
Abstract
This study was conducted in order to examine the level of cognitive function of individuals ≥65 years of age with diabetes. The cross-sectional descriptive design was used. The research was carried out in the diabetes polyclinic of a university hospital between June 2016 and January 2018. The study sample consisted of 91 patients. Data were collected with the scale of Montreal Cognitive Assessment (MoCA). The average score of the patients in the MoCA Scale was found to be 19.61 ± 1.70 (min: 15, max: 26). Diabetes is a risk factor for cognitive dysfunction for individuals above 65 years of age. Health professionals regularly monitor the cognitive functions of diabetic patients and use the MoCA scale in these follow-up and plan training and counseling initiatives according to their needs.
Introduction
In the developed countries, the population in the geriatric age-group constitutes a significant part of the population. This ratio is expected to increase further in the coming years. 1 According to data of Turkey Statistical Institute, the elderly population in our country (65 and above) was 6 651 503 in 2016. 2 With the development of technology, the expected increase in the length of life causes an increase in chronic illness. Diabetes is one of the first 5 diseases among the common chronic diseases in the society. 2 According to Turkey’s health survey data, the rate of incidence of diabetes in Turkey was found to be 6.7%. 2 The known number of diabetic patients in the 65 to 99 age-group in the world is 122.8 million; the rate of incidence of diabetes in the older age-group is increasing steadily. 1 Diabetes is a systemic disease that can damage every organ in the body, including retina, skin, kidney, small and large vessels, and central and peripheral nerves, and it has an increasing frequency with obesity and advancing age. The duration of life with this disease is prolonged as the approaches to classical micro- and macrovascular disease prevention and treatment are improved. This means that existing treatment strategies for type 2 diabetes may lead to new nonaimed complications. Cognitive inefficiency and dementia are examples of these new complications. The correlation between diabetes and cognition has drawn more attention in the last decade. Cognition includes a group of mental functions such as attention, memory, learning, verbal recall, concentration, reasoning, problem-solving, and decision-making. 3 –5 The pathophysiology of the cognitive dysfunction of diabetes is not fully understood, but hyperglycemia, vascular disease, hypoglycaemia, and insulin resistance play an important role. 6 Diabetes is known to cause structural damage and functional disorders in various tissues and organs with time. Diabetes has been reported to cause a variety of cerebrovascular, neurochemical, and electrophysiological changes in the central nervous system. Due to these changes, the cognitive functions also become distorted. Experimental studies have reported that depression and anxiety levels increase as the age of experimental diabetic animals increases. Problems occur in the cognitive functions such as problem-solving, attention, interpretation in these study. 5,7 However, the age of onset of diabetes, the glycemic control level, and the duration of diabetes affect the severity of cognitive deficiency. A mild cognitive inefficiency, a disorder that involves a decrease in cognition, does not usually significantly interfere with daily independent function, but is a risk factor for dementia. 6,8 There are clinical trials that report an attenuation of the cognitive functions, a decrease in abstract reasoning and the complex psychomotor activity, and an increased risk of dementia in patients with type 2 diabetes mellitus (DM). 7,9 The evaluation of a patient in the geriatric age-group is a time-consuming operation. Therefore, there is a need for, as short as possible, standard and sensitive assessment tools that also can be implemented by health personnel for the diagnosis of certain diseases or symptoms, except for general health checks, internal, neurological, or psychiatric evaluations. The evaluation of the cognitive status and taking necessary precautions for diabetic patients are important for managing the procedure and preventing complications. 3,10 The goal of evaluating cognitive functions in a diabetic patient is to maintain the treatment and to know whether he needs help to manage diabetes. Thus, health professionals, patients, and caregivers will be able to predict the cognitive dysfunctions of elderly individuals with diabetes and take necessary precautions. 5,11,12 This hypothetical study was conducted to evaluate the cognitive functions of patients diagnosed with diabetes above 65 years of age.
Research Questions
What is the level of cognitive function of ≥65 years of age with diabetes. Is there a relationship between the sociodemographic characteristics of individuals with diabetes at age 65 and cognitive function levels? Is there a relationship between the clinical features of individuals with diabetes at age 65 and cognitive function levels?
Materials and Methods
Design and Sample
We used a descriptive cross-sectional design. The research was carried out in the diabetes polyclinic of a university hospital between June 2016 and January 2018. Convenience sampling methods were used. Seventeen (18.6%) patients refused to participate. The study sample consisted of 91 patients. Post hoc power analysis was done in our study. According to this research, effect size was 0.52 and power 80%. The inclusion criteria for patients were a person who voluntarily accepted participation in the research, who had been diagnosed with diabetes for at least 5 years, was literate in Turkish, had no hearing or speaking impairment, and was 65 years and older. Factors that disqualified patients from sampling were their diagnosis with any psychiatric and neurological disease, brain surgery, and alcohol-drug addiction.
Instruments
Demographic characteristics
This form is comprised of 10 questions regarding patients’ sociodemographic characteristics: age, sex, marital status, educational status, social insurance, any accident, surgery history, smoking, other chronic illness, and number of drugs used.
Montreal Cognitive Assessment
The Montreal Cognitive Assessment (MoCA) is a screening instrument and assesses 8 different cognitive domains that include attention and concentration, executive function, memory, language, visual/ constructional skills, conceptual thinking, calculations, and orientation. Although all sections are brief, each contains items selected from longer psychometric instruments. 13 –16 The maximum possible score is 30 points. Montreal Cognitive Assessment was developed by Nasreddine et al. 13 The adaptation, reliability, and validity studies of the scale in Turkey were already available. 16 Scale's cut off value is 21 points over 30 points. Internal consistency using Cronbach was .66. In this study, the reliability coefficient of the scale was determined as 0.71.
Ethical Considerations
Written permission from Mehmet Akif Ersoy University Ethical Committee (GO 2016/27) was obtained. The objective of the research was explained to the participants and written permission was received from those agreeing to participate in the research. Data were collected through face-to-face interviews to help increase the accuracy of the collected information.
Statistical Analysis
Analysis was conducted using descriptive statistics tests using the Statistical Package for the Social Services SPSS version 22.0 (SPSS Inc, Chicago, Illinois). Descriptive statistics were used to determine patients’ characteristics. The statistic “r” value of 0.00 to 0.24 was considered a weak relationship; 0.25 to 0.49 was a moderate relationship; 0.50 to 0.74 was a strong relationship; and 0.75 to 1.00 was a very strong relationship. 17 A test of hypothesis with P value of < .05 was considered significant.
Results
The average age of the patients was 70.56 ± 3.81 years (min: 65, max: 81), 60.4% were male, 89.9% were married, 54.9% were primary school graduates, and 97.8% had social security. It was found that 82.4% of the patients did not have an accident history, 64.8% did not undergo any surgery before, 68.1% had another chronic disease other than diabetes, 75.8% did not smoke cigarettes, and all of them were using drugs continuously. It was found that the average use of medication was 3.33 ± .77 (min: 1, max: 5). The average MoCA Scale score of the patients was found to be 19.61 ± 1.70 (min: 15, max: 26; Table 1).
Demographic Characteristics of the Patients.a
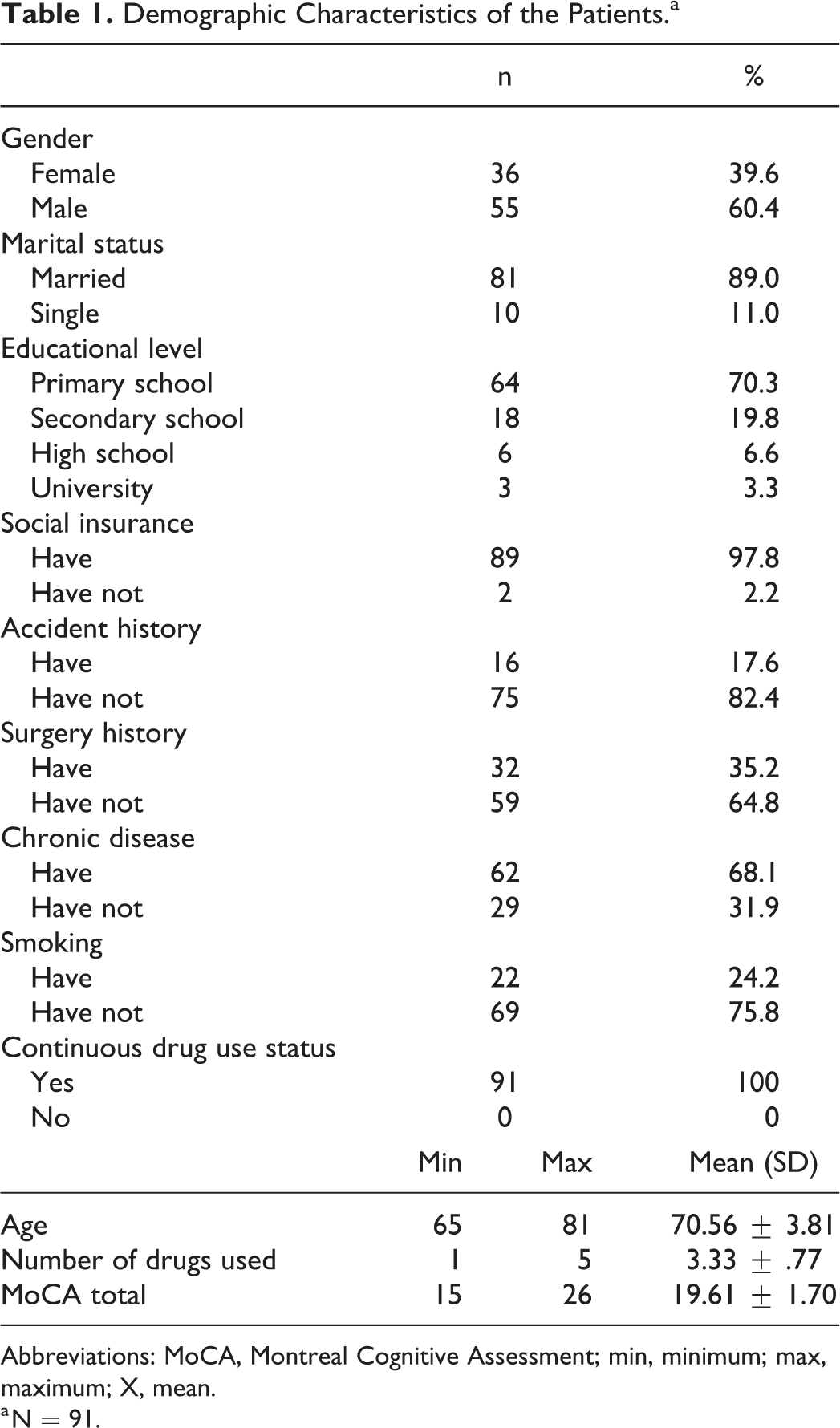
Abbreviations: MoCA, Montreal Cognitive Assessment; min, minimum; max, maximum; X, mean.
a N = 91.
There was no significant relationship between the age of the patients and the cognitive assessment scale when the individual characteristics of the patients were compared with the Montreal Cognitive Rating Scale Score and there was a negative weak significant correlation with the number of used medications (r = −0.206; P = .051). A statistically significant difference was found between the gender of the patients, educational status, having another chronic disease, and the MoCA Scale averages (P < .05). There was no statistically significant difference between the marital status, social security, the accident and operative history, the smoking status of the patients, and the MoCA Scale total average scores (P > .05; Table 2).
Comparison of the Montreal Cognitive Assessment Scale Point Averages According to Individual Characteristics and Clinical Characteristics of Patients.
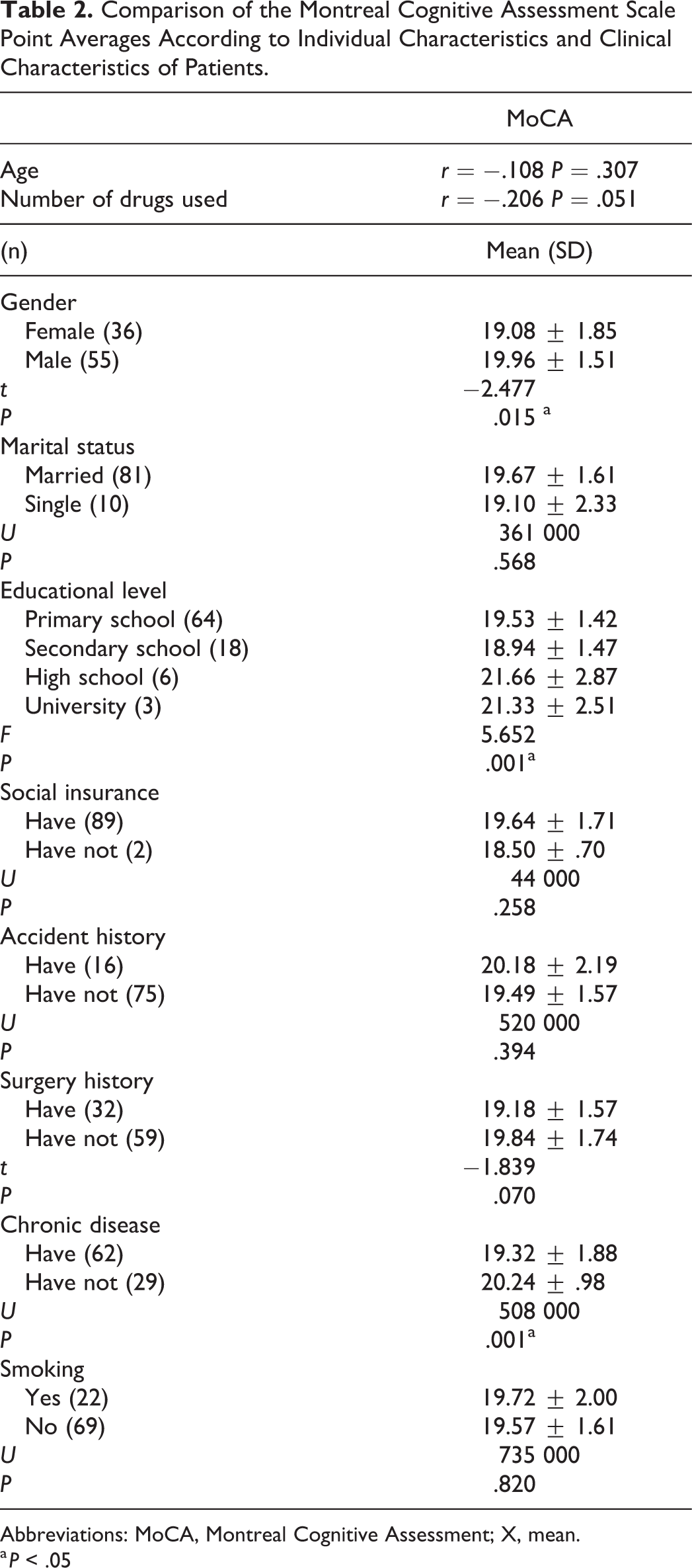
Abbreviations: MoCA, Montreal Cognitive Assessment; X, mean.
a P < .05
Discussion
Diabetes is an important risk factor for cognitive dysfunction and dementia. 5,6,8,16 In patients with type 2 DM, a cognitive function decrease, a decrease in abstract reasoning and complex psychomotor activity, and an increase in the dementia risk increases show up. 5,10 When compared to people without diabetes, diabetics suffer from cognitive dysfunction, particularly in memory and managerial functions. 7 The total MoCA cutoff score for cognitive inefficiency diagnosis is accepted as 21 points. According to our results, the cognitive functions of the participants were low (average 19). In case–control studies, type II DM cases have been shown to be worse in terms of verbal memory, speed of information processing, attention, and managerial activities compared to age, gender, and education-matched control group. 7 Diabetes is a disease that can cause cognitive dysfunction independent of other factors. Cognitive functions are reported in the studies to be impaired with advancing age. 5,12,18 There was no significant relationship between age and cognitive function in our study. The age range of the participating participants was 65 to 80. When the literature is reviewed, it is reported that the incidence of cognitive dysfunction, dementia, and Alzheimer is increased at people above 80 years of age. After the age of 85, the probability of getting a diagnostic of the Alzheimer’s disease is more than one-third. 15 It is thought that there are no significant associations between the samples constituting our study, while there are no individuals over 80 years old and the age groups are close.
When cognitive functions of participants were evaluated according to gender, they were found to be below the average of both genders; it is seen that the cognitive evaluation score of women is slightly lower than that of men. Elderly women living in society all over the world are at an economic, cultural, and political level of disadvantage compared to older men and it is stated that this will also negatively affect the health-related parameters of older women. 11 Age, gender, and educational status are shown as risk factors for cognitive inefficiency in patients with diabetes. Another study showed that the general health status of older women was significantly more affected by depressive symptoms than by male elderly people. In the same study, it was stated that the cognitive functions of both genders were similar. 19 Again, in a study conducted in our country, it is stated that elderly women are a risk group in terms of depression and cognitive inefficiency. 12 Our research result is compatible with the literature.
According to our study, when we look at the general average, the cognitive function scores of high school and college graduate participants are above the average. Education is an important factor in assessing cognitive function. Another scale used for cognitive evaluation is the minimal test. While in this test a score of 26 and below was sufficient for dementia for those who had an education for 8 years and above, this score is 18 or less for person who had an education for 1 to 8 years. 7 Studies show that the more the education level increases, the more cognitive impairment decreases. In a study conducted in Trabzon, the lack of education was reported as a risk factor for cognitive dysfunction. 12 In the study in which the reliability of the Turkish Cognitive Assessment (MOCA) Scale was made, it was stated that education was a factor affecting the test result. 14 Our research result supports the literature knowledge. The cognitive evaluation average scores of participants with a chronic illness were lower than those without an illness. Due to the advanced age of the sample group, it is not possible to eliminate all chronic diseases. For this reason, neurological disorders such as Parkinson, dementia, Alzheimer, psychiatric disorders, and neurosurgery, which may directly affect the cognitive level, have been determined as exclusion criteria. When the literature is reviewed, hypertension and heart diseases in diabetic patients can also affect cognitive functions. 18 The fact that cardiac disease are no exclusion criterion was accepted as a limitation in our study.
Conclusion and Recommendations
Diabetes is a risk factor for cognitive dysfunction in individuals over 65 years of age. Cardiovascular diseases are considered as exclusion criteria and new studies, regular monitoring of the cognitive functions of diabetic patients, and the use of the MoCA Scale are recommended.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.