
Abstract
Background:
Dementia constitutes a public health hazard in developing countries. The aim of this study was to evaluate the prevalence of dementia and its associated factors in older hospitalized patients.
Methods:
The participants of this cross-sectional study consisted of older patients admitted to medical wards in Rasoul-e Akram hospital in Tehran, Iran. Mini-Mental State Examination, Mini-Cog test, Geriatric Depression Scale, Activities of Daily Living-Instrumental Activities of Daily Living (ADL-IADL) scale, and socioeconomic questionnaires were used.
Results:
A total of 205 elderly inpatients were included. The mean age was 71.33 ± 7.35 years; 63.4% of the participants had normal cognitive function, while 36.6% had some degree of cognitive impairment. There was a statistically significant relationship between gender, age, number of children, and occupation and the prevalence of dementia.
Conclusion:
Appropriate cognitive screening of older patients upon admission to hospitals could help identify potential adverse events and enhance the quality of care for patients with comorbid dementia.
Introduction
According to the latest estimates from World Health Organization, the number of people aged 60 years and older has increased significantly in the recent years in most countries. In 2015, an estimated 901 million people were aged 60 or older. By 2050, this number is anticipated to reach 2.1 billion, accounting for 22% of the world population. 1 Globally, the number of elderly people is increasing more rapidly than any other age-group. 2 In Iran, similar to other developing countries, there have been considerable changes in the population’s age structure in the past few years, owing to constant fertility reduction and increased life expectancy. According to Iran’s 2016 national population and housing census, nearly 9.27% of the country’s population were aged 60 or older. It is expected that this age-group will comprise more than 20% of the population by 2020. 3
Aging can bring about several physical and mental health issues. More than 15% of adults aged 60 or older have a mental disorder. One of the most common mental disorders in this group is dementia, occurring in 5% of the world’s elderly population. 4 Dementia is a disorder that affects orientation, attention and concentration, memory, language, and executive function. This cognitive impairment usually comes after a deterioration in emotion and behavior. Alzheimer’s disease is the most common type of dementia that accounts for an estimated 60% to 80% of cases. Other types include vascular dementia, mixed dementia, dementia with Lewy bodies, and frontotemporal dementia. 5 Estimates of worldwide prevalence of dementia range from 0.3 to 1.0 per 100 people aged 60 to 64, growing significantly to 42.3 to 68.3 per 100 people older than 95 years. 6
Cognitive impairment of various severity is common among hospitalized seniors, yet the majority of such cases remain undiagnosed. 7 Older people are commonly admitted to the hospital, and a large number of them have dementia. 8 The prevalence of dementia in general hospitals has been reported to range from 2.8% to 63.0%. 9 There is evidence that admission of older adults with dementia and acute medical illness to hospitals is a critical event associated with high 6-month mortality rates. 10 Many older adults with dementia are hospitalized for diagnoses other than dementia. 11 This is while early diagnosis of dementia in elderly inpatients can allow them to receive appropriate support and treatment that may improve their cognition and enhance their quality of life. Undetected dementia places older patients at risk of delirium and medical complications. Furthermore, early detection of dementia provides an opportunity for the individuals to participate in advance care planning while still competent to do so. 12 There appears to be limited data on the prevalence and characteristics of patients with dementia, their medical and psychiatric comorbidity, and the effects of dementia on clinical outcomes, in the hospitals of Iran. In this regard, the aim of this study is to evaluate the prevalence of dementia and its associated factors in older hospitalized patients admitted to medical wards in a general hospital in Iran.
Method
Study Design
This was a cross-sectional hospital-based study carried out at the Rasoul-e Akram hospital, an affiliate of Iran University of Medical Sciences in Tehran, Iran.
Participants
The population included in the research consisted of older patients (aged ≥60) (note 1) admitted to Rasoul-e Akram hospital from October 2017 to March 2018. Rasoul-e Akram is a tertiary-level hospital which provides care to patients suffering from all types of medical condition. The study participants were selected by census sampling, and those who consented to participate in the research were enrolled in the study. Patients admitted to the departments of emergency, intensive care unit, and coronary care unit were not included. In addition, patients with psychotic and mood disorders admitted to the psychiatric ward were excluded. If participants had surgery within 8 hours prior to participation, met the delirium criteria of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), 13 and had altered levels of consciousness, or acute neurological or metabolic conditions, they were not eligible for the study.
Screening and Assessment
Demographic data
A sociodemographic questionnaire was devised by the researchers in order to collect data on age, gender, marital status, educational level, occupation, income level, number of children, history of medical and psychiatric disorders as well as medication and substance use.
Cognitive assessment
Initially, cognitive function was assessed using the Farsi version of the Mini-Mental State Examination (MMSE) and the Mini-Cog test. The MMSE is a 30-point screening tool measuring 5 cognitive domains including orientation to time and place, registration and short-term recall, language, concentration, and visual construction. This test was originally created by Folstein et al in 1975 to estimate the severity of cognitive impairment and can be administered in 5 to 10 minutes. 14 The Mini-Cog test is a rapid and brief cognitive screening instrument consisting of a 3-item recall test for memory and a scored clock-drawing test. This tool was initially developed by Borson et al in 2000 as a brief test for distinguishing individuals with dementia from non-demented ones in a community setting. A score of 3 to 5 out of 5 is a negative screen for dementia. 15 Both instruments have been shown to be valid and reliable among Farsi speakers. 16,17
Following the initial cognitive screening, patients scoring <26/30 on MMSE or <3 on the Mini-Cog test were subjected to further cognitive evaluation by a geriatric psychiatrist or a neurologist. The effects of education on performance in the MMSE was considered. A final diagnosis of dementia/major neurocognitive disorder was confirmed through a clinical interview based on criteria from the DSM-5. 13
Assessment of depression
Presence of depressive disorder was assessed using the 15-item short form Geriatric depression scale (GDS-15). The GDS is a self-reported questionnaire that is used to screen for clinical depression among older adults. The scale was first developed in 1982 by Yesavage et al. It consists of 15 questions about how participants have felt over the past week and is responded through a “Yes/No” format. In this scale, a total score of 0 to 4 is considered normal, whereas scores between 5 and 8, 9 and 11, and 12 and 15 denote the presence of mild, moderate, or severe depression, respectively. 18 In a study by Malakouti et al, the Farsi version of GDS showed satisfactory psychometric properties. 19
Assessment of functional status
A cross-culturally adapted version of the ADL-IADL scale was used to screen elderly respondents for functional status. This scale ranks the patient’s ability to perform the 16 functions of bathing, dressing, toileting, transferring, continence, feeding, ability to use the telephone, shopping, preparing meals, light house work, laundry, going to distant places using some form of transportation, getting around inside, performing minor repairs, responsibility for taking medications, and ability to manage finances. Spector et al examined the psychometric properties of this combined ADL-IADL scale in 1998 and reported on major advantages for this tool in measuring functional disability compared to scales based solely on IADLs or on ADLs. 20 Patients and their informants respond to the abovementioned items using a 3-point Likert-type scale. The total score varies from 0 to 30. A score of 13 or more depicts high functioning, 7 to 12 indicate moderate functional impairment, and 6 or less suggest low functioning. 21
Ethical Consideration
Ethical approval was obtained in accordance with the Helsinki Declaration. Written informed consent was obtained from all individual participants included in the study. This study was approved by the institutional review board of Iran University of Medical Sciences (Ref No: IR.IUMS.REC1395.8823215248). 22
Statistical Analysis
All statistical analyses were performed in SPSS ver. 23 (IBM, Chicago, Illinois), with the level of significance set at α = .05. As the data demonstrated a normal distribution, Student’s t test and analysis of variance were used for quantitative variables and the χ2 test for qualitative variables.
Results
Of the 205 elderly inpatients recruited, 109 (53.2%) were male and 96 (46.8%) were female. The mean age of the participants was 71.33 ± 7.35 years, with a range between 60 and 89. Other demographic characteristics of the participants are included in Table 1. As shown in this table, the post-coronary care unit had the highest elderly patient load and the orthopedic ward had the lowest.
Demographic Characteristics of Participants.
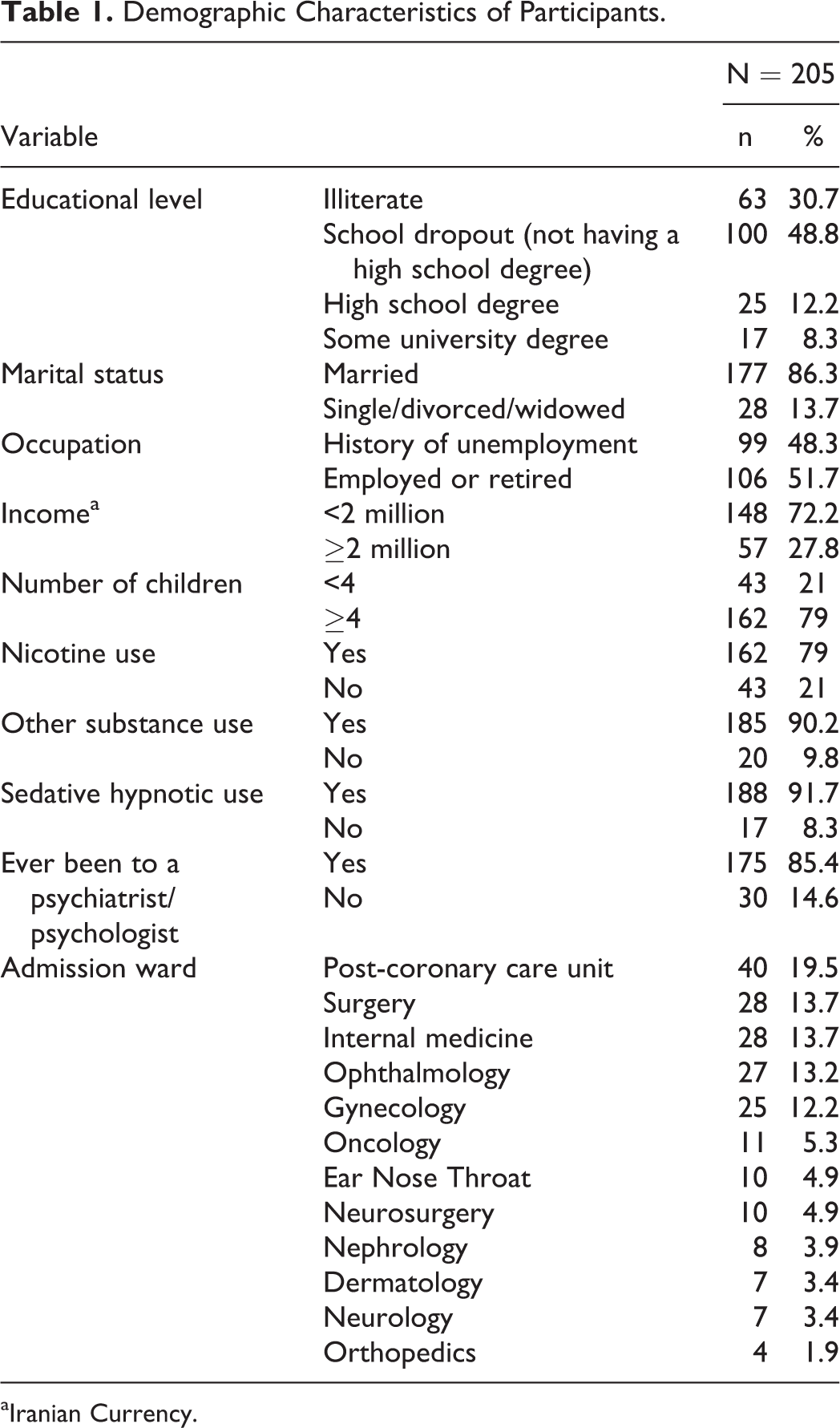
aIranian Currency.
Of the 205 patients, 130 (63.4%) had normal cognitive function, while 75 (36.6%) had some degree of impairment in their performance in cognitive tests. Within the latter group, 45 patients received dementia/major neurocognitive disorder diagnosis according to DSM-5 criteria, and the remaining 30 patients did not fulfill the criteria. Cognitive deficits in the latter group were assumed to be due to depression or mild cognitive impairment (MCI). Hence, the prevalence of dementia in our study was 22%. As represented in Table 2, only 60 (29.3%) of the 205 participants were able to draw a normal clock on the Mini-Cog test, and 145 (70.7%) patients failed to complete the task. There was a statistically significant difference between demented and nondemented groups in the ability to draw a normal clock (P < .001).
Clinical Characteristics of Patients With Dementia Compared to those Without.
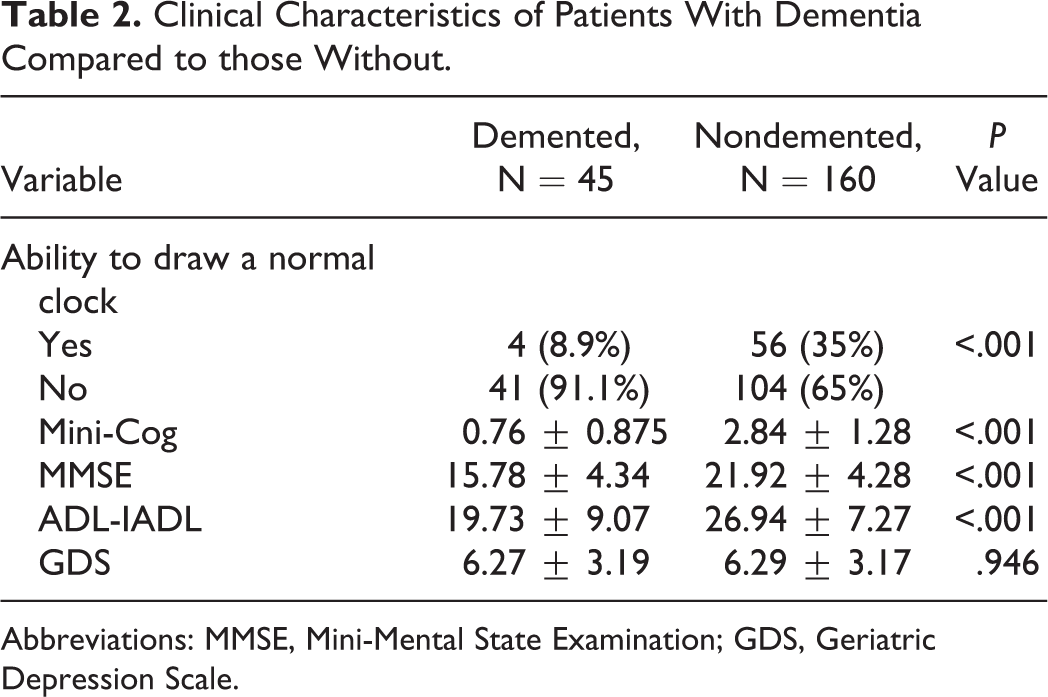
Abbreviations: MMSE, Mini-Mental State Examination; GDS, Geriatric Depression Scale.
The mean (standard deviation [SD]) of the Mini-Cog scores for demented and nondemented groups were 0.76 (0.875) and 2.84 (1.28), respectively. There was a statistically significant difference between these 2 groups in the Mini-Cog scores (P < .001). Additionally, the mean (SD) of the MMSE scores in the demented group was 15.78 (4.34) compared to 21.92 (4.28) in the nondemented group. In a similar manner, demented and nondemented groups differed significantly in their MMSE scores (P < .001). Since formal education affects cognitive performance on the MMSE, low MMSE scores of nondemented patients could be due to an educational bias.
The mean ADL-IADL scores were 19.73 (9.07) in the demented group and 26.94 (7.27) in the nondemented patients. The Mann-Whitney U test revealed a statistically significant difference between demented and nondemented groups with respect to ADL-IADL scores (P < .001).
The mean GDS scores in the 2 groups were compared using the Mann-Whitney U test, which showed no significant differences between the demented (6.27 [3.19]) and nondemented groups (6.29 [3.17]; P = .946).
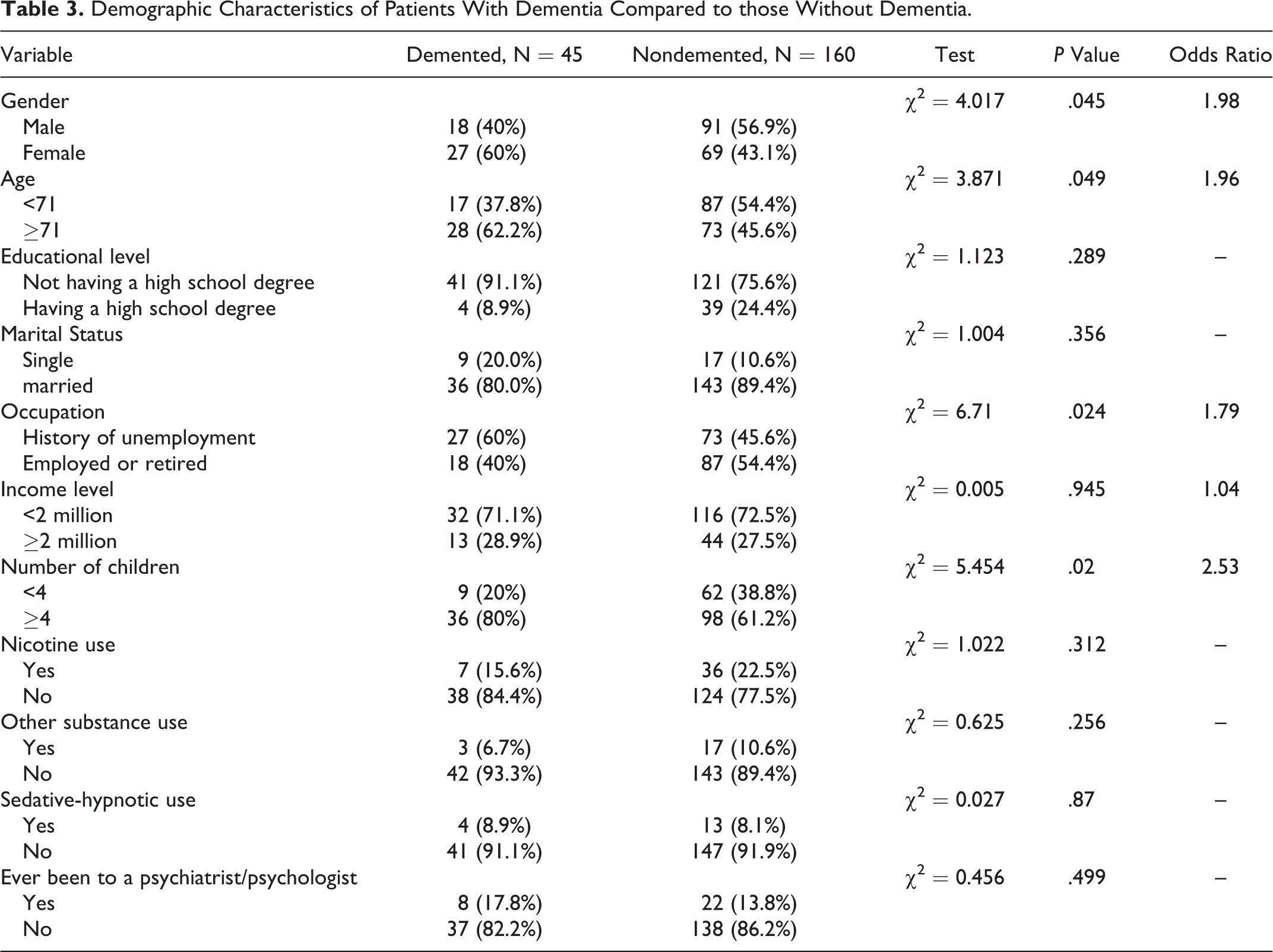
The results also showed that there is a statistically significant relationship between gender, age, number of children, occupation, and the prevalence of dementia (Table 3). Females were 1.98 times more likely to have dementia than males. Patients aged 71 and older were 1.96 times more likely to have dementia compared to those younger than 71. Moreover, having 4 or more children was associated with a reduced occurrence of dementia (OR = 2.53, P = 0.04). Dementia was also significantly associated with a history of unemployment (OR = 1.79, P = 0.024).
Demographic Characteristics of Patients With Dementia Compared to those Without Dementia.
Discussion
To our knowledge, this is the first study on the prevalence of dementia in medically ill elderly patients admitted to a general hospital in Iran. Results of this study demonstrated that dementia is common in older patients admitted to Rasoul-e Akram hospital (22%). A worthwhile point to consider is that none of these patients with dementia had a formal diagnosis established prior to this investigation.
Few previous studies have investigated the prevalence of dementia in general hospital inpatients in developing countries. Our results are comparable to the prevalence of dementia (17%) recorded by Maia et al in a study conducted in 5 general hospitals in Florianopolis, Brazil. 9 However, our found percentage (22%) of dementia prevalence is higher than the prevalence estimate (8.8%) reported by Dieu donné et al in a cross-sectional research study in Benin. 23 This discrepancy could be attributed to the fact that their sample consisted of younger patients who went through consultation in the neurology department.
With respect to the studies conducted in developed countries, our results were broadly in line with a recent study reporting a prevalence of 21% across 493 older patients admitted to medical, surgical, or orthopedic wards in 4 Queensland teaching hospitals. 24 Similarly, Timmons et al reported a dementia prevalence of 25% in older adults admitted to acute hospitals in Ireland. 25 However, our result of 22% dementia prevalence was lower than the 38% found by Briggs et al in elderly patients presenting to acute hospital services in Ireland. 26 Our percentage is also lower than 42%, recorded by Sampson et al in a research on medical admissions of elderly patients to a London teaching hospital. 7 Several reasons may explain the abovementioned differences in prevalence rates. First, in the studies by Sampson et al and Briggs et al, patients aged 70 and older who underwent acute medical admission were included. As shown by previous studies, 27,28 cognitive impairment and prevalence of dementia increase with age. We can also expect such conditions to be more common in older patients admitted to acute medical wards compared to other hospital wards. 29 As mentioned before, in our study, participants were aged 65 and over, and those admitted to the emergency ward were not included. Second, unlike our study, Briggs et al did not exclude patients with delirium. 26
Another notable observation is that according to our results, the prevalence rate of dementia in general hospitals is far more than rates found in the normal community, which is around 6%. 30 In 2014, Rashedi et al reported that the prevalence of severe cognitive disorder in community-dwelling older adults was 2.8%, 31 and results of the National Elderly Health Survey (NEHS) in Iran showed that the overall crude prevalence of dementia among people aged 60 years was 7.9% (8.7% in women and 6.5% men). 32 Several studies thus far have revealed that dementia is associated with higher all-cause hospital admissions and that patients with cognitive impairment are among the most frequent service users in general hospitals. 33 -35 There are several possible explanations for this finding. Primary conditions that heighten the risk of dementia (eg, cerebrovascular disease) or those that develop secondary to dementia (eg, dysphasia and urinary incontinence, which increase the risk of pneumonia and urinary tract infection) may increase the chances of hospital admission. In addition, dementia is associated with impaired ability to self-manage chronic diseases and to warn others about their presence, thereby increasing the risk of medical complications and the necessity for hospitalization. 29
In our research, dementia prevalence increased with age. The figure rose from 37.8% for patients younger than 71 to 62.2% beyond 71 years of age. This was consistent with the results of previous studies pointing out the association between age and prevalence of dementia. 27,28 In the present study, 60% of patients with dementia were females, although the total number of females was fewer than males. This result is in line with the findings of the majority of the previous research, which have reported higher rates of dementia within women. The interaction between genes, hormones, and the social environment may be the main reasons for this difference between genders. 36 We also found that the prevalence of dementia was higher in patients with 4 or more children. Beeri et al showed that having at least 1 child, rather than none, is associated with an increased risk of Alzheimer’s disease in women but not in men. 37 Other authors such as Colucci and Ptok have reported similar results. 38,39 The associations found in these studies could be ascribable to biological and social factors associated with women’s child raising and family issues. It is known that estrogen deprivation is a risk factor for Alzheimer’s disease. 40 There is evidence that estrogen levels are negatively associated with the number of children and women who have more children have lower circulating estrogen levels compared to women with few or no children. 41 Therefore, having more children could be related to Alzheimer’s disease neuropathology by causing a decline in estrogen. It should be noted that in the present study, no comparison was made between men and women on this factor.
Another point we would like to highlight about this study is that the rate of dementia prevalence was significantly lower among employed or retired individuals (40%) than unemployed patients (60%). Although this discrepancy may be due to differences in premorbid ability rather than the potential protective role of occupation, several studies have shown that not having an active job throughout one’s life increases the risk of dementia due to a reduction in cognitive reserves. 42
In our research, the prevalence of dementia was not found to be related to marital status. This is in step with a recent Italian study, which reported that marital status was not associated with dementia occurrence among persons aged 80 years or older. 43 Despite that, most authors have emphasized that lack of a family and social support should be considered as a major risk factor for dementia. 44 Furthermore, we did not find a significant association between level of education and prevalence of dementia. Again, this is dissimilar to most previous findings which suggest that higher education levels are associated with a reduced risk of cognitive decline. This difference in observations could be due to our limited sample size.
One unanticipated finding of the present study was that a great number of nondemented participants were not able to draw a normal clock on the Mini-Cog test, despite acceptable performance on other visuospatial constructional skills and executive function tasks. Therefore, it seems possible that in spite of the promising results of previous research by Sadeghipour et al, 45 the clock-drawing test has limited value for dementia screening in the older Iranian population. It is difficult to explain this result; however, it is likely that factors such as cultural, linguistic, or educational background play an important role here.
Conclusion
The results of this study are, to our knowledge, the first to shed light on hospital-based prevalence of dementia in Iran. The findings of this study, along with those of other studies in different countries, suggest that considerable numbers of older people admitted to hospitals have undiagnosed preexisting dementia, which increases the risk of unfavorable patient outcomes. Regular screening for dementia in all older adults is not recommended due to a lack of enough evidence. However, seeing as many people with dementia are admitted to hospitals for other physical illnesses prior to dementia diagnosis, dementia case finding in general hospitals can be a reasonable practice. Detection of cognitive impairment in older hospitalized patients may result in a timely diagnosis and an improvement in their immediate and future care planning. In this regard, it seems necessary to develop appropriate guidelines and train various medical specialists to screen and identify dementia symptoms in older hospitalized patients.
Strengths and Limitations
The strengths of this study included a fairly large sample size as well as carrying out a face-to-face patient assessment by geriatric psychiatrists, allowing for a high level of diagnostic accuracy. However, there are some limitations that must be noted. Our study was conducted in a single general hospital; therefore, the sample may not be representative. Moreover, complete information was not available from third parties for most of the patients evaluated, and this could have led to certain misclassification errors. Another limitation to consider was the design of our study. Prospective studies can provide more accurate information about factors associated with the prevalence of dementia. In addition, further multicenter studies may be necessary in order to corroborate our results.
Footnotes
Acknowledgment
This study was part of an MD thesis by Moein Moghaddamnia. We are especially grateful to all participants for their cooperation in this study.
Authors’ Note
The United Nations cutoff for referring to the older population is 60+ years.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.