
Abstract
Background:
Folie à deux is a clinical condition that was first described in 19th century. It is a psychotic disorder in which two closely associated individuals share a similar delusional system.
Objectives:
The aim of this article is to review the nosological significance of folie à deux and to explore the disorder among patients with dementia.
Methods:
Medline and Google Scholar searches were conducted for relevant articles, chapters, and books published before 2017. Search terms used included dementia, folie à deux, induced delusional disorder, neurocognitive disorders, shared psychotic disorder. Publications found through this indexed search were reviewed for further relevant references.
Results and Conclusion:
Cases of Folie à deux involving patients with dementia are reported quite infrequently. Most of the studies on the topic consist in case reports. Clinicians are obliged to treat the disorder. They should be alert to the potential high risk inherent this psychotic syndrome.
Keywords
Introduction
Dementia is one of the common mental health morbidities of the elderly population. It is conceptualized as a multifactorial process, 1 presenting a significant variability of clinical pictures. Progressive decline in cognition is the ultimate fate in dementia which is often associated with psychiatric manifestations in the form of apathy, 2 aggression, 3,4 depressive, 5 and other neuropsychiatric symptoms. 6 -8 A rarely reported feature of dementia is folie à deux (FaD), an intriguing condition of great relevance to the understanding of human psychopathology. In this article, we aim to describe the conceptual development of FaD including proposed etiologies and forensic concerns and review the scientific literature presenting the comorbidity of FaD and dementia.
Nosographic Questions
FaD is a challenging and fascinating yet poorly understood clinical syndrome. The term literally translates into “madness of two.”
Development of the Concept
The term FaD has been attributed to Lasègue and Falret, 9 who described a “psychiatric entity characterized by the transference of delusional ideas and/or abnormal behaviour from one person to one or more others who have been in close association with the primarily patients” 10 (p. 230). However, even before this syndrome was assigned a nomenclature, William Harvey (1651) presented a case of “phantom pregnancy” associated with FaD in 2 sisters who both believed that they could frequently feel the movement of the child as they occupied the same bed. 11 In 1860, the French psychiatrist, Jules Baillarger described the disorder as folie communiquée (communicated psychosis), while reporting a case in which 2 members of the same family were admitted to the hospital on the same day having similar delusions. The disorder continued to be described by French psychiatrists: In 1871, Legrand du Saulle reported “idée de persecution communiqué ou délire à deux et à trois personnes” (communicated persecutory idea or delusion of 2 and 3 persons), 12 and in 1880, Régis asserted that sharing delusions is possible between 2 individuals who have genetic disposition toward psychosis. 13 In German-speaking psychiatry, FaD was termed induziertes Irresein (induced psychosis) by Lehmann (1838). 14 Tuke (1888) categorized FaD according to the presence or absence of primary mental illness thus distinguishing between 4 presentations: (1) a delusion that is transferred from one mentally ill primary to a vulnerable secondary, who was not previously mentally ill; (2) a vulnerable secondary who becomes mentally ill and accepts a shared delusion subsequent to the shock of experiencing their family member’s delusional mental illness; (3) a shared delusion that arises concurrently, yet independently, in 2 individuals with simultaneous mental illness and similar symptomatology; and (4) any combination of these, including when an already mentally ill person takes on a new shared delusion from a primary, who is also mentally ill. 15 In 1942, Gralnick 10 also listed 4 subtypes of FAD:
Subtype A is termed folie imposée. Here, the dominant person with delusions imposes his or her delusions on a younger, more submissive person. Both persons are intimately associated, and the delusions of the recipient disappear after separation. Subtype B is termed folie simultanée and describes the simultaneous appearance of an identical psychosis which occurs in 2 intimately associated and morbidly predisposed individuals. Subtype C is termed folie communiqué. The recipient develops psychosis after a long period of resistance and maintains the symptoms even after separation. Finally, subtype D is termed folie induite and describes new delusions that are adopted by an individual with psychosis who is under the influence of another individual with psychosis. Depending on whether the delusions are shared among 2, 3, or 4 people, the condition is referred to as FaD, folie à trios, and folie à quatre, respectively. Rarely all family members share the same delusions, and this is called folie à famille. 16 Among the larger groups of individuals reported with FaD have been a group of eighteen 17 and a family of 12. 18 Folie à plusieurs (madness of many) arises when several individuals are willing to share the same psychopathology. The mass suicide in 1978 of over 900 members of the People’s Temple Cult, including their psychotic charismatic leader, Reverend Jim Jones, and 260 children, was probably an example of the latter phenomenon. 19 Jones’ followers were sucked into leader’s psychotic world: They believed that he was the Messiah and that by killing themselves they would be travelled with him to another planet and live a life of eternal bliss. 20 Various terms such as “inducer-induced,” “primary agent-recipient,” or “principal-associate” have been used to distinguish the partners of FaD. The content of the shared delusional beliefs may depend on the diagnosis of the primary case and can include bizarre delusions, or nonbizarre delusions characteristic of delusional disorder, and delusions congruent with mood. 21 All kinds of delusional contents can be seen in this disorder. 22 However, persecutory, religious, and grandiose themes are the most common. 23 -25 The acceptance of these beliefs results from a lack of critical evaluation by both members of the dyad. Hallucinations are most common in inducers, whereas they seem to be less frequent and less intense in recipients. 22,26 Dewhurst and Todd 27 listed 3 criteria generally regarded as prerequisites for the diagnosis of FaD: (a) evidence that the partners have been intimately associated, (b) identical or near-identical delusional content, and (c) acceptance, support, and sharing of each other’s delusional ideas.
Update of an Old Concept
Fundamentally, the nosology of FaD has changed little over the years. This phenomenon is also known by a number of different terms, including “induced delusional disorder” in the International Classification of Diseases, Tenth Revision 28 and “shared psychotic disorder” in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV). 29 International Classification of Diseases, Tenth Revision diagnostic criteria for FaD are 2 people share the same delusional system or delusion and support one another in this belief; they have an unusually close relationship and temporal or contextual evidence exist that indicates the delusion was induced in the passive member by contact with the active partner. In the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V), 30 shared psychotic disorder was removed as a separate disease entity and was included in the section on other specified schizophrenic spectrum and other psychotic disorders.
The Dyad
In FaD, one person, the dominant partner, initiates the delusions and the other, the submissive partner acquires them secondarily. It emphasized the preponderance of induced psychotic disorders in persons who live together intimately for a long time. 10 A review found that 98% of cases reported between 1993 and 2005 occurred within the nuclear family, usually between married or common-law couples (52%) or sisters (24%). 22 Fifty percent of the cases happen between the sister-sister and mother-daughter dyads. 31 -33 According to Gralnick, 10 about 8% of a series of cases occur among nonconsanguineous patients or friends. Additionally, there are case reports of physician–patient FaD 34 and even a case involving a dog. 33,35 Scharfetter 36 stated that the age range of the dominant partner is 16 to 82 years (average 38.5 years) and that of the submissive partner is 4 to 79 years (average, 36.2 years). It has been reported that the secondary case is characteristically younger, less intelligent, more gullible, and more passive, with lower self-esteem than the index case, although these findings have not been consistently replicated. 37 Imitation and persuasion are characteristic of the type of relations in the dyad. 38 The disorder usually starts with a difference in power and influence between the two, in which the one that induces the psychotic symptoms is the “real” psychotic and is an individual with energetic and active character. 21 According to Nielssen and colleagues, 39 the source of delusional content in the principal subject is generally conceived as reflecting endogenous processes and arising from the patient’s distinctive personal and natural history and particular vulnerabilities, whereas the source in secondary patients in FaD is purely exogenous. Individuals who develop shared psychosis often have suspicious, antisocial, dependent, and histrionic traits. 40 The degree of impairment is usually less severe in the secondary case(s) than in the index case. 41 The psychotic illness of the dominant person is most commonly schizophrenic, although other diagnoses may include delusional disorder or mood disorder with psychotic features. 42 Schizophrenia is thought to contribute to 58% to 60% of these cases. 26,42 -45 Only few cases in the literature report of FaD associated with bipolar affective disorder. 46,47 The recipient’s diagnosis may be multifactorial and many conditions including mental retardation, depression, dependent personality, physical disabilities, and sensory impairment have been reported. 48,49,50,51 Arnone and colleagues 22 described secondaries with comorbid diagnoses, including schizophrenia, dementia, and mental retardation, and stated that the so-called contagious effect of the primary in these cases was merely a temporal trigger for a psychiatric condition in already susceptible individuals.
Epidemiology
FaD is difficult to study in a controlled manner. Its epidemiology remains unclear because most of the data have been extrapolated from case reports. 52 Milder cases may not be recognized, and many delusional people strive to avoid psychiatric referral. Furthermore, the existence of a plethora of cultural belief systems sometimes makes distinguishing cultural beliefs from delusions a laborious task. 41 Another confounding factor is that social isolation often plays an integral role in the development of shared psychotic beliefs. 53 The true population prevalence is difficult to assess, as underreporting and underdiagnoses are likely to be considerable. Incidence rates of 1.7% and 2.6% have been found in consecutive admissions to a psychiatric hospital. 54,55 The disorder affects both genders equally and all age-groups. 26 These outcomes are in contrast with earlier theses that females had a higher risk of being affected. 10 Although rarely, its occurrence has been described in also children. 56 Cases have been reported from beyond western societies, including Nigeria and India. 57,58
Risk and Etiological Factors
Risk factors include longstanding social isolation and a very close relationship of the psychotic couple, as well as mental retardation of the secondary patient. 59 One of the most fertile grounds for the development of the disorder is social isolation, which is reported in 64.3% and 84% of the cases. 20 Possible risk factors for FaD identified in the literature include poverty 60 and shared traumatic life experiences. 61 The etiology of FaD remains a controversial topic. The etiological studies are grouped under 2 headings: (1) genetically transmitted structural factors and (2) environmental–psychological factors. There are several reports of monozygotic twins with FaD in the literature 51,62 -64 and many more of 2 affected siblings. 65 -69 It has been hypothesized that the genetic dispositions toward schizophrenia can also play an important role in the development of FaD, especially in the case of twins. 64 -71 In addition, it has been reported that individuals who develop FaD have a high risk of schizophrenia in their families, with a very high prevalence of schizophrenia in first-degree relatives (6.5%-26.2%), which is similar to the prevalence seen in first-degree relatives of schizophrenic patients (5.0%-16.9%). 21 Despite this evidence, the extent of genetic influence is difficult to determine. 26 Socioclinical substrates such as suggestibility and some cultural traits and religious beliefs could also provide the soil for the sharing of delusions. 44,71 Others have emphasized the role of imitation and sympathy in the causation of FaD. 10 Behavior based on beliefs induced by powerful suggestion in circumstances where a state of religious fanaticism or practices are potent and relevant factors is difficult to demarcate from shared delusional beliefs such as those occur in FaD. Enoch and Ball 72 sustained that, although there may be some reluctance to accept that the basic mechanisms operative in such cases (dominance-submission, identification and a need to cling together against a seemingly hostile world) may resemble those of FaD, nevertheless in some instances this certainly does appear the case. According to Salib, 73 folie à plusieurs might provide some explanation of al-Qa’ida’s bizarre and evil but meticulously calculated and executed suicide–homicide attacks on the United States in September 2001. To date, no single theory has been able to fully explain the etiology and pathogenesis of induced delusional disorder.
Forensic Aspects
After a crime is committed, psychiatrists may be asked by the defendant’s attorney to retrospectively evaluate whether the defendant was having a mental disorder and whether that mental disorder affected the defendant’s thinking and behavior around the time of the crime. 74 FaD has been associated with forensic and fatal consequences and it raises several questions of ethics that relate to autonomy, safety, and risk estimation. The disorder is a condition that presents distinct challenges in the legal system being one of many poorly validated psychiatric conditions that the legal system has dealt with over the years. It must be regarded as a serious, and potentially dangerous psychiatric disorder sometimes resulting in violence. 69,75,76 There have been several reports of forensic complications of “communicated insanity,” including theft, violence, attempted murder, and murder. One article describes the extraordinary case of 3 elderly, intensely religious sisters who developed a shared psychosis: folie à trois led to the horrible death of 2 of them, while the third sister lived for more than a year and a half with their mummified remains. 71 There are also cases of FaD associated with suicide pacts. 77,78 In these cases, the relations between the psychotic partners (domination–subordination) change over to relations of double suicide (instigator–participant). The challenge is in determining whether adopting another person’s delusional system is enough to support a diagnosis of mental illness or defect and thus can be used to establish the foundation for an insanity defense. Mental health experts undoubtedly differ in opinion, depending on their understanding of this condition and their individual beliefs about criminal responsibility. 52 Folie à deux resulting in violence creates uncertainty regarding the legal accountability of defendants, particularly the secondary partners, because many secondary patients abandon their delusional belief soon after separation from the primary. 41,52
Folie à Deux and Dementia
Cases of FaD involving elderly patients are reported quite infrequently. Apparently, the syndrome is similar in both old and young, but FaD relationships in the elderly seem to have a particularly strong interdependent and psychotic character, with a high ratio of folie simultanee.
79
Interestingly, the combination of FaD and dementia may have been reported in the fictional literature as early as the year 1604. Don Quixote, the eponymous hero of Miguel de Cervantes’ novel, Don Quixote de la Mancha, is described as a previously calm and righteous middle-aged Spanish nobleman who “was driven out of his wits” by excessive reading of books of chivalry and became convinced he was a knight errant. Don Quixote exhibits a constellation of symptoms that could possibly fulfill the clinical diagnostic criteria of modern day dementia with Lewy body disease. Specifically, he had evidence of polymorphic hallucinations and paranoid delusions, symptoms suggestive of fluctuating cognitive impairment and rapid eye movement sleep behavior disorder.
80
Sancho Panza, his squire, was initially skeptical but gradually accepted and completely shared Don Quixote’s delusional grandiosity. This leaves us with the combination of a dominant Don Quixote, who has lost his reason, and a submissive, not so bright Sancho Panza, thrown together through much of their adventurous travels. Therefore, some have hypothesized this to be a case of FaD.
81,82
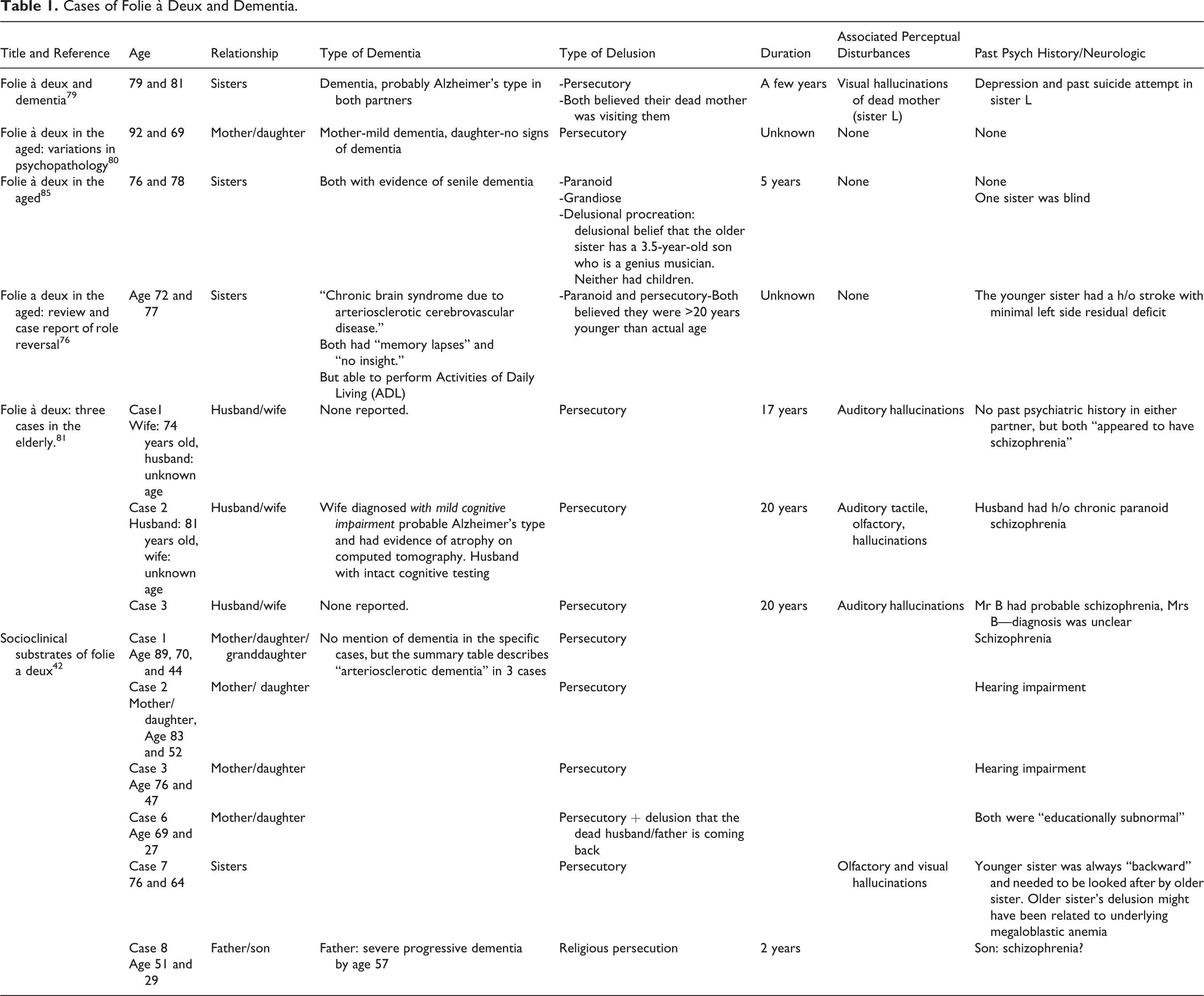
We intend to facilitate the comprehension of the disorder in persons having dementia by describing, in the subsequent paragraph, some cases drawn from the scientific literature. In the first example, Draper and Cole
83
described a case in which both partners with FaD had Alzheimer’s disease (AD). L, a 79-year-old widow, was living with E, her 81
Cases of Folie à Deux and Dementia.
Prognosis and Therapeutic Approaches
Treatment of FaD can be both complicated and difficult because frequently only 1 member of the shared delusional system presents for therapy. Commonly, the inducer’s primary illness is treated with antipsychotic medication. 86 In some instances, the primary condition is affective in nature 47 and an antidepressant drug and/or mood stabilizer may be indicated. Most authors agree that separation of the patients is a crucial intervention in the management of this disorder. 47,87 However, cases with fatal outcome after separation have been reported, suggesting, in some situations, separation might increase risk of adverse outcomes. 23 Once successful treatment of the pathologic processes is completed, the physician must utilize adequate social supports to treat the susceptible relationship between the partners in an effort to prevent a recurrence. The goal of such intervention is to increase the autonomy of the enmeshed partners. 88 Unfortunately, few published studies have examined the outcome of different treatment approaches.
Conclusions
The phenomenon of FaD has been a topical issue in neuropsychiatry for more than a century. It poses several dilemmas for clinicians, mental health experts, and legal professionals. Little is known about its incidence and prevalence or its optimal treatment. Although infrequent, FaD has been reported in patients with dementia, and physicians should be aware of the phenomenon and not overlook it.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.