
Abstract
Background:
Occurrence of adverse drug reactions is a major global health problem mostly affecting older adults. Identifying the magnitude and predictors of adverse drug reactions is crucial to developing strategies to mitigate the burden of adverse drug reactions. This study’s objectives were to estimate and compare the prevalences of adverse drug reactions, to characterize them and to identify the predictors among hospitalized older adults.
Methods:
A comprehensive systematic literature search including both prevalence and risk factors of adverse drug reactions in hospitalized older adults was conducted using PubMed, Scopus and Google Scholar, involving all articles published in English. Descriptive statistics and comparison of means was performed using SPSS version 20.0 and metaprop command was performed in STATA version 13.0. Heterogeneity was assessed using I2 statistic.
Results:
A total of 18 studies, involving 80,695 participants with a median age of 77 years, were included in this study. The pooled prevalence of adverse drug reaction was 22% (95% confidence interval: 17%, 28%; I2 = 99.23%). Among high-income countries, the prevalence of adverse drug reactions was 29% (95% confidence interval: 16%, 42%) as compared to 19% (95% confidence interval: 14%–25%) in low and middle-income countries (p value = 0.176). Of the 620 adverse drug reactions categorized, most were type A (89%), which are generally predictable and preventable. Two-thirds (795, 67%) of the adverse drug reactions were probable and most (1194, 69%) were mild or moderate. The majority (60%) of the categorized adverse drug reactions were preventable and less than one-third (31%) were severe. The most consistently reported predictors of adverse drug reactions in hospitalized older patients were medication-related factors, including polypharmacy and potentially inappropriate medications followed by disease-related factors—renal failure, complex comorbidity, heart failure and liver failure.
Conclusion:
Almost one-quarter of all hospitalized older adults experienced at least one adverse drug reaction during their hospital stay. The majority of the adverse drug reactions were preventable. Medication-related factors were the most consistently reported predictors of adverse drug reactions followed by disease-related factors.
Introduction
According to the World Health Organization (WHO), 1 an adverse drug reaction (ADR) is defined as “any response to a drug which is noxious and unintended, and which occurs at doses normally used in man for prophylaxis, diagnosis, or therapy of disease, or for the modification of physiological function.” Occurrence of ADRs is a major global problem for patient safety and it affects different age groups; the older population of 60 years and above is the most vulnerable. Globally, ADRs contribute significantly to morbidity and mortality.2–4 Among the hospitalized older patients, significant proportions (15%–35%) experience an ADR during their hospital stay.5–7 About 10% of hospital admissions are related to ADRs.8–10 In the United States, approximately 100,000 emergency hospital admissions of older adults were attributed to ADRs every year. 11 Most of the ADRs in the elderly are predictable and preventable and are caused by commonly prescribed drugs. 12 More severe ADRs are more likely to be preventable. 13
WHO 14 defines older adults (elderly) as those aged 60 years and older. WHO 14 has estimated that between 2015 and 2050, the proportion of the world’s population over 60 years would nearly double from 12% to 22%, and in 2050, 80% of older people will be living in low- and middle-income countries.
Older age was consistently reported as a risk factor for ADRs.15,16 Older people undergo various physiological changes that result in drug pharmacokinetic and pharmacodynamic changes, making them highly susceptible to ADRs. 17 Moreover, multiple diseases in older adults account for polypharmacy, which increases the risk of ADRs by mounting the probability of drug interactions.7,18 Incidence of ADRs in older adults (11%–32%)19,20 is higher compared to the general population, ultimately reducing the patient’s compliance and complicating the patient’s treatment outcomes and thus, effecting a high burden on the healthcare system.21,22
Strategies that precisely address the management of complex drug regimens are required. 23 Studies focusing on predictors of ADRs among hospitalized older adults are scarce in low or middle-income countries (LMICs). 24 However, the identification of these predictors is crucial to develop preventive strategies that help to mitigate the burden of ADRs in clinical as well as economic aspects in the developing world.25,26 Potential risk factors for ADRs in LMICs differ from those in high-income countries (HICs); greater proportions of patients taking antituberculosis (anti-TB) and antiretroviral therapy (ART), a high prevalence of anemia and malnutrition, highly prevalent use of traditional medicines, and higher incidence of concomitant anti-TB drugs and ART with overlapping adverse effects, all contribute to higher risk for ADRs in low or middle-income countries.24,27,28
Two of the previous systematic reviews6,29 that reported prevalence of ADRs in hospitalized older patients did not consider the predicting risk factors and focused on the culprit drugs. Moreover, they excluded participants 60–64.9 years of age in studies from LMICs that employed recommendation by the United Nations (UN) 30 and WHO 14 for age 60 years and above for the older adults population. In addition, those studies might have missed data even for participants 65 years and above when the authors could not share the data specific to that age group. The other systematic review published in 2014 10 did not include the studies conducted after 2014 and was limited to studies in critical care settings. To the best of our knowledge, no systematic review has been conducted on the prevalence and risk factors of ADRs among hospitalized older adults involving general wards, geriatric wards as well as critical and emergency settings.
This study aimed at estimating the magnitude of ADRs among hospitalized older adults, identifying the predictors, comparing the case of LMIC and HICs and ultimately generating recommendations to mitigate the burden of ADRs, thus giving direction for future studies.
Method
This systematic review was performed according to Preferred Reporting Items for Systematic Reviews and Meta Analyses (PRISMA) guidelines. 31
Search strategy
A comprehensive systematic literature search focusing on the prevalence and risk factors of ADRs in hospitalized older adults was conducted using MEDLINE (PubMed), PubMed (HINARI), Scopus and Google Scholar to recover articles published in English until 31 December 2020. Hand searching of references of the relevant systematic reviews was also conducted during the same period.
A combination of the following keyword terms were used: “adverse drug reactions,” “drug related side effects,” “adverse drug events,” “adverse drug effects,” “drug toxicity” combined with “adult patients,” “elderly patients,” “older adults,” “older patients,” “geriatric patients.” The synonyms were combined with OR and then words of parallel concept combined with AND. All searches were limited to an abstract or title. In the advanced search of PubMed, the keywords were combined as follows: “adverse drug reactions” OR “drug related side effects” OR “adverse drug effects” OR “drug toxicity” AND “adult patients” OR “elderly patients” OR “older adults” OR “older patients” OR “geriatric patients” in the title or abstract for all words. In Google Scholar, we used the following search strategy: allintitle: “adverse drug reactions” OR “side effects” OR “drug related side effects” AND “old patients” OR “older adults” OR “elderly” OR “geriatric patients.”
Selection criteria and data extraction
Articles were included when they met the following eligibility conditions: observational studies reporting on the prevalence or predictors/risk factors of ADRs in hospitalized older patients 60 years and above in studies from LMICs and 65 years and above in studies from HICs. All prospective or retrospective observational studies that reported prevalence or/and predictors/risk factors of ADRs, both as primary or secondary endpoint, in older inpatients were included. Validation studies that used data from previously published study or those that did not report prevalence of ADRs were excluded. We excluded studies that involved patients with a specific condition or drug and studies involving dose-related adverse drug events, medication errors, treatment failure and drug poisoning. Reviews, meta-analysis, case–control and systematic reviews were all excluded during the review of abstracts. We also excluded studies that solely employed spontaneous ADR reporting to generate their data because such studies underestimate the actual prevalence of ADRs as asymptomatic, transient and mild ADRs are not commonly reported.8,32 Study participants included were older patients 60 years and above in LMICs 30 and 65 years and above for studies from HICs, who were involved in ADR studies during hospitalization.
For inclusion in this review, studies were required to employ an obvious definition of ADR, for example, WHO, 1 Edwards and Aronson, 33 and so on, and a clear determination method for ADR causality including, for example, Naranjo et al., 34 WHO, 1 and so on. We included only studies with consistent and accurate ADR identification procedures and those with clear data analysis for determining the risk factors. We excluded duplicate studies by comparing the title, abstract and full-text for all articles retrieved. We classified low-income and HICs according to the World Bank 35 classification for the fiscal year 2021.
To determine eligibility, abstracts of the recovered studies were screened independently by T.M.Y. and S.D. Full-text articles of eligible studies were then reviewed and data were extracted and compared for consistency by both T.M.Y. and S.D. for those studies considered eligible from title/abstract. The other researchers (P.E.A., R.T. and P.O.E.) were consulted when consensus was not reached between the two researchers on inclusion of the specific studies or extraction of the respective results.
Data collected include year of publication, country, study participants, study design, definition and causality assessment of ADRs, prevalence of ADRs, types, severity, and preventability of ADRs, and the risk factors of ADRs.
Study quality assessment
The risk of bias was evaluated by two of the reviewers (T.M.Y./S.D.) using a method adapted form of the Newcastle-Ottawa Cohort Scale, 36 which allowed the evaluation of cross-sectional studies, the risk of selection bias and misclassification bias.
Statistical analyses
The extracted data were entered on MS Excel version 2016 and imported to SPSS version 20.0. Frequencies and percentages were generated from descriptive statistics. Tables and charts were also used to present the data. The distribution of the ADR prevalences was tested for normality using Kolmogorov–Smirnov test (p value = 0.08). Thus, distribution of the prevalence of the individual studies was summarized as mean ± standard deviation. The Excel data were then imported to STATA version 13.0 (Statacorp, LP, College Station, TX). The prevalence values from the different studies were pooled using the metaprop command in STATA. The effect estimate (ES; prevalence of ADR) and 95% confidence intervals (CI) were determined. Heterogeneity was assessed using I2 statistic and chi-square test. Random-effects model (REM) was employed using DerSimonian and Laird method due to significant heterogeneity. The possible presence of publication bias was assessed using Egger’s test.
Results
Included studies and participants
Based on predefined inclusion and exclusion criteria, we included 18 studies7,20,21,37–51 that reported the prevalence and predicting risk factors of ADRs in hospitalized older adults. All inpatients 60 years and older in studies from LMICs and 65 years and above in studies from HICs were studied (Figure 1).

Flow chart showing included and excluded studies.
Study participants
A total of 80,695 participants (52.2% being females among 74,256 with available gender information) with a median age of 77 years were included in this study. Two-thirds of the studies (12/18) employed prospective study designs.20,21,37–39,41–43,48–51 One-half (9/18) of the studies20,21,41–43,46,47,49,51 were based in general hospital wards including medical, surgical, oncology, nephrology, and stroke wards, whereas four were done in geriatric wards7,38,39,50 and the remaining five37,40,44,45,48 are from emergency and critical care settings.
ADR definition and causality methods
A total of 13 out of the 18 included studies20,21,41–51 used ADR definition by WHO, whereas 4 employed the Edwards and Aronson definition. Naranjo ADR causality method was the most commonly (10/18) employed among the included studies21,37,41–45,47,49 (Table 1).
Summary of the included studies.

ADRs: adverse drug reactions; WHO: World Health Organization; UK: United Kingdom; WHO-UMC: World Health Organization Uppsala Monitoring Center; ICU: intensive care unit.
Value not reported.
General wards: Medical, surgical, oncology, nephrology and stroke wards.
ADR prevalence
A total of 77,925 older adults involved in 12 studies7,20,37–40,45–50 from HICs and 2770 from 6 studies21,41–44,51 from LMICs were included. A sum of 7752 ADRs was reported: 6934/7752 from studies in HICs and 818/7752 from studies in LMICs. No study was obtained specifically from low-income countries. The prevalence of ADRs in hospitalized older patients ranged from 6.3% 40 to 64.4% 41 with standard deviation of 14.1 and mean prevalence of 23.7% (95% CI: 16.7, 30.7) (Table 1).
Characteristics of ADRs (causality, severity and preventability)
The included studies used the Schumock and Thornton 52 method to categorize preventability of ADRs; employed the Rawlins and Thompson method 52 to classify ADRs as type A (predictable reactions) and type B (non-predictable reactions); and used different severity assessment methods, including Hartwig et al. 53 ADR severity scale and team of expert’s assessment. A total of 11 studies20,21,37–39,41,42,45,47,49,50 reported the characteristics of a total of 1923 ADRs; 1292 ADRs from HICs and 631 ADRs from LMICs. According to the 3 studies21,38,42 that reported the types of ADRs, out of 620 ADRs identified, most (550, 89%) were classified as type A. Similarly, according to 8 studies20,21,37–39,42,45,49 that reported the causality assessments, out of a total of 1191 ADRs, about two-thirds (795, 67%) were classified as probable, whereas only 115 (10%) were rated as definite. On the contrary, among the 6 studies21,37,38,42,45,49 that reported the preventability status of 909 ADRs, the majority (543, 60%) were probably or definitely preventable. Among the 9 studies20,21,38,41,42,45,47,49,50 that rated the severity of 1738 ADRs, most (1194, 69%) were rated as mild to moderate, while 544 (31%) were rated as severe (Table 2).
The characteristics of ADRs documented among the hospitalized older adults.

ADR: adverse drug reactions.
Values not reported.
Comparison of the prevalence and characteristics of ADRs in HIC and LMICs
The prevalence of ADRs ranged from 6% to 46% (20.5; 14.8, 27.3; 95% CI) in HICs and from 10.7% to 64.0% (30.2; 17.8, 46.1; at 95% CI) in LMICs. The mean percentage of preventable ADRs of 68.4% in HICs was comparable with that of 60.5% in LMICs, whereas the percentage of severe ADRs 42.7% in HICs was much higher compared to 5% in LMICs (Table 3).
The comparison of prevalence, percentage of preventable and severe ADRs among hospitalized older adults from LMICs and HICs.
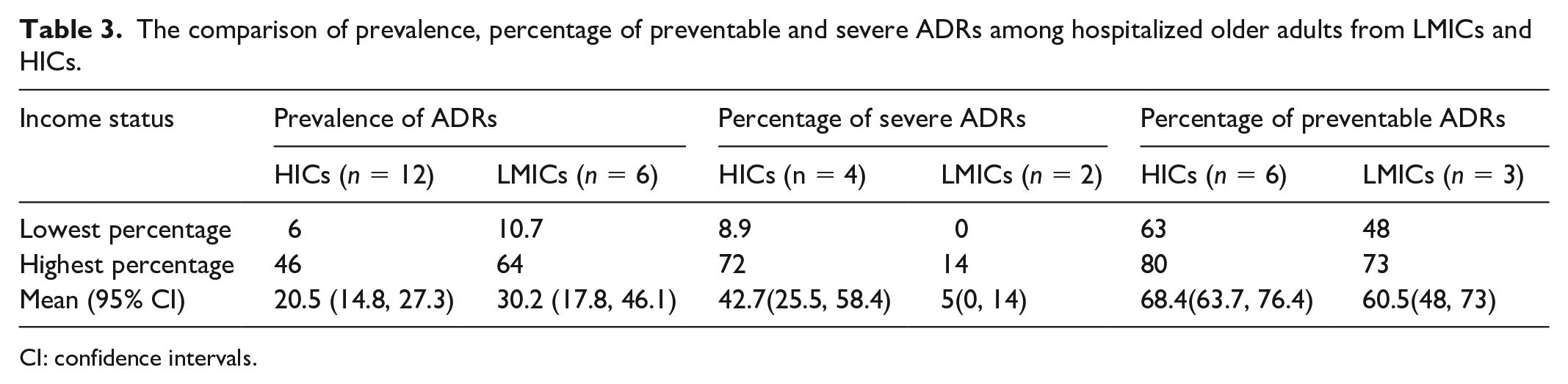
CI: confidence intervals.
Meta-analyses of ADR prevalence
Pooled prevalence of ADR in hospitalized older patients
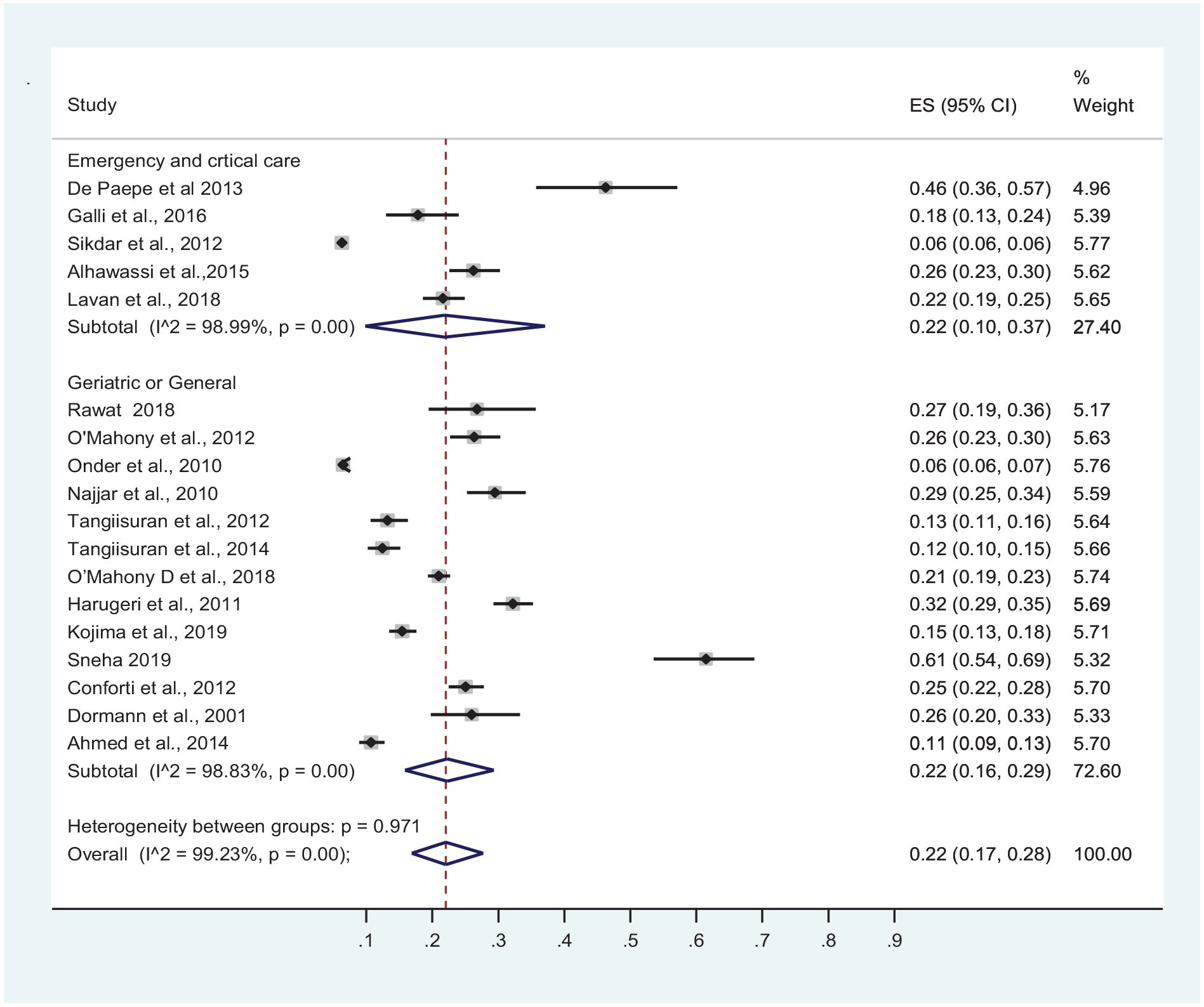
The pooled prevalence of ADR in hospitalized older patients was 22% (95% CI: 17%, 28%; I2 = 99.23%). The pooled prevalence of ADRs was higher in LMICs than in HICs at 29% (95% CI: 16%, 42%) versus 19% (95% CI: 14%–25%), respectively. However, this difference was not statistically significant (p value = 0.170) (Figure 2). Subgroup analysis by study design showed a significantly higher prevalence of ADR in prospective studies (p value = 0.008); 26% (95% CI: 20%, 33%) versus 15% (95% CI: 9%, 21%) (Figure 3). On the contrary, subgroup analysis by study setting showed no significant difference (p value = 0.971) in ADR prevalence between studies conducted at acute and emergency care, and geriatric or general wards, at 22% each (Figure 4).

Forest plot of prevalence of ADR by study by income status.

Forest plot of prevalence of ADR by study design.
Forest plot of prevalence of ADR by study setting.
Publication bias, heterogeneity and risk of bias assessment
High heterogeneity, I2 = 99.23%, and p values < 0.001 was observed. The Newcastle-Ottawa cohort scale 36 showed that all of the studies had low risk of bias in general. The risk of bias among included studies according to authors’ judgment is presented in Figure 5. Egger’s test showed the presence of publication bias (p value < 0.0001); studies with a small sample size might have been missed, as shown in Funnel plot (Figure 6).

Risk of bias graph: review authors’ judgments about each risk of bias item presented as percentages across all included studies.

Funnel plot of Egger’s test (p value < 0.0001).
Predicting risk factors
Medication-related factors were the most commonly implicated predictors in hospitalized older adults. Reported by 107,20,37–39,42,45–47,51 of the 18 studies, polypharmacy or concurrent use of five or more medications was the most consistently identified predicting risk factor of ADR among hospitalized older adults, followed by the use of potentially inappropriate medications (PIMs), which was reported by two studies.20,46
The next most frequently reported risk factors of ADRs were disease-related factors: renal disease was reported by five studies20,42,45–47 followed by having four or more comorbid conditions or higher Charlson comorbidity index (CCI), which was reported by three studies.42,46,47 CCI is used to predict 10-year survival in patients with comorbidities. Several patient-related factors were also identified as risk factors of ADRs, particularly female gender reported by five studies21,37,41,45,46 followed by longer hospital stay reported by four studies.7,38,39,42 The healthcare setting involved was the only health facility-related factor reported as an independent risk factor of ADRs among hospitalized older adults 42 (Table 4).
The independent risk factors identified among the hospitalized older adults.
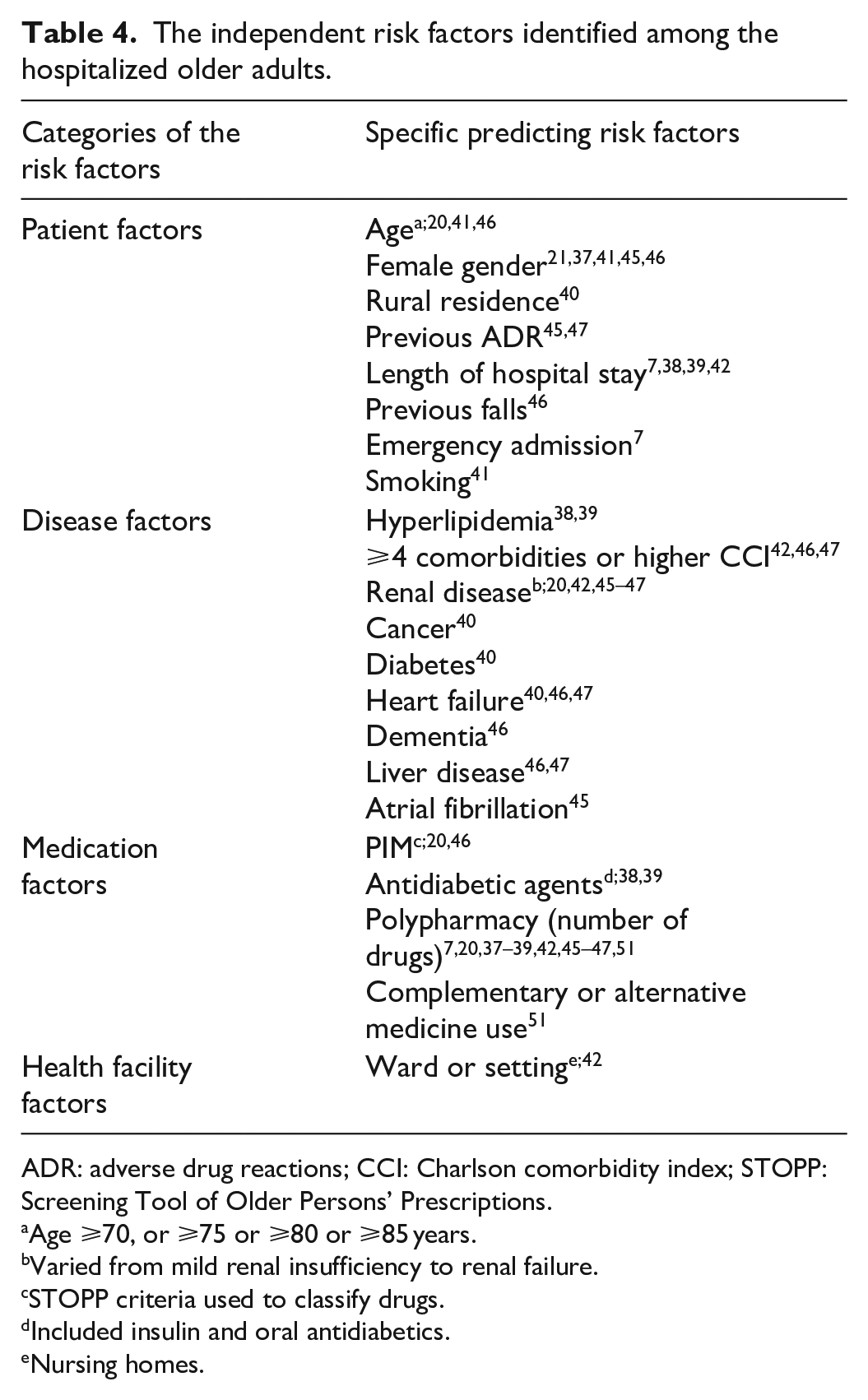
ADR: adverse drug reactions; CCI: Charlson comorbidity index; STOPP: Screening Tool of Older Persons’ Prescriptions.
Age ⩾70, or ⩾75 or ⩾80 or ⩾85 years.
Varied from mild renal insufficiency to renal failure.
STOPP criteria used to classify drugs.
Included insulin and oral antidiabetics.
Nursing homes.
Discussion
At 80,695 participants from 18 studies, this review is one of the largest systematic reviews on prevalence and risk factors of ADRs in hospitalized older patients. Because the previous systematic reviews6,10,29 addressed the drugs commonly associated with ADRs and the systemic classification of common ADRs, we focused on prevalence, risk factors, preventability, severity and types of ADRs and compared the case of LMICs and HICs. This is the first large systematic review that compared ADR and prevalence and risk factors between LMICs and HICs. A total of 7842 ADRs were reported: 6934(89.4%) from HICs and 818(10.6%) from LMICs.
The pooled prevalence of ADR in hospitalized older patients was 22% (95% CI; 17, 28), with individual prevalences ranging from 6.3% 40 to 64.4%. 41 This is higher compared to the prevalence of 2% in the general adults. 32 Previous studies were also consistent with a higher prevalence of ADR in older adults.15,16 This reproduces the fact that aging is associated with multiple morbidity, renal impairment and polypharmacy, thus ultimately resulting in increased ADR occurrences.54,55
The current ADR prevalence among hospitalized older adults is also higher than ADR prevalences ranging from 5% to 10% in ambulatory older patients,13,56 respectively. ADRs are more prevalent among hospitalized older patients, probably because of more complex comorbidity and more number of medications during hospitalization. More frequent medication changes in admitted patients might contribute to more prevalent ADRs. 57 Thus, more effort to prevent ADRs is warranted in hospitalized older patients.
The pooled ADR prevalence of 22% observed in the current study is comparable with 24% in a systematic review published in 2018. 6 However, it is higher than the pooled prevalence of 16% reported by another systematic review published in 2020. 29 This difference can be explained by the fact that our study included solely studies conducted specifically among older adults, whereas the later included studies had been done among general adults that reported subgroup ADR prevalence for older adults, and it also excluded participants 60–64.9 years that we have included. However, the most important explanation is probably the fact that the review missed several studies conducted in older adults that have been included in this study. To this effect, Jennings et al. conducted meta-analysis for only 20,153 compared to the current study with 80,695 patients.
The current prevalence of 22% is also higher than the mean prevalence of 11.5% reported by another systematic review in critically ill hospitalized older patients. 10 This deviation can be explained by the fact that the current study consisted mainly of prospective studies (12/18) which had been shown to detect more ADRs compared to retrospective studies. An additional explanation is the probable temporal rise of the prevalence of ADR in this group of population.
A subgroup meta-analysis by study setting showed no significant difference (p value = 0.971) in ADR prevalence between studies conducted at emergency or acute care settings, and geriatric or general wards (22% each). Most previous studies on ADRs also confirmed that disease and drug characteristics, rather than the study setting, determine the risk of in-hospital ADRs among older patients.20,42,46
All of the studies from LMICs were from middle-income countries and none could be recovered from low-income countries. This highlights an outstanding gap of research in low-income countries in the area of ADRs among hospitalized older adults. Therefore, researchers in these countries should consider to address this important area of pharmacovigilance.
The prevalence of ADRs in LMICs was higher compared to HICs; a pooled prevalence of 29% (95% CI: 16%, 42%) versus 19% (95% CI: 14%, 25%) (p value = 0.561). Greater proportions of patients taking anti-TB and ART, a high prevalence of anemia and malnutrition, highly prevalent use of traditional medicines, and higher incidence of concomitant anti-TB drugs and ART with overlapping adverse effects24,27,51 could explain the higher pooled ADR prevalence in LMICs. However, this difference was not statistically significant (p value = 0.170).
The high variation between the prevalence reported by the individual studies, which ranged from 6.3% 40 to 64.4% 41 could be explained by the differences in study design and the methods used to detect the ADRs. In the current study, subgroup meta-analysis by study design showed a significantly higher (p value = 0.008) prevalence of ADR in prospective studies: 26% versus 15%. This is likely because of potentially missing data, recall bias or incomplete information that is commonly encountered by retrospective studies. Such large variations in the ADR prevalences between the individual studies were also reported by previous systematic reviews.6,10,24
Of all categorized ADRs, 89% (550/620) were type A that are potentially predictable, 67% (n = 795/1191) were probable and only 10% were definite. The majority (60%, 543/909) of ADRs were probably or definitely preventable. This shows that significant percentages of ADRs in hospitalized older patients can be prevented if active ADR prevention strategies are implemented. Preventing ADRs among hospitalized patients can save huge health expenditure in addition to reducing mortality and hospital stay associated with ADRs.25,26
The percentage of preventable ADRs was comparable: 60.5% in LMICs versus 68.4% in HICs. On the contrary, the percentage of severe ADRs was significantly higher in HICs (42.7%) compared to 5% in LMICs. This finding is comparable with a review of the literature by Angamo et al. 24 This higher percentage of severe ADRs in older patients from HICs may be related to having more complex comorbidity, their advanced age and more access to newer medications compared to patients from LMICs.
The current study showed that medication-related factors were the most commonly implicated predicting risk factors in hospitalized older adults. Reported by 10 of the 18 included studies,7,20,37–39,42,45–47,51 polypharmacy or taking five or more medications was the most consistently identified predicting risk factor of ADR among hospitalized older adults, followed by the use of PIMs, which was reported by two studies, both of which were using the Screening Tool of Older Persons’ Prescriptions (STOPP) criteria.20,46 This finding is comparable with the results of Mudigubba et al., 54 which reported that polypharmacy was the most frequently reported predictor of ADR in hospitalized patients. Thus, a vigilant evaluation of pharmacotherapy among hospitalized older adults remarkably reduces the risk of incurring ADR during hospitalization.54,55 Because of the strong association between ADR and the number of medications as well as the use of PIMs, identification of PIMs and systematic deprescribing in hospitalized older patients is probably one of the most effective strategies for mitigating the burden of in-hospital acquired ADRs. 58 To this effect, the application of STOPP and The Norwegian General Practice criteria (NORGEP) to hospitalized older patients demonstrated a significant circumvention of the use of PIMs, and thus reduction in risk of ADRs.59,60
The next most frequently reported risk factors of ADRs were disease-related factors: renal failure reported by five studies,20,42,45–47 having four or more comorbid conditions reported by three studies,42,46,47 heart failure by three studies40,46,47 and liver failure,46,47 cancer and hyperlipidemia38,39 each reported by two studies. Renal impairment directly reduces the excretion of most medications and raises the risk of future ADRs. In the current study, it was shown to be the most consistently reported disease-related risk factors of ADRs. A previous study implicated both concealed and overt renal failure as important risk factors for ADR. 61 Likewise, most of the drugs are metabolized in the liver before excretion. Some medications are eliminated through biliary secretion to the gastrointestinal tract. Thus, liver impairment results in higher plasma drug concentration from normal dose of these medications and puts the patients at increased risk of ADR. Moreover, the complications of liver failure require multiple therapeutic and prophylactic medications associated with ADRs, including diuretics 59 and antibiotics. 62 Previous studies did also identify liver diseases as a predictor of ADR and other adverse drug outcomes.17,63
Having four or more comorbidities was also reported by three previous studies by Alhawassi et al., 10 Mudigubba et al. 54 and Green et al. 64 More comorbidity usually requires concomitant use of numerous medications, which, in turn, increases the risk of ADR. On the contrary, Catananti et al. 65 explained that ADR risk with heart failure might be attributed to the use of cardiovascular drugs, which were shown by Kongkaew et al. 32 to be the most frequent culprit of ADR in adults and older adults. Moreover, the higher number of medications often taken by this group of patients might even increase the risk.
Both having diabetes 40 and being on antidiabetic medications38,39 were shown to be risk factors for ADRs in hospital. This can be explained by the higher susceptibility to hypoglycemia, multiple medications, 32 diabetic nephropathy 61 and cardiovascular comorbidities66,67 in older patients with diabetes.
Similarly, older hospitalized patients with cancer, 40 hyperlipidemia,38,39 dementia 46 and atrial fibrillation 45 have been shown to be at increased risk of hospital-acquired ADRs. This may be explained by risk associated with the medications they take and a need for special precautions and a close follow-up in such patients. The very old, 80 years or older, are at higher risk of ADRs in hospital,20,41,46 likely because of more complex comorbidity.
Among the patient-related factors, female gender was reported by five studies21,37,41,45,46 followed by longer hospital stay, which was reported by four studies.7,38,39,42 Female gender was also reported by previous studies by Alhawassi et al. 10 and Mudigubba et al., 54 as the most important patient-related predictor of ADR. This higher risk is probably because women generally have a larger body fat, lower lean body mass, reduced hepatic clearance, differences in activity of cytochrome P450 enzymes, and metabolize drugs at different rates compared with men. 68 The risk associated with longer hospital stay may be explained by a higher risk of acquiring ADR in the hospital setting; in line with the fact that ADR is more prevalent in hospitalized older patients compared to older patients in the outpatient setting, as discussed above. Previous ADR was also implicated by a previous review by Angamo et al. 24 The ADR profile of older patients should be properly documented to avoid re-exposure to the same medications, or for a possible more cautious use of similar drug products, thus preventing future ADRs.
Limitations
A possible publication bias and missing out articles without accessible full-texts are among the probable limitations of the study. The other important limitation was that some of the studies did not classify the types, severity and preventability of ADRs. Moreover, no study from low-income countries was included; all of the studies included from LMICs were from the middle-income countries. Studies conducted on general adults that did subgroup analysis for older adults were not included.
Conclusion
This study revealed that almost one-quarter of all hospitalized older adults experienced ADRs during their stay in hospital. Prospective studies detected significantly higher ADRs compared to retrospective studies. The prevalence of ADRs was higher in LMICs than in HICs but the difference was not statistically significant. There was no significant difference in the percentage of preventable ADRs between HICs and LMICs. However, severe ADRs occurred more frequently in HICs. Medication-related factors like polypharmacy and PIMs were the most frequently reported predictors of ADRs followed by disease-related factors, renal failure, having four or more comorbid conditions, heart failure, liver disease, hyperlipidemia, cancer and atrial fibrillation. Female gender, longer hospital stay, age and previous ADR were the most frequently reported patient-related predictors of ADRs. These findings can be applied in guiding active pharmacovigilance services and by informing clinicians on prioritizing and monitoring of hospitalized older adults at high risk of experiencing ADRs.
Footnotes
Acknowledgements
The authors thank PHARMBIOTRAC, Mbarara University of Science and Technology, a project of World Bank ACE-II for supporting the corresponding author’s tuition for his PhD studies.
Author contributions
T.M.Y. and S.D. conducted the systematic searching, reviewed the abstracts and full-text articles, and extracted and analyzed the data. T.M.Y. compiled the manuscript. P.E.A., R.T., F.E.K. and P.E.O. contributed to developing methods and were consulted when consensus was not reached between the two researchers on inclusion of the specific studies. They also reviewed and edited the final manuscript. Finally, all the authors read and approved the manuscript.
Availability of data and material
The dataset supporting the conclusions of this article is included within this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.