37 Thus, grounded optimism 38,39 is defined as the conviction of being able to exercise control (self-efficacy component) in an environment perceived as controllable (contingency component), which supports expectations of goal achievement (success or outcome component). A remarkable feature of this optimistic perspective is “keeping one’s feet on ground,” which should be differentiated from others such as unrealistic optimism 40,41 and naive optimism. 42 In comparison with Pearlin’s model of stress and control, 21 this approach allows us to differentiate between the locus of control (internal vs external) and the self-efficacy components as opposed to the global construct of mastery.
This study examines the relationship between optimism and external locus of control in the decision to use an adult DCC for PWD. It is known that optimism could buffer the negative effects of stress, such as burden and depression, but the relevance of these factors in relation to the use of community services for PWD needs to be investigated. Thus, a possible mediator effect of burden and depression on the relationship between GEC and admission in the DCC is still unclear. Finally, the relevance of factors related to the characteristics of caregivers, the relationship with the patient, and the caring context is discussed.
Methods
Participants
A sample of 130 family caregivers (mean age = 58.62 ± 12.45, 36 males and 94 females) and their respective patients (mean age = 77.96 ± 6.02, 48 males and 82 females) was recruited from consecutive referrals to the local Association of Family Members of Patients with Alzheimer’s Disease (AFA, Salamanca, Spain). Informal caregivers who visited AFA (from January to December 2009) because they were interested in specific adult day programs were invited to participate in the study. All caregivers volunteered to participate in the study. Their role was that of primary caregiver, taking on responsibility for any decisions and for the patient’s well-being. Once they were informed about the aims of the study, written informed consent was obtained from all the participants. This study was a part of a research project funded by the Local Government (Junta de Castilla y León). The board of the AFA (Salamanca) approved the study.
All care recipients met the criteria for the diagnosis of dementia, 43 which was corroborated by the general practitioner, and they were susceptible to receiving assistance in the DCC of AFA Salamanca. The selected caregivers were living in the province of Salamanca (northwestern Spain), and their native language was Spanish. A 6-month period of caring was considered an inclusion criterion for the participants. Importantly, none of the caregivers were receiving specialized psychological support at the time of assessment, and they were living at home with the patient. Prior use of day care was an exclusion criterion for participation in the study.
The interview with the caregivers was performed in one session divided into 2 parts: (1) a questionnaire of sociodemographic characteristics and (2) a psychological protocol. The assessment of family caregivers was conducted by qualified psychologists from AFA who were blind to objectives of the study. Once the caregivers had completed the assessment, they were stratified into 2 groups according to the decision they made at the baseline measurement: home care (n = 60) versus voluntary admission in the DCC (n = 70). The AFA Salamanca is a local entity with a limit of 70 places in the DCC. For this reason, participants who had selected admission but who could not enter the DCC at baseline measurement were included on a waiting list. At this time, it was confirmed that a professional from AFA would contact them in less than 6 weeks for admittance in the center. Importantly, waiting list participants who changed their minds for any reason during this interval (eg, rejection, change of address) or who requested admission in the home care group were excluded from this study. Rejection of DCC services did not have any influence on participation in future programs provided by AFA Salamanca.
Measures
Information obtained about PWD included age, gender, education, type of dementia, and time since the diagnosis. In addition, all patients completed a standard neuropsychological assessment protocol. Dementia severity was established according to the clinical dementia rating (CDR) scale (CDR-1 = mild, CDR-2 = moderate, and CDR-3 = severe). 44 The Mini-Mental State Examination, 45 the Barthel Index, 46 and the Neuropsychiatric Inventory Questionnaire 47 were used to assess the patients’ cognitive status, functional impairment, and psychopathological symptoms, respectively.
The caregivers’ questionnaire obtained data about their sociodemographic characteristics (age, sex, and education) and situational factors (relationship with the patients and duration of caregiving). Additionally, the following standardized measures were included in the survey questionnaire.
The Zarit Burden Interview
This instrument (22 items) was used to measure caregivers’ perceived burden in diverse domains. 48 The scale was validated for the Spanish population 49 with acceptable internal reliability (Cronbach’s α), ranging from .69 to .90. Score responses ranged from 0 (never) to 4 (almost always) to prevent discrepancies with the original scale scores. Total scores range between 0 and 88 points, with higher scores reflecting higher caregiver burden.
The Goldberg Anxiety and Depression Scale
For this 18-item instrument, 9 addressing depression and 9 addressing anxiety, respondents indicate how they felt during the past 2 weeks (response format = yes/no; range = 0-18 points). 50 The optimal cutoff points for the anxiety (4 points) and depression (2 points) scales were established for the Spanish version by Montón et al. 51 Overall specificity and sensibility were over 80% in the Spanish population.
The Battery of Generalized Expectancies of Control Scales
This instrument was designed based on Palenzuela’s approach to personal control. 34,52,53 The Battery of Generalized Expectancies of Control Scales (BEEGC) includes 20 items distributed in 5 GEC-related scales (contingency, self-efficacy, success, helplessness, and luck). Respondents rate their degree of agreement with each statement on a 9-point Likert-type scale ranging from 1 (totally disagree) to 9 (totally agree). Independent scores are obtained by adding the items contained in each scale, which are positively formulated (eg, high scores on each dimension represent higher saturation in this construct). Although each dimension measures different theoretical concepts, we combined the scores to study the targeted psychological constructs as follows: (1) grounded optimism (self-efficacy, contingency, and success; range = 3-27) and (2) external locus of control (helplessness and luck; range: 2-18).
Palenzuela et al 33 confirmatory factor analysis showed that all the items of the BEEGC-20 loaded above .40 (except for 3 with loadings of less than .30) in a 1-factor model, but model fit was unsatisfactory. In contrast, all items achieved high weights and good fit in a 5-factor model. The correlations between the scales that make up grounded optimism were efficacy-success (r = .62), contingency-success (r = .69), and efficacy-contingency (r = .35). Similarly, external locus of control components (helplessness and luck) showed a correlation of .42. Therefore, the scales assess different theoretical constructs, but higher order constructs related to positive (eg, grounded optimism) or negative control expectations (eg, external of locus of control) can be obtained by calculating composite scores.
Statistical Analyses
Statistical analyses were performed with SPSS software, version 19.0 for Windows. The main outcome of interest was the decision of care setting at baseline (own home vs DCC). First, we compared all the variables using univariate analyses (t test or chi-square [χ2] test, depending on the measurement of the variable). Pearson’s correlation coefficient was calculated to test the associations between quantitative variables. In addition, multivariate logistic regression models (Enter Method) were used to analyze whether grounded optimism, external control, and depression are significantly associated with DCC. Sociodemographic (eg, caregivers’ age), situational variables of caring (eg, time of care and relationship), and burden were introduced as covariates. Finally, mediator effects of burden and depression in the relationship between optimism and DCC use were carried out following the Baron-Kenny method. 54 Level of significance was set at P ≤ .05.
Results
Characteristics of the Sample
Table 1 shows the characteristics of caregivers and PWD, stratified by the decision of care setting: care at own home (n = 60) versus DCC (n = 70).
Characteristics of the Participants: Means and Standard Deviations (in Parenthesis).
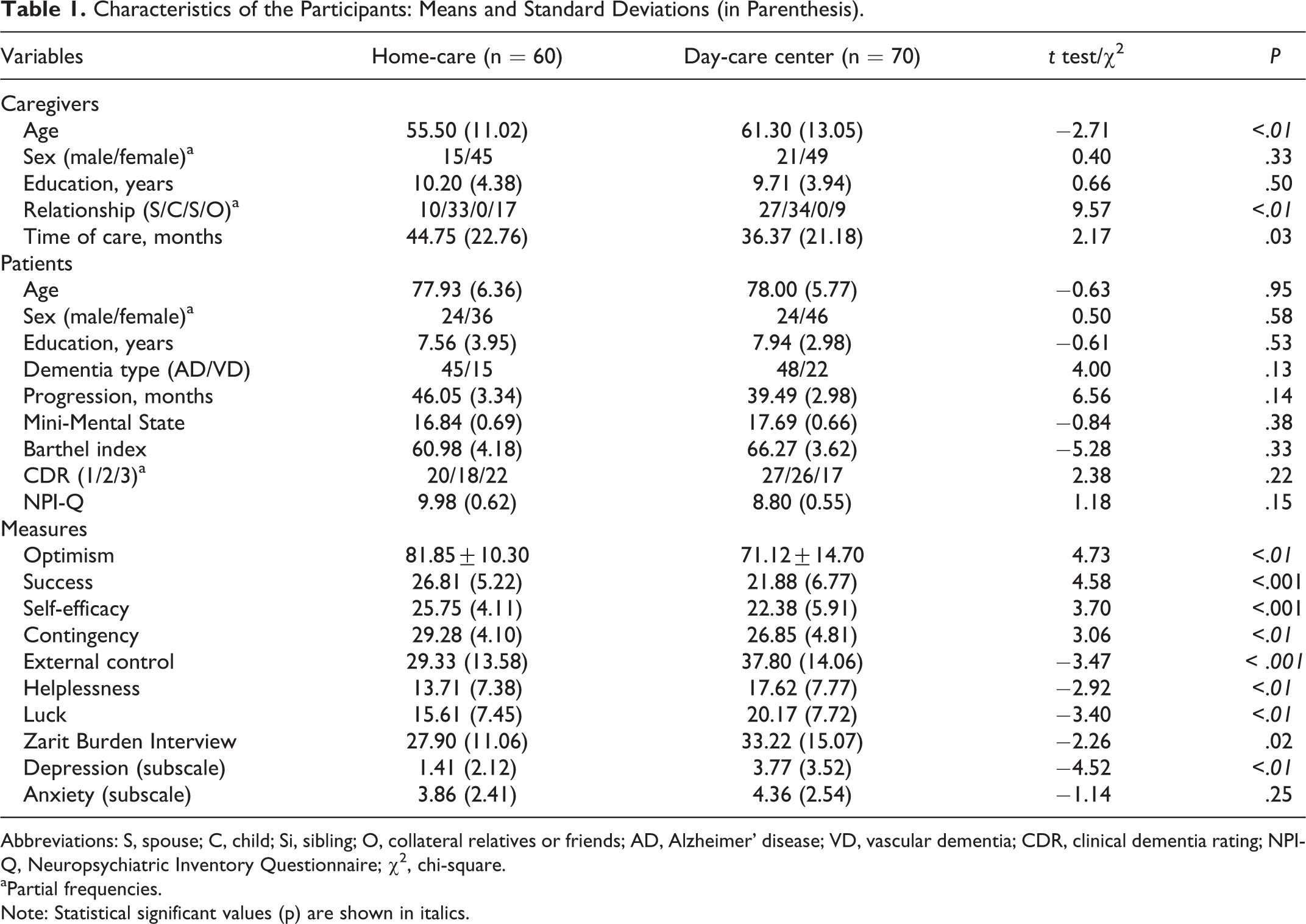
Abbreviations: S, spouse; C, child; Si, sibling; O, collateral relatives or friends; AD, Alzheimer’ disease; VD, vascular dementia; CDR, clinical dementia rating; NPI-Q, Neuropsychiatric Inventory Questionnaire; χ2, chi-square.
aPartial frequencies. Note: Statistical significant values (p) are shown in italics.
Student’s t tests for independent samples indicated that the DCC group was older than the home care group, but care duration (months) was shorter for the DCC group. Chi-square tests also showed that the DCC was used more frequently by spouses, but collateral relatives were more common in the home care group. No significant differences emerged (home care vs DCC) in care recipients’ clinical characteristics. Furthermore, caregivers from the DCC group scored significantly higher on external locus of control than caregivers from the home care group (group means = 37.80 ± 14.06 vs 29.33 ± 13.58, respectively, t = −3.47, P < .001). The DCC group also scored significantly higher on burden and depression. In contrast, the home care group scored significantly higher on grounded optimism (group means = 81.85 ± 10.30 vs 71.12 ± 14.70, respectively, t = 4.73, P = .001).
A positive correlation was found between time of care and grounded optimism (r = .23, P < .01), whereas caregivers’ age showed a positive correlation with external locus of control (r = .32, P < .01). Spouses scored significantly lower than other relatives on grounded optimism (group means = 71.32 ± 16.83 vs 77.96 ± 12.12, respectively, t = −2.51, P = .01).
Burden, Depression, and Expectancies of Control
Table 2 shows the correlations between the BEEGC components, burden, and depression.
Correlations Between Expectancies of Control, Depression, and Burden.

Abbreviations: E, efficacy; LCE, locus of external control.
aSignificant correlation, P < .01.
The dimensions of grounded optimism (self-efficacy, contingency, and success) showed negative relations with depression and burden.
Prediction of Assistance in the DCC
This section analyzes the relationship between predictors (optimism, external control, and depression) and the main outcome (home care vs DCC). Independent multivariate logistic regression models are shown in Table 3. Caregivers’ age, time of care, relationship with recipients, and levels of burden were introduced as covariates in all the models.
Logistic Regression Analysis for the Prediction of Home Care Versus Day Care Center.
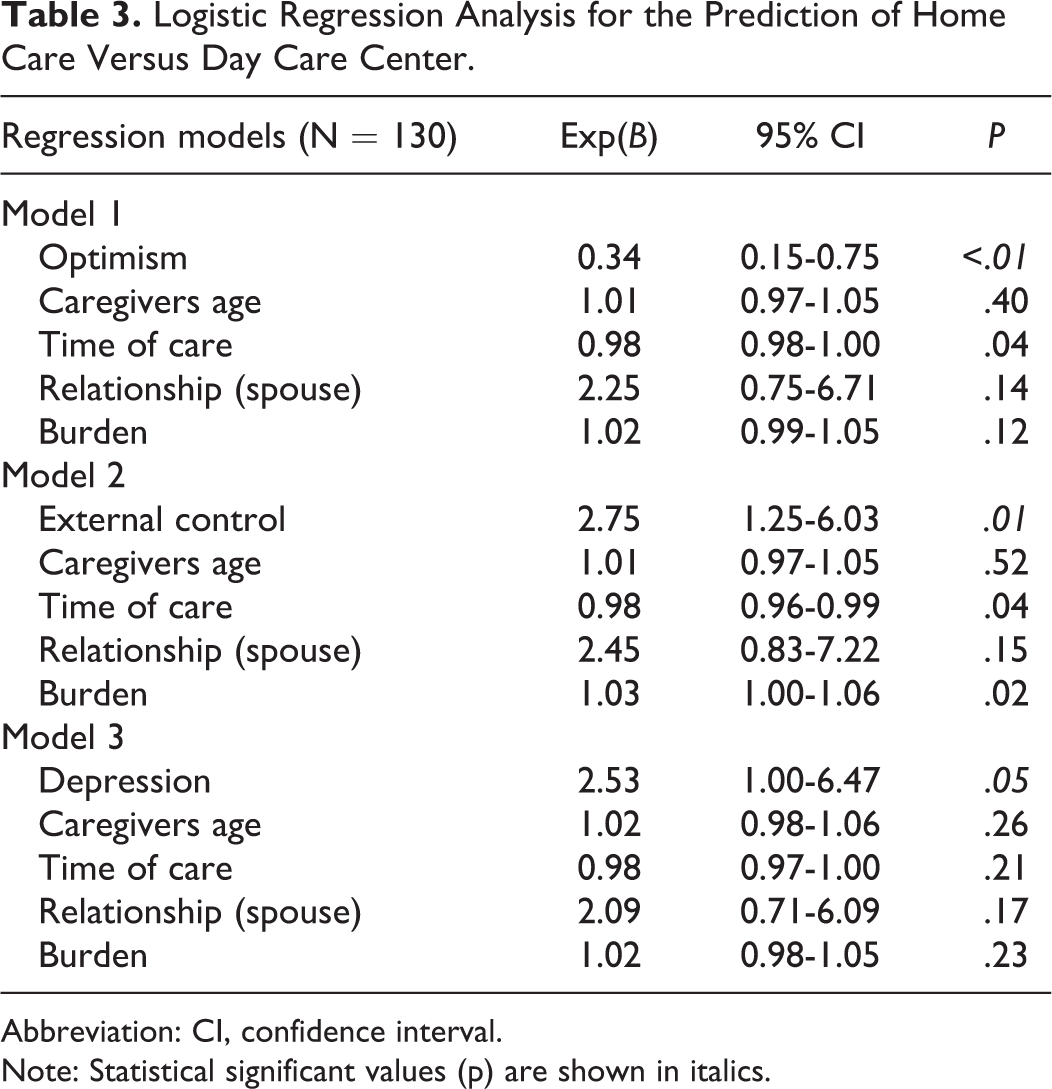
Abbreviation: CI, confidence interval. Note: Statistical significant values (p) are shown in italics.
Model 1 analyzed the relation between grounded optimism and admission in the DCC (χ2 = 26.80, degrees of freedom [df] = 5, P < .001), revealing that low scores on grounded optimism were significantly related to DCC use. External locus of control (model 2) was also significant (χ2 = 24.66, df = 5, P < .001); thus, higher scores on this construct were significantly associated with DCC use. Finally, model 3, in which depression (χ2 = 23.46, df = 5, P < .001) was introduced as a predictor, showed that higher scores on depression were linked to DCC use.
In brief, high scores on depression and external locus of control significantly increased the probability of using specialized DCC services for PWD, but grounded optimism was a preventive factor for admission. These effects were significant after controlling for significant covariates such as burden and time of care (models 1 and 2).
Depression and Burden as Mediation Factors
Previously, logistic regression analyses showed that grounded optimism, external locus of control, and depression were independent predictors of admission at the DCC (Table 3). In addition, burden was also related to DCC use (model 2).
The simple regression analysis model indicates that grounded optimism was related to lower scores on depression (F 1,128 = 263.19, P < .001) and burden (F 1,128 = 44.36, P < .001). Figure 1 shows (A) the relationship between grounded optimism and admission in the DCC and (B and C) the effect of grounded optimism on DCC use after including depression and burden. In summary, grounded optimism remained significant when burden was included in the model. However, the individual effect of optimism on admission was rendered nonsignificant (P = .06) after inclusion of depression as a mediator variable.
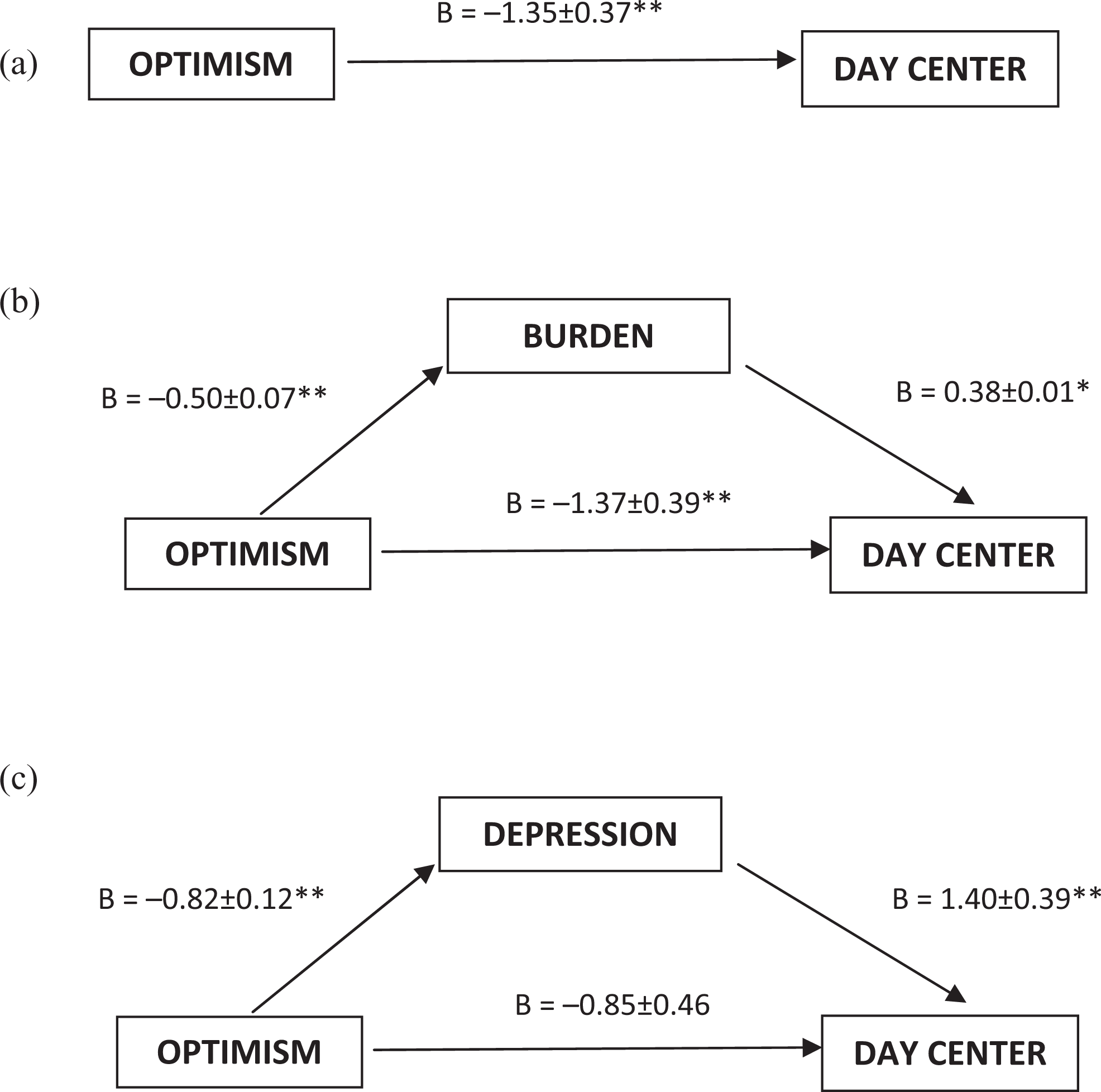
Depression and burden as mediator variables between optimism and day care center admission. A, shows the total effect of optimism on the outcome measure. B and C, depicts the effect of optimism after including mediators. B values represent regression coefficient ± standard error. *P ≤ .05 and **P ≤ .01.
Discussion
The main objective of this study was to examine the relationship between optimism and external locus of control with the use of community services for PWD. Focused on the multidimensional approach to GEC proposed by Palenzuela, 33,34 3 positive expectancies of control (self-efficacy, contingency, and success expectations) and 2 components of external locus of control (helplessness and luck) were combined to obtain the constructs of grounded optimism and external locus of control, respectively. These constructs have been compared to classical variables related to caregiver stress (depression and burden) as predictors of admission in adult DCCs in a sample of informal caregivers of PWD.
This research indicates that caregivers who used DCCs reported higher levels of burden and depression than home caregivers. Previously, burden and depression have been related to day care use and placement, 55,56 but this research adds some noteworthy results. Grounded optimism and external locus of control were independent predictors of admission to adult DCCs, even after controlling for various covariates such as burden. Thus, caregivers who decided to send their patient to the DCC obtained lower scores on grounded optimism and higher scores on external locus of control than caregivers from the home care group. Consistently, Robinson et al 14 suggested that caregivers who cope with the circumstances of care are less likely to use community services. Similarly, Infurna et al 30 indicated that loss of mastery in caregivers preceded the use of formal resources.
According to the caregiver stress model proposed by Pearlin et al, 21 it seems reasonable that psychological resources (secondary stressors) could influence the use of adult DCCs. Although this effect was independent of burden levels, depression showed a mediation effect in the relationship between optimism and the use of DCCs. Basically, this fact is explained by the strong negative relationship between depression and grounded optimism, which is consistent with the buffer effect of optimism on the negative outcomes of stress. 37,39 In brief, optimistic caregivers are less susceptible to experiencing negative emotions during care, 26 which indirectly prolongs care at home.
Contrary to what might be expected, external locus of control did not correlate with depression. In this sense, although helplessness has been proposed as an explanatory theory of depression, this term was originally coined to refer to a state of passivity and futility due to an unresponsive environment or consistently punished behavior. 57 This conceptualization failed to explain some symptoms of human depression (eg, low self-esteem), so the notion of personal helplessness 58 emerged as a change from the original connotation toward a sense of low self-efficacy. In fact, the helplessness component of the BEEGC-20 was designed to assess its original connotation that seems to trigger an angry response, rather than depression that emerges from a low sense of self-efficacy. 35,59 This fact is crucial to the absence of correlation between depression and helplessness in the present study. Therefore, a distinction should be made between personal helplessness (efficacy-based futility) and environmental helplessness (unresponsive environment-based futility), which are connected to singular emotional responses and therapeutic strategies, respectively. This is consistent with the arguments of Bandura and other authors. 35,59
Beyond the importance of subjective (eg, burden) and objective stressors (eg, behavioral disturbances) in the use of community services, this study highlights the importance of GECs for care setting. Although adult DCCs are usually resorted to late in the course of dementia, when individuals are more impaired, 15 in this study, care recipient characteristics were similar at baseline. Therefore, primary stressors do not necessarily predict the use of DCCs, which depends on multiple interactive factors, 12 –15 and its role can be influenced by other variables, such as caregivers’ psychological resources related to control. 14,30
It should also be noted that DCC use was related to some sociodemographic variables. Caregivers who decided to request formal assistance were older than those from the home care group. In addition, less time of care was also related to the use of DCCs. Indeed, other studies have also reported that age is related to negative experiences of care and to the request for institutionalization. 55,60 In addition, some authors have found that longer time of care can benefit adapting to the important challenges of caring for a PWD. 61 In this regard, our study also showed positive correlations between time of care and grounded optimism, whereas caregivers’ age correlated with external locus of control. These observations may indicate some changes in control beliefs concerning age-related decline, 62 and the adaptive capacity of some caregivers to the stressful situation. As both the correlations were weak, these interpretations should be taken with some cautions.
This research has some limitations. First, sample size and sociodemographic characteristics limit generalization to some extent. Our sample had not graduated from high school on average, as it seems that less than one-quarter of informal caregivers go beyond secondary school in Spain. 63 Considering that the decision to use community services is complex, other factors such as economic limitations of the families or stigmatization of formal resources for elders may also influence the use of services. Therefore, possible interaction effects between GECs and other explanatory factors related to the use of DCCs promise further research. Finally, the assessment of external locus of control was not exhaustive, so other beliefs such as powerful others or fate (or fatalism) should be explored in the future.
Conclusion
Grounded optimism and external locus of control are related to the use of specialized community services for PWD. Grounded optimism buffers the emergence of caregivers’ depressive symptoms and burden, which were also linked to the use of DCCs. This multidimensional approach to optimism (contingency, self-efficacy, and success) should be useful to develop multicomponent therapies aimed at strengthening informal caregivers’ personal resources for coping with the caring situation. The final aim would be to improve the family’s quality of life and delay the institutionalization of PWD.
Footnotes
Acknowledgments
The authors thank the Velum Foundation and the Association of Family Members of Patients with Alzheimer’s Disease (AFA, Salamanca) for their collaboration in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by the Autonomous Government of Castilla y León (ref. SAN191/SA10/06).