
Abstract
This quasi-experimental, nonrandomized study examined the feasibility and impact of a multicomponent (MT) intervention on 7 community-dwelling individuals diagnosed with probable Alzheimer’s disease (AD) at mild to moderate stage. During 6 months, patients with AD and their caregivers were submitted to a biweekly exercise program, including muscle strengthening, aerobics, balance, and postural exercises. The following tests were used: Senior Fitness Test and Incremental Treadmill Test, Disability Assessment for Dementia Scale, Alzheimer Disease Assessment Scale–Cognitive, and Quality of Life–Alzheimer’s. Attendance and retention mean rates were high (86% and 78%, respectively). No adverse events occurred. Results revealed a significant beneficial effect on cardiorespiratory fitness (P = .028), upper (P = .018) and lower (P = .026) body muscle strength, agility (P = .018), and ability to perform daily activities (P = .018). Data suggest that a biweekly MT intervention is feasible to conduct in patients with AD. Findings also suggest a potential positive effect on mitigating cognitive decline and in positively influencing quality of life.
Keywords
Introduction
Dementia affects around 50 million people worldwide, and in every 3 seconds, someone develops it. 1 In 2012, the World Health Organization placed this pathology as a public health priority, 2 and the recent Draft Global Action Plan 3 highlights the existing gap between eminent needs and the actual provision of prevention, treatment, and care for dementia.
Aging is the major risk factor for Alzheimer’s disease (AD), the most common cause of dementia that may contribute to 60% to 70% of all cases worldwide. 1 Alzheimer’s disease represents one of the major causes of dependency and disability among the elderly individuals. 4 This progressive and irreversible disease has a significant impact on diagnosed individuals, which is extended to informal caregivers and to the community itself. 5 Moreover, it leads to significantly increased cost for governments, particularly in low- and middle-income countries. 3
Along with the cognitive decline that characterizes AD, this neurodegenerative disease adversely affects the physical condition and progresses along with functional impairment on activities of daily living (ADLs). 6 The available pharmacological treatment is unsatisfactory, 7 emphasizing the need to implement effective interventions to minimize the impact of AD—either delaying its progression or reducing its symptoms. 8
Recent studies have emphasized the impact of physical inactivity on the increased risk to develop dementia 9,10 and particularly AD. 11 According to the American College of Sports Medicine (ACSM), 12 physical exercise contributes to reduce the development and progression of chronic diseases, including those associated with the aging process and related to cognitive and physical functions. Although several studies reported the benefits of exercise as a preventive measure against AD, 11,13 the therapeutic role of exercise as an adjuvant nonpharmacological strategy after AD diagnosis needs further evidence. 6
Nevertheless, several key issues, including methodological incongruence, heterogeneity of results, and absence of specific recommendations, compromise the planning and/or prescription of an exercise intervention for elders with AD. 6,14 Viability assessment of pilot interventions is therefore needed to understand the exercise adherence, safety, attendance, main barriers, and intensity monitoring, 15 which are essential to implement effective community-based exercise programs. 16 Additionally, innovative aspects such as including caregivers on exercise sessions as participants need to be explored, 15 as this is an innovative aspect when we are not focused on domiciliary contexts. 16 –19
Multicomponent training (MT) seems to be effective at improving functional and cognitive performances in older healthy adults living in the community 20 –22 and in older adults with neurodegenerative disorders. 23 This type of exercise intervention usually combines aerobic, strength, and postural exercises 20 and seems to have a great adherence and satisfaction among elders. 21 Results from our group previously demonstrated the efficacy of an MT intervention on cognitive function and physical fitness on institutionalized elderly patients diagnosed with dementia due to AD. 24
However, from our knowledge, there is a need to assess both the effectiveness of an MT intervention in older, community residents diagnosed with mild to moderate AD and the related exercise adherence, attendance, and safety. As proposed by the Medical Research Council, 25 pilot studies are important to assess the viability to carry out a complex intervention such as a full-scale randomized controlled trial (RCT). Several methodological aspects were piloted for a planned future RCT.
The present pilot study aims to analyze the feasibility of a community-based MT intervention for individuals diagnosed with AD and their caregivers and complimentarily explore its impact on physical fitness, functionality (ADL), cognitive function, and quality of life.
Methods
Participants
Sample recruitment occurred for 9 months prior to the beginning of the study, and through this process, 13 individuals were selected to participate in this quasi-experimental, nonrandomized study. The patients were clinically diagnosed with probable AD according to National Institute of Neurological and Communicative Disorders and Stroke and Alzheimer’s Disease Related Disorders 26 and at mild or moderate stage according to the Mini-Mental State Examination (MMSE) 27 and the Clinical Dementia Rating (CDR). 28,29 The diagnosis and the stage characterization were conducted by a team of physicians from the Neurological Department of a hospital center located at the north of Portugal.
The eligible participant pool was restricted to older adults presenting the following inclusion criteria: (i) age ≥60 years; (ii) community living; (iii) not engaged in a regular exercise training (ie, planned and organized activity practiced systematically) during the year prior to this study; (iv) independent mobility; (v) inexistence of past medical history of major depression, bipolar disease, schizophrenia, or other neuropsychiatric pathologies; and (vi) lack of any diagnosed or self-reported musculoskeletal or cardiovascular disorders that contraindicate participation in moderate exercise and testing.
The investigation was in full compliance with the Helsinki declaration, 30 and the ethical commission approval has been sought from the institutional review boards that took part in the intervention.
After initial screening, individuals diagnosed with AD and their caregivers received a complete explanation of the purpose, risks, and procedures of the study and signed a written informed consent. Two individuals refused to participate during the first physical evaluation, one individual was institutionalized at a nursing home, and the caregiver of another showed unavailability to attend training sessions. Nine individuals voluntarily accepted to participate in the exercise intervention.
An adaptation period before the training program was considered, which had the main purpose of promoting familiarization with exercises, socialization between participants, and the management of the caregiving dyads. During this period, 2 participants were unable to continue due to transportation unavailability and significant manifestation of behavioral and psychological symptoms of dementia. Seven community-dwelling individuals diagnosed with mild to moderate AD completed the exercise intervention.
Sociodemographic and clinical characteristics of all participants were assessed through a questionnaire fulfilled by the caregiver. The International Standard Classification of Occupations 31 was used to categorize each participant’s occupation before retirement.
Exercise Intervention
The 7 community-dwelling individuals diagnosed with mild to moderate AD (AD1 to AD7) completed a 6-month exercise program following the recommendations of the ACSM for healthy older adults, 32,33 including aerobic, muscle strengthening, balance, and postural exercises with 2 sessions per week on nonconsecutive days. Caregivers have participated as class members on exercise sessions, although the focus was patients with AD.
Patients with AD and their caregivers were subdivided into 2 smaller groups (6 and 8 participants, respectively) and submitted to the same exercise program to assure their full participation and motivation. Group sessions took place in a specific sport facility located at one of the partners’ institutions and lasted for 60 minutes; the same exercise trainer, specialized in working with older adults with neurocognitive disorders, conducted each session. The sessions were divided into 3 main parts: warm-up (8-10 minutes, including postural and stretching exercises), specific training (40-45 minutes, including 10-15 minutes of aerobic exercises—eg, mostly walking and transporting light objects; 10-15 minutes of strength exercises—eg, weight lifting or calisthenics; and 10-15 minutes of coordination or balance training—eg, tandem walks or exercises shifting direction), and cool down (5-10 minutes with respiratory and stretching exercises).
To increase exercise program’s efficiency and attractiveness, regular similar routines that included spatial orientation activities and/or corporal perception and laterality were established during warm-up. An illustrative example of this is the fact that all exercise sessions began with an initial walking on a preestablished perimeter, and the range of motion/stretching exercises were performed on a circle position. The variety of different exercises used during each session was restricted and familiar to patients with AD, since the majority reproduced daily activities—such as chair sit and stand or climbing stairs.
Additionally, some cognitive tasks were promoted whenever appropriate through colors, shapes, numbers, objects, and exercises that mimic daily living activities. In other words, whenever it was possible, a cognitive challenge was introduced without disturbing the performance and execution of physical exercises in patients with AD (eg, transporting all the objects with a specific color from one side of the room to the other as fast as they could). During the adaptation period, this type of dual-task activities was not prioritized; hence, the main purpose was to instruct patients with AD about the correct execution of exercises.
Assessment of Feasibility
Feasibility was assessed based on the overall suitability to conduct this pilot study, including adherence, retention, attendance, and safety analysis; level of exercise intensity achieved; and improvements in physical fitness, functionality on ADL, cognitive function, and quality of life.
Adherence was assessed considering the number of individuals who have accepted to participate in the study relative to the number of participants who were recruited, and from these, the ones who have completed the study—retention.
A 70% minimum attendance rate to the exercise sessions was required. Attendance rate was calculated as a percentage of the number of exercise sessions completed by participants by the full amount of sessions they were expected to perform throughout the study. The attendance levels were 71% or over. Reasons for missing exercise sessions were registered.
Safety was evaluated based on the occurrence of adverse events during sessions or related to each exercise. Additionally, the intensity of exercise was measured with objective measures. Accelerometry and heart rate were monitored using ActiGraph GT9X Link, during exercise sessions of the last month of the intervention, to ensure the safety of participants and evaluate whether the proposed intensity level of training was achieved. According to the established intensity limits for old people, 34,35 in this study, more than 70% in light-to-moderate intensity level was considered as a target purpose.
Concerning the heart rate assessment, a cardio frequency meter associated with the accelerometer was used during the 6 exercise sessions. Medium heart rate during exercise sessions and the percentage achieved considering the theoretical maximum were analyzed. Based on Tanaka et al’s 36 age-predicted equation 208 − (age × 0.7) to calculate maximal heart rate for healthy older adults, a maximal heart rate of 55% to 70% corresponds to a moderate intensity of exercise 37 and was the safety criteria assumed for this intervention.
Outcome Measures
All following measures were assessed at baseline and after 6 months of exercise intervention: Senior Fitness Test (SFT), Disability Assessment for Dementia Scale (DAD), Alzheimer Disease Assessment Scale–Cognitive (ADAS-Cog), and Quality of Life–Alzheimer’s Disease Scale (QoL-AD). Additionally, cardiorespiratory fitness was objectively assessed with a maximal testing method to determine peak of oxygen consumption (
Physical Fitness
The SFT 38 battery is considered a reliable instrument for assessing physical fitness in older adults (≥60 years old) including those with cognitive impairment. 39,40 The following physical parameters were evaluated: lower body strength (chair-stand test), upper body strength (arm curl test), aerobic endurance (2-minute steps test), and agility/dynamic balance (8-foot up and go test).
Peak oxygen consumption provides a quantitative measure that reflects the efficiency of several body systems and is an indicator of performance and health.
41
In the presence of an exercise physiologist,
Functional Capacity
The DAD 47 was developed to assess functional disability in community-dwelling individuals with dementia due to AD. The Portuguese version was validated by Leitão and Santana, 48 and it is a measure of the actual performance on ADL over a 2-week period previously to the assessment moment. The ability to perform basic, instrumental, and leisure activities was analyzed through an interview with caregivers and took approximately 15 minutes each. A highest result as final percentage indicates less disability on ADL.
Cognitive Function
The ADAS-Cog, 49 Portuguese version, 50 was used to assess cognitive function. It takes about 40 minutes to complete and is composed of 11 cognitive tests that cover several cognitive areas: memory, orientation, praxis, language, attention, and concentration. 51 Scores range from 0 to 70, with higher scores suggesting greater severity of cognitive impairment.
Quality of Life
The QoL-AD 52 was used to measure the quality of life of patients with AD. The questionnaire included 13 items such as physical health, energy, mood, memory, family, marriage, friends, and ability to do things for fun. The QoL-AD provides the participant and the caregiver reports of the participant’s QoL and is scored on a 4-point Likert-type scale ranging from 1 to 4 (excellent), with total scores ranging between 13 and 52 points.
Statistical Analysis
Statistical analyses were conducted with the SPSS IBM Statistical Software version 23.0 for Windows with a significance level of .05. Impact of the intervention was tested using the Wilcoxon signed rank test. Results are expressed as mean and standard deviation (SD).
Results
Characteristics of the Participants
Sociodemographic and clinical characterization of the participants are summarized in Table 1. The sample included 7 participants with AD at mild (n = 5) to moderate (n = 2) stage according to the MMSE (17-25 points) and CDR (1-2 stage). The majority (71%) were female and with low educational level (≤4 years). Individuals’ professions were categorized according to the International Standard Classification of Occupations. 31 Diabetes mellitus, hypertension, osteoarticular, or other cardiovascular diseases were main complimentary diagnosis.
Characterization of Participants.
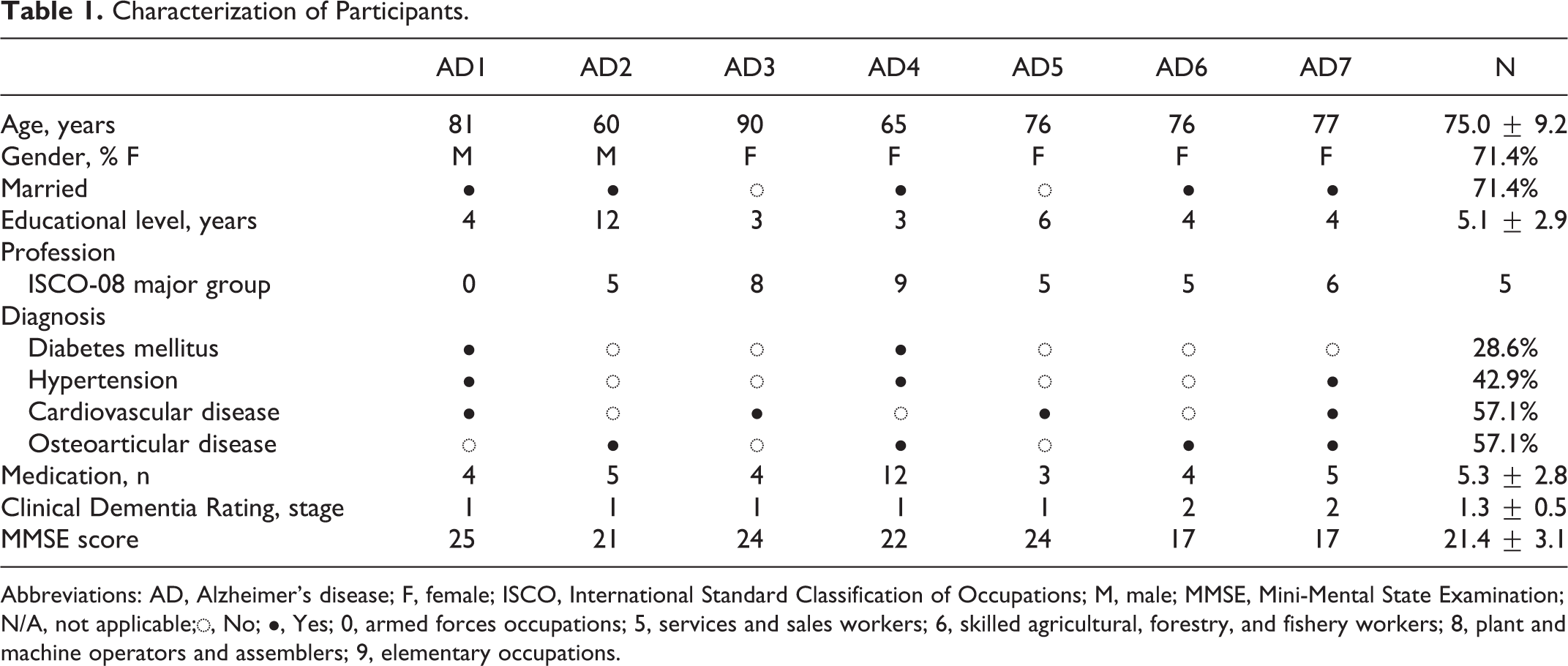
Abbreviations: AD, Alzheimer’s disease; F, female; ISCO, International Standard Classification of Occupations; M, male; MMSE, Mini-Mental State Examination; N/A, not applicable;◌, No; ●, Yes; 0, armed forces occupations; 5, services and sales workers; 6, skilled agricultural, forestry, and fishery workers; 8, plant and machine operators and assemblers; 9, elementary occupations.
Adherence, Retention, Attendance, and Safety of the Exercise Intervention
As previously stated, from the 13 individuals initially recruited, 9 accepted to participate in the exercise intervention, representing 69.2% of adherence rate. Moreover, from the initial exercise group of 9 patients with AD, there were 2 dropouts only during the adaptation period; therefore, the retention rate was 77.8%.
Forty-eight exercise sessions were conducted, in which the mean session attendance rate was 86.4% (Table 2). The main reasons for missing exercise sessions were caregiver unavailability due to work, acute disease, and/or family issues (43.5%); acute disease of the patient with AD (41.3%); participation in another sociocultural activity (8.7%); or other reason (6.5%).
Attendance Rate and Exercise Intensity: Descriptive Values for Level of Activity and Heart (Average Value During Exercise Sessions and % From Individual Maximal Heart Rate).
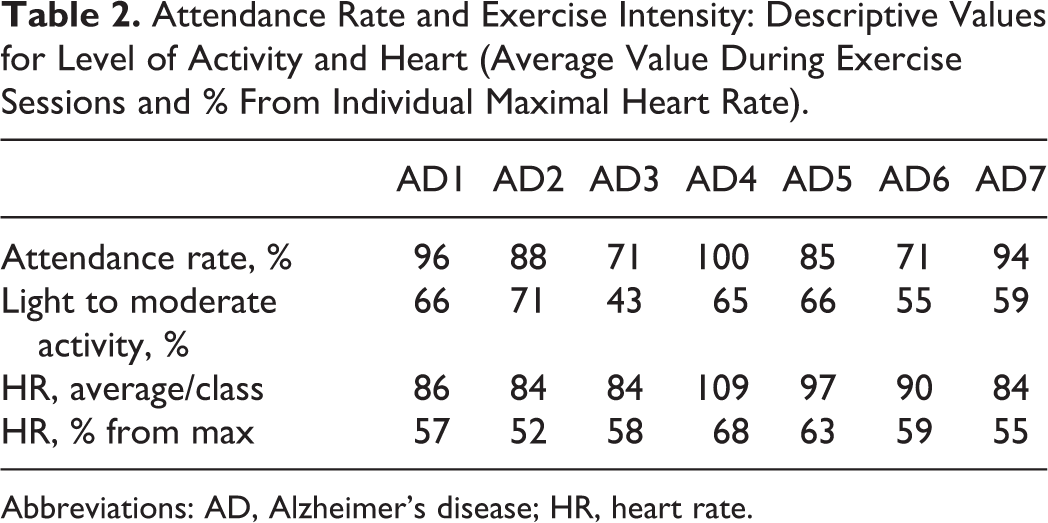
Abbreviations: AD, Alzheimer’s disease; HR, heart rate.
Table 2 presents the individual attendance rate to exercise sessions, level of activity, and medium heart rate. Safety was assessed based on the occurrence of adverse events and intensity. No serious adverse events were observed during this exercise program over a period of 6 months, and none of the participants revealed side effects directly or indirectly related to exercise.
The exercise intensity was measured using an accelerometer and a cardio frequency meter, during 6 exercise sessions. As it can be seen in Table 2, for most individuals, the mean percentage of the maximal heart rate achieved during the exercise sessions was above 55% and considered in moderate intensity level. 37
Body Composition, Physical Fitness, and Functional Capacity
Analyzing the differences between baseline and postintervention results for body composition of patients with AD who participated in the exercise intervention, no statistical differences were observed (Table 3). For physical fitness measures, data suggest a positive effect of this MT intervention on the participants’ upper and lower body strength, aerobic endurance, and balance, based on the increasing repetitions for chair stand (P = .026), arm curl (P = .018), 2-minutes step tests (P = .028), and the decrease in time spent on 8-foot up and go test (P = .018). Additionally, for
Mean (±SD) Values for Preintervention and Postintervention Results for Anthropometric Measures, SFT, DAD, and Peak Oxygen Evaluation.
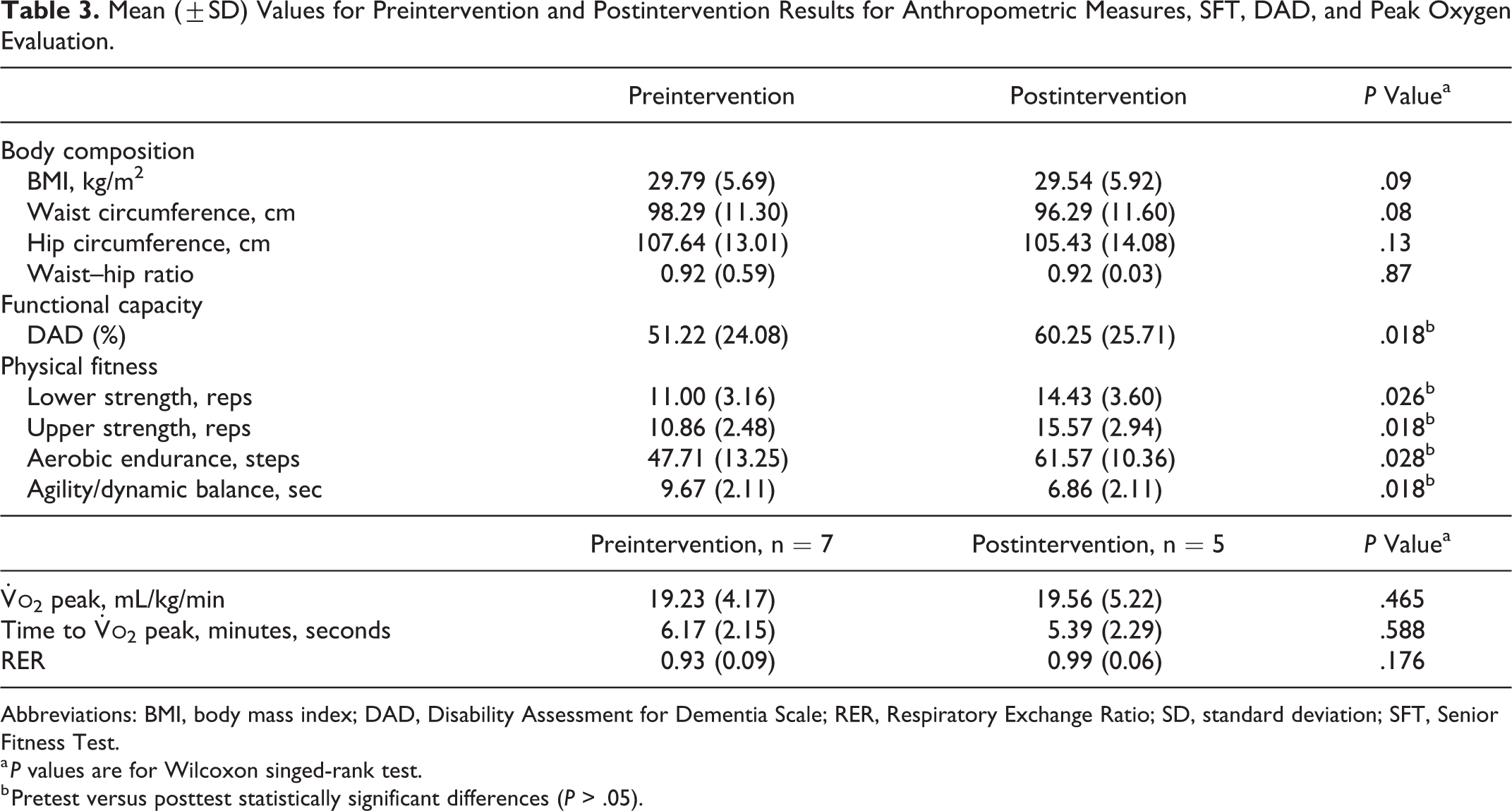
Abbreviations: BMI, body mass index; DAD, Disability Assessment for Dementia Scale; RER, Respiratory Exchange Ratio; SD, standard deviation; SFT, Senior Fitness Test.
a P values are for Wilcoxon singed-rank test.
b Pretest versus posttest statistically significant differences (P > .05).
Results from both evaluation moments suggest that cardiorespiratory fitness for some patients with AD is under the established partners for independent healthy older adults. 53,54 Regarding the functionality on ADLs, data suggest a potential positive effect (P = .018) of the 6-month MT intervention on patients diagnosed with mild to moderate AD (Table 3).
Cognitive Function and Quality of Life
The MT intervention has not promoted differences in cognitive function nor quality of life for patient with AD between baseline and after 6-month intervention (Table 4).
Mean (±SD) Values for Preintervention and Postintervention Results for ADAS-Cog and QoL-AD.
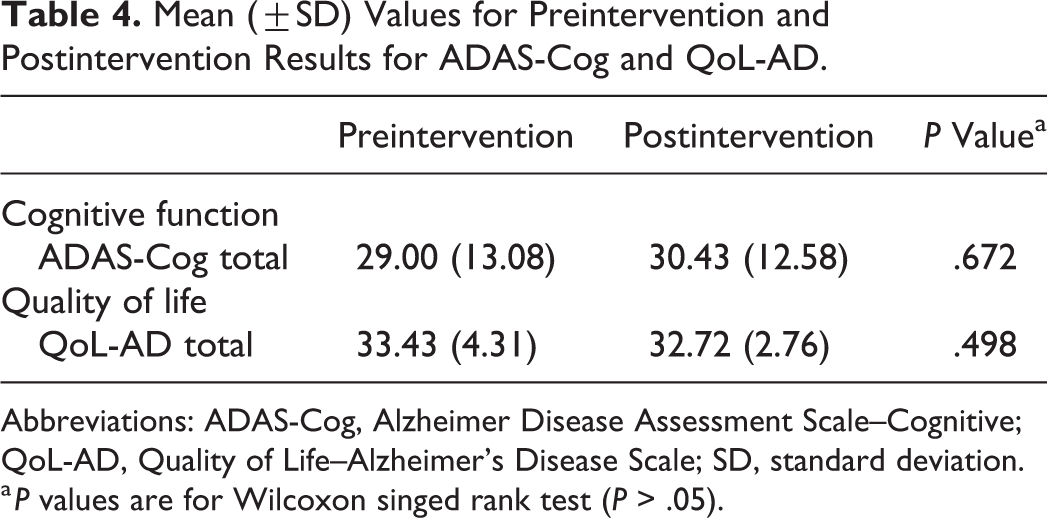
Abbreviations: ADAS-Cog, Alzheimer Disease Assessment Scale–Cognitive; QoL-AD, Quality of Life–Alzheimer’s Disease Scale; SD, standard deviation.
a P values are for Wilcoxon singed rank test (P > .05).
Individual changes in cognitive function can be observed in Figure 1. However, it is not possible to suggest an effect of exercise on mitigating the cognitive decline associated with AD due to nonstatistically significant difference on ADAS-Cog test (P = .672).
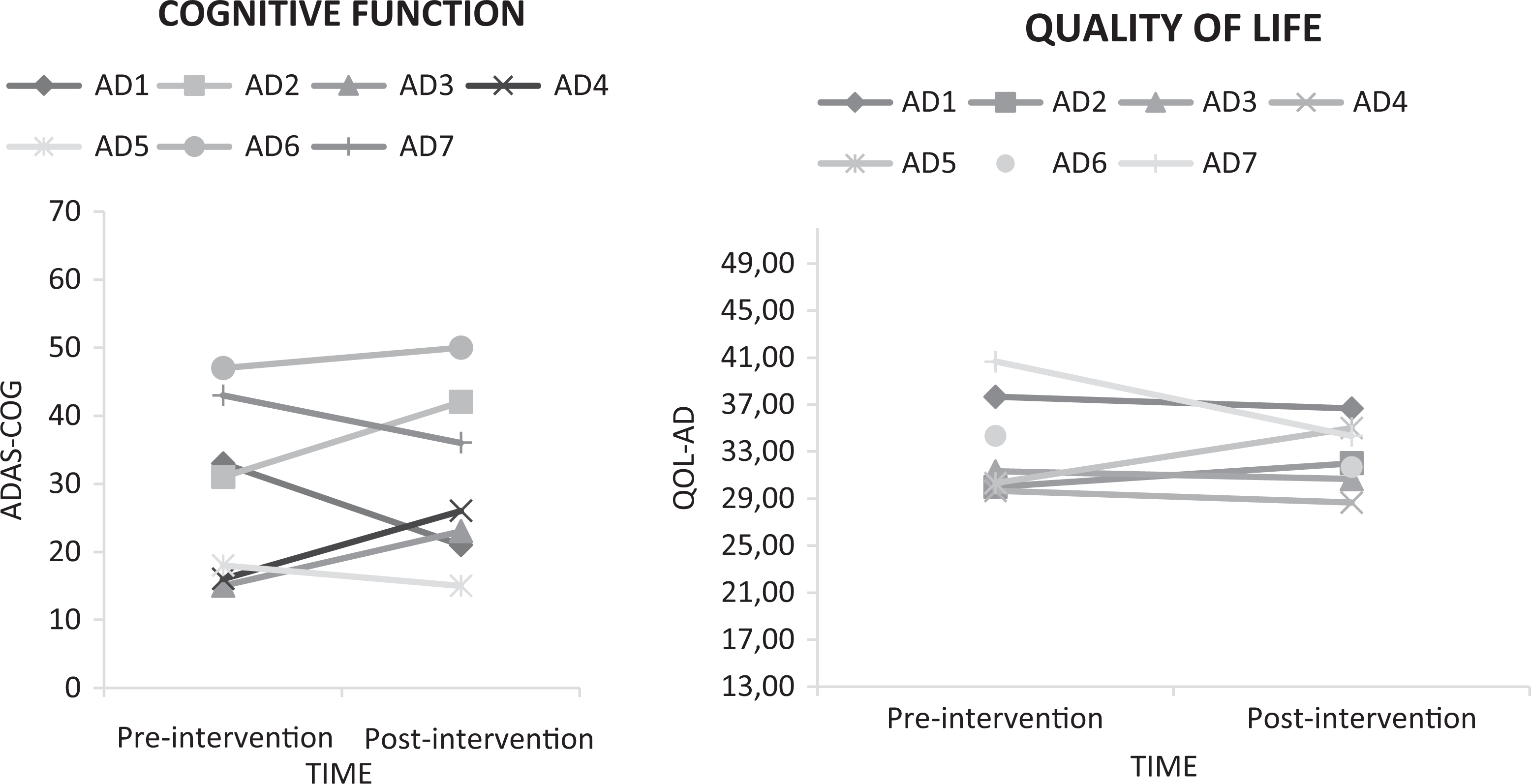
Cognitive performance and quality of life (QoL) at preintervention and postintervention.
Likewise, although quality of life of patient with AD has not decreased after 6 months, as presented in Figure 1, it is not plausible to suggest a possible positive effect of this MT intervention.
Discussion
This pilot study showed that this 6-month MT exercise program for community-dwelling older individuals with mild to moderate AD is feasible and safe. We observed high rates of adherence and retention and that no adverse event has occurred. The high attendance rate suggests that the number of sessions per week, the duration of training sessions, and length of the intervention period were adequate, as previous similar interventions studies have confirmed. 24,55 Following reasons should be considered regarding the difficulty to reach the target intensity levels: participants’ safety, high potential for distraction, and management of the caregiver’s role. 16 This group-based intervention required minimal equipment.
The inclusion of the caregiver as a participant on exercise sessions is one of the novelties of the present study and can help to explain the high adherence to this program. This emphasizes the caregiver as a crucial element on the success of this type of interventions, not only due to practical reasons (eg, providing transport and establishing exercise sessions on AD patients’ routines) but mainly because of emotional and motivational/satisfaction reasons. 16,56
Regarding the exercise protocol, only few experimental studies have addressed older adults with neurodegenerative syndromes, including AD. 24,55,57,58 Although aerobic training is the most frequent exercise methodology applied 6,59 due to the well-studied brain health benefits, 60,61 recent systematic review studies highlighted the potential larger effect of MT exercise on cognition when compared to resistance or aerobic training alone. 23,62 Furthermore, MT training methodology has been identified as efficient in preventing functional decline and promoting sociopsychological well-being in community-dwelling older adults. 20,21
In what regards the purpose of assessing the viability of a 6-month, community-based MT exercise program for individuals with mild to moderate AD, our secondary findings suggested that this intervention has benefited patients with AD on their functional fitness outcomes and on their ability to perform daily activities. Postintervention results have shown a positive effect on upper and lower body strength, aerobic endurance, and agility/dynamic balance. However, no body composition differences were observed at the end of the intervention.
Several studies have shown the positive impact of exercise among older adults with AD, 63,64 and our study results seemed to reveal similar trends. As highlighted by other authors, 33 our results hypothesized that the increased ability to perform the 30-second sit to stand test and the arm curl test seems to have an impact on the ability to perform basic ADLs, probably due to the decrease in fatigue, increase in muscle function, and independent mobility. 22
Cardiorespiratory fitness has been directly associated with different health-related parameters,
44,65
brain health,
66,67
neurocognitive performance, and ability to perform ADL
45,68
which has significant impact on autonomy and progression of dependence of patients with AD and caregivers’ quality of life. However, just few trials have addressed the cardiorespiratory effects of exercise in patients with AD using a treadmill incremental test.
15,44,69,70
Morris and collaborators have addressed a limited/variable physiologic response of individuals with early AD to aerobic exercise relative to cognitively normal elders.
45
However, our data suggest a slight increased
As previously stated, several studies have shown the MT effectiveness on improving functional fitness capacities in older adults with dementia 24,57 ; however, to the best of our knowledge, its efficacy on AD community-dwelling patients and on ADL functionality has been less well studied. Postintervention results from this pilot study suggest a positive impact on ADL independence. Considering that the majority of individuals diagnosed with dementia are community-dwelling elders, the improvement in their autonomy and independency levels may significantly minimize the family burden, health-care costs, and delay institutionalization. 71 –73
Despite the observed differences in functionality and ADL performance in the postintervention moment, results from ADAS-Cog and QoL-AD did not report significant differences. In being a neurodegenerative disorder, AD is characterized as a progressive and irreversible cognitive decline. 1 Therefore, a better performance on ADAS-Cog was not to be expected after an exercise program intervention, but the maintenance of cognitive function outcomes is considered a positive effect. 23 The small sample size, the low volume and/or intensity of training, 62 and/or type of exercise 59 should be considered.
Furthermore, unlike other pilot studies 74,75 and systematic reviews analysis, 76 the current study did not observe a significant effect on quality of life of patients with AD. The relationship between exercise and perception of QoL is complex, and it is possible that other unmeasured variables can explain the no-effect of MT intervention in this specific population.
This pilot study design has some limitations that do not allow the evaluation of determinant aspects to proceed with an RCT as the randomization process—due to the absence of control group—and as the viability of a multicenter setting design study. Regardless of these aspects, and of the small sample size, this study has several strengths, including the social impact of this community extended university study; the promotion of cognitive stimulation and use of routines; the inclusion of caregivers as class members, which enabled a greater involvement by the patient; the familiarization and adaption period to the exercise program; the use of performance-based tests to objectively evaluate fitness; the monitoring of exercise intensity with heart rate monitors and accelerometers; and the viability assessment of training protocol and other methodological aspects as instruments adequacy.
This pilot study may represent an important contribution to the literature, since it proves that it is feasible to carry out a 6-month community MT intervention that is specifically designed for AD caregiving dyads. In general, it revealed to be a feasible training modality that is highly recommended for older individuals, as it resulted in beneficial improvements in physical fitness and functionality on ADL performance. These methodological findings are crucial for a future RCT. Although these findings provide some potential to the MT probable effect on community-dwelling patients with AD, additional evidence is needed to validate and build upon our findings with a larger sample and using additional clinical outcome measures.
Future Research Recommendations
Further research is necessary to identify the most effective exercise modality for people with different types and severity of dementia in terms of type, frequency, intensity, and duration and to identify standard instruments to allow comparisons between studies. Additionally, well-designed RCTs should be conducted and consider a multicenter recruitment process from several hospitals, primary care services, and community dementia services, as they could represent an important advance in the selection of patients with AD and their caregivers. In addition, in future RCT, concerning the control group, a social activity intervention should be considered, as it can be more effective for participant retention purposes and represent a more accurate ethical procedure. Along with MT interventions for this specific population, other adjuvant nonpharmacological therapies and exercise programs should be recommended and promoted by clinicians as a possible cost-effective approach to attenuate dementia progression and disease-related symptoms.
Footnotes
Acknowledgments
The authors would like to cordially thank Ana Rita Barbosa and Tiago Montanha, respectively, for conducting the exercise sessions with patients with AD and their caregivers and for conducting the cardiorespiratory fitness tests. The authors would also like to thank CIAFEL—Research Centre in Physical Activity, Health and Leisure (UID/DTP/00617/2013), Instituto Português do Desporto e Juventude—“Mais Ativos Mais Vividos” Program and to the project “Body and Brain” (POCI-01-0145-FEDER-031808).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.