
Abstract
Introduction:
Supplementary tests are part of the clinical approach to diagnose cognitive impairment. We aimed to determine the role of supplementary examinations, except for biomarkers, on diagnostic stability of dementia over time and to identify reversible dementias.
Methods:
We identified 432 patients with dementia who performed 2 clinical evaluations and the supplementary examinations recommended by the American Academy of Neurology in a follow-up period of 1 year.
Results:
In this sample, 110 (24.5%) patients changed their diagnosis at 1-year follow-up for the appearance of vascular cognitive impairment than the initial diagnosis, due to the neuroimaging. Concerning the reversible dementias, depression was the major differential diagnosis, detected in 13 (81%) of the 16 patients with cognitive improvement.
Conclusion:
Therefore, regarding the supplementary examinations only neuroimaging and the depression triage were relevant for clinical practice regarding the differential diagnosis of dementia.
Keywords
Introduction
The term “dementia” does not denote a disease 1 but a syndrome characterized by a progressive deterioration in the cognitive function, more commonly the memory, but also of other domains such as speech, praxis, visual perception, and executive functions can be affected. 2
As for any neurological disease, the right diagnosis is the key for the pharmacological treatment, if available, and for proper care, orientation, and familial planning.
Due to the variability in sensitivity and specificity of the diagnostic criteria, and due to the growing need for accurate diagnosis for clinical research and appropriate orientations, supplementary examinations are more and more expected to assist with and confirm diagnostic suspicions, as well as to exclude reversible diseases that might simulate them—the so-called reversible dementia.
With this purpose in mind, the last revision by the American Academy of Neurology 3 on the parameters used to diagnose dementia was published in 2001, which instructs that all patients should obtain a cranial computed tomography (CT) scan or magnetic resonance imaging (MRI), a depression triage scale such as the “Geriatric Depression Scale” (GDS), 4 dosing of Vitamin B12, thyroid-stimulating hormone (TSH), and venereal disease research laboratory test (VDRL) for those with a risk factor, or residing in an endemic area. In endemic areas, the European guideline also recommends the serology for HIV 5 and, more recently, the systematic sleep analysis, particularly in the search for the obstructive sleep apnea syndrome (OSA). 6 The request of a complete blood count, blood urea concentrations, creatinine, albumin, hepatic enzymes alanine aminotransferase, aspartato aminotransferase and gama glutamyltransferase, and calcium, in order to exclude misleading clinical and psychiatric causes, is also widely recommended. 3,5,7
Considering the significant increase in the occurrence and prevalence of patients with dementia reaching 47 million people in 2015, which is expected to triple until 2015, particularly in developing countries, 8 and considering the progressive increase in the requests for supplementary examinations available, added to the progressive reduction in the time for clinical assessment with anamnesis, physical examinations, and neuropsychological triage, it is important to demonstrate how and when the supplementary examinations, except biomarkers, can make a difference in the investigation and the treatment of dementia. The purpose of this study is to determine the role of the supplementary examinations in dementia diagnostic approach. The primary end point is providing useful tools for the diagnosis of dementia, and the secondary end point is using these tools also to exclude reversible syndromes.
Methods
Participants
A review was carried out with all medical records from the Service of Cognitive and Behavioral Neurology of the Department of Neurology and Neurosurgery of the Federal University of São Paulo, between 2000 and 2015. The evaluations of each patient and the completion of each medical record were made by neurologists, geriatricians, psychiatrists, or residents supervised by a board-certified clinician, accompanied by neuropsychologists from that service. All medical records were evaluated by a single researcher.
Criteria for inclusion were: 1-year follow-up with at least 2 medical visits. Clinical Dementia Rating (CDR) ≥ 1.0 and ≤ 2.0. Diagnosis defined by the end of the follow-up period. Medical file duly completed. Presence of a family member or companion.
Criteria for Exclusion were: Less than 1-year follow-up. CDR < 1.0 or > 2.0. Diagnosis not defined by the end of the follow-up period. Incomplete data on the file. Absence of a family member at the appointments.
Assessment
A data collection file was elaborated to include sociodemographic data. Then, the reported complaints from patients (self-report) and family or relatives were assessed and divided into the following domains: memory, speech, executive function, behavior, visual–spatial, perception, and gait. The neurological examination was classified according to the changes that contribute to the differential diagnosis of dementia (parkinsonism signs, ataxia, frontal release signs, limb and eye apraxia, pyramidal signs, and extra ocular movement tests). 9 The beginning of clinical onset, as well as the psychiatric, vascular, and nonvascular background, was described. The CDR, 10 the Neuropsychiatric Inventory, 11 and the Functional Activities Questionnaire 12 were included based on informant’s descriptions.
All patients underwent neuropsychological tests in the first evaluation, which include the Mini-Mental State Examination (MMSE), 13 the Consortium to Establish a Registry for Alzheimer’s Disease battery test, 14 the verbal fluency within 1 minute with fruits and animals, 15 the clock drawing test, 16 the digit span, 17 and the drawing of the Rey complex figure and figure recall 18 from which it was possible to determine the cognitive domains indicated as altered in the tests (short-term memory, long-term memory, speech, executive function, and visual–spatial functions). The MMSE and the CDR of the first evaluation were recorded for comparison with these same data collected after 1 year of follow-up. The neuropsychological tests were standardized based on their validity in the Brazilian population and on their intra- and interrater reliability.
According to the specific international criteria of each disorder, the diagnoses were defined in the first medical appointment and 1 year after the supplementary examinations. The depressive disorder was triaged with the application of the Brazilian version of the GDS, with 15 items (GDS 15). 19 The mandatory examinations for the differential diagnosis of dementia were considered relevant (TSH, B12, VDRL, HIV, cranial CT scan or MRI, and when available, single-photon emission computerized tomography [SPECT], polysomnography, liquor routine [opening pressure, determination of protein, albumin, immunoglobulin, glucose, lactate, and cell count and cytology, as well as specific antigen and antibody testing for infectious agents], and electroencephalogram [EEG]).There was no use of biomarkers on spinal fluid or imaging due to its unavailability in our health public system during the follow-up period. For the primary end point, it was considered any change in the diagnosis and for the secondary end point any reduction in the CDR score. The study was approved by the research ethics committee of the Federal University of São Paulo. There were no funding related to this study.
Statistical Analysis
In the description of data, the qualitative variables were summarized to absolute frequencies (n) and relative frequencies (%); the quantitative variables were expressed as the average ± standard deviation, median, minimum, and maximum values. In order to identify the factors associated with the primary and secondary end points related to the diagnostic change, binary logistic regression models were used. At first, the isolated effect of each variable was investigated by simple logistic regression (single-variant analysis). The variables with P < .10 in the single-variant analysis were included in a multiple logistic regression (multivariate analysis). Based on the complete multivariate model (with all variables selected by the single-variant model), a reduced model was adjusted to consider only the variables with P ≤ .05. The significant level considered was .05. The results were presented in odds ratio and respective 95% confidence intervals. Cases in which a change in diagnosis (primary end point) and/or reduction in the CDR (secondary objective) were found were evaluated individually in order to identify the examination(s) related to such difference. The statistic software used in all of the analyses was SPSS 19.0 for Windows.
Results
From a total of 1485 patients evaluated by the Service of Cognitive and Behavioral Neurology of the Department of Neurology and Neurosurgery of the Federal University of São Paulo between 2000 and 2015, 432 patients were selected in accordance with the inclusion and exclusion criteria.
The demographic and clinical characteristics are described on Table 1. In the initial evaluation, 263 (60.9%) patients presented mild dementia (CDR 1.0) and 169 (39.1%) patients presented moderate dementia (CDR 2.0). After at least 1 year of follow-up, 204 (47.2%) presented CDR 1.0, 160 (37%) presented CDR 2.0, 52 (12%) presented CDR 0.3, and 16 (3.7%) presented CDR 0.5. The initial MMSE average was 18.2 ± 5.4 with a median of 18.0, evolving to 17.1 ± 6.7 with a median of 18.0 after 1 year.
Demographic and Clinical Characteristics.a
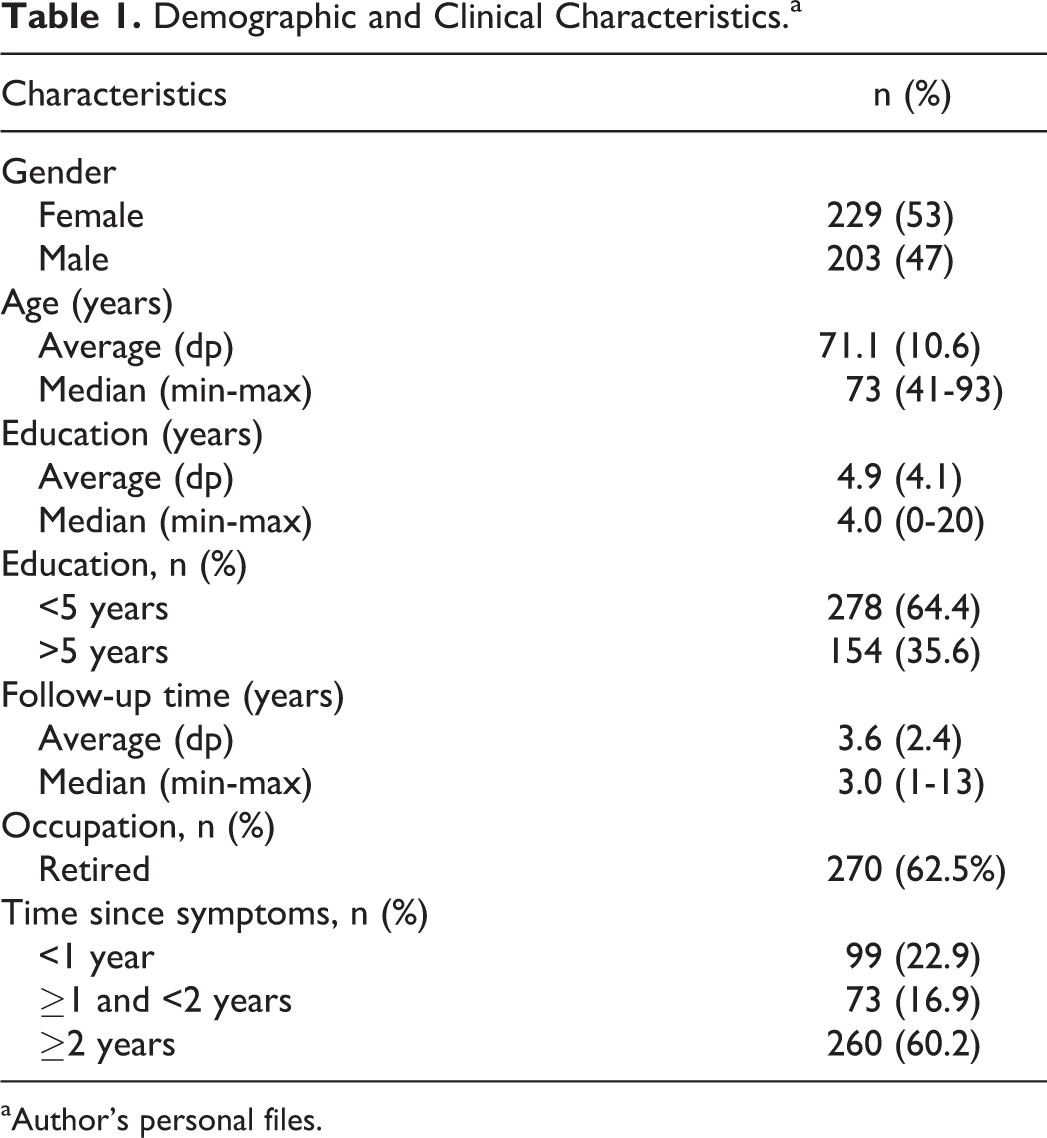
aAuthor’s personal files.
Table 2 discriminates the initial and final diagnosis of the sample. There was a decrease in the number of patients with only 1 diagnosis after the minimum 1-year follow-up from 82.6% at first to 66.4% after 1 year. At the end, 140 (32.4%) patients received 2 diagnoses, and 5 (1.2%) patients received 3 diagnoses.
Distribution of Diagnoses After the Follow-Up Period (%).a
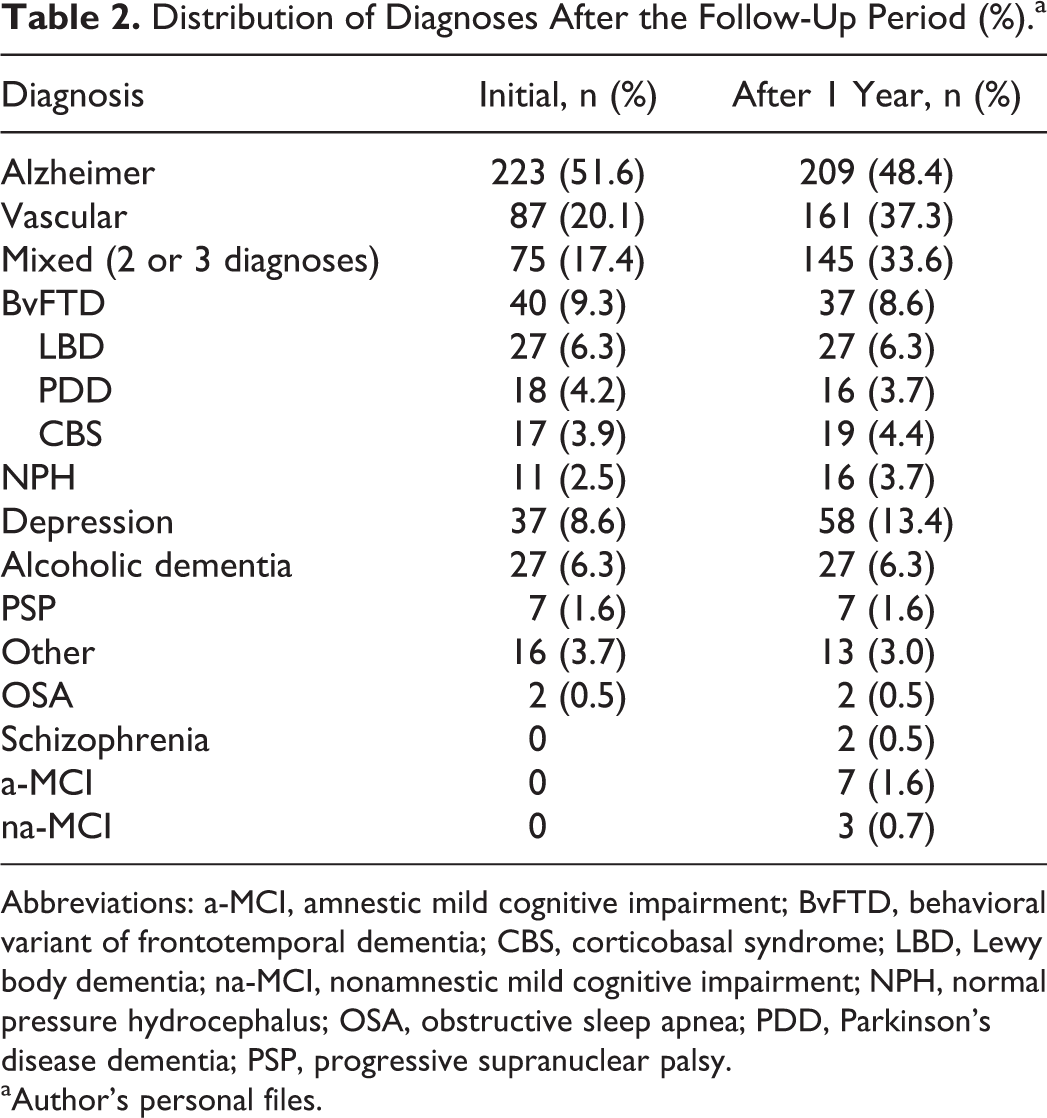
Abbreviations: a-MCI, amnestic mild cognitive impairment; BvFTD, behavioral variant of frontotemporal dementia; CBS, corticobasal syndrome; LBD, Lewy body dementia; na-MCI, nonamnestic mild cognitive impairment; NPH, normal pressure hydrocephalus; OSA, obstructive sleep apnea; PDD, Parkinson’s disease dementia; PSP, progressive supranuclear palsy.
aAuthor’s personal files.
Table 3 assesses the concordance (κ) between the initial and final diagnoses. Table 4 shows the number of patients submitted to examinations and their results.
Kappa Correlation Between Initial and Final Diagnoses.a
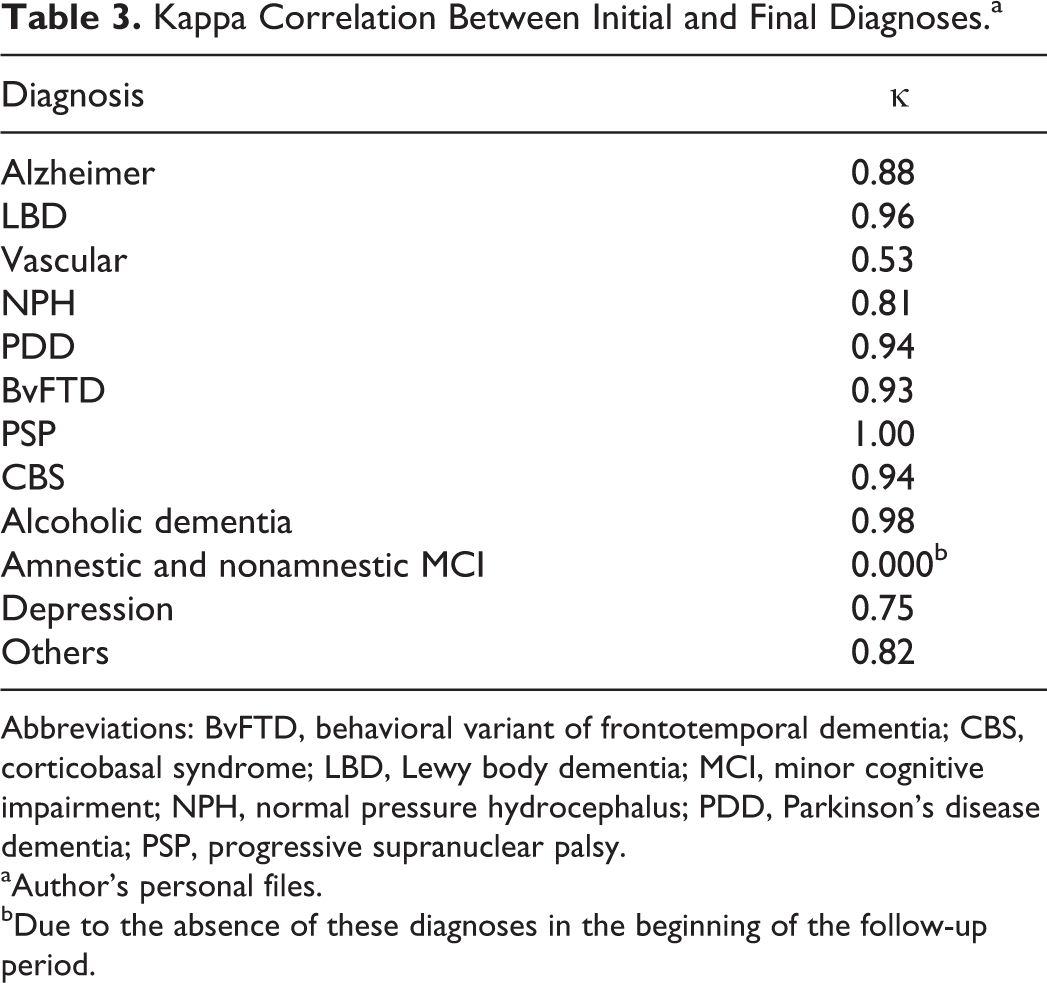
Abbreviations: BvFTD, behavioral variant of frontotemporal dementia; CBS, corticobasal syndrome; LBD, Lewy body dementia; MCI, minor cognitive impairment; NPH, normal pressure hydrocephalus; PDD, Parkinson’s disease dementia; PSP, progressive supranuclear palsy.
aAuthor’s personal files.
bDue to the absence of these diagnoses in the beginning of the follow-up period.
Results of the Supplementary Examinations, Performed, and Nonperformed.a ,b
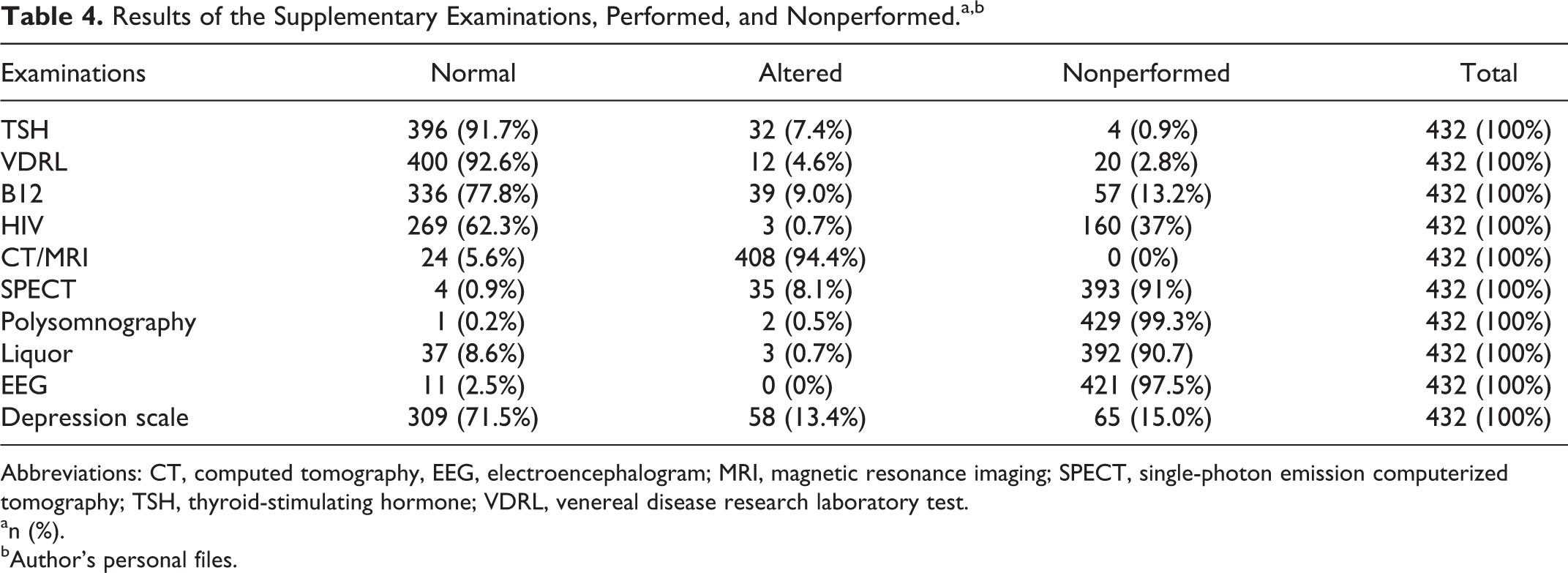
Abbreviations: CT, computed tomography, EEG, electroencephalogram; MRI, magnetic resonance imaging; SPECT, single-photon emission computerized tomography; TSH, thyroid-stimulating hormone; VDRL, venereal disease research laboratory test.
an (%).
bAuthor’s personal files.
Considering the primary end point related to diagnostic stability, from the total of 432 patients, 110 (25.4%) had their diagnoses altered by the examinations. The examinations that showed a significant role for the primary end point and thus for the diagnosis of dementia were structural imaging examination (107/110 patients—97.3%), triage for depression (15/110—13.4%), SPECT (6/110—5.5%), liquor routine (07/110—6.4%), and polysomnography (2/110—1.8%). Venereal disease research laboratory test, vitamin B12, TSH, HIV, and EEG did not contribute to the change in the diagnoses of patients.
The 3 patients who had their diagnoses altered, independently of the examinations, were initially diagnosed with primary progressive aphasia (PPA). Two of them progressed to the corticobasal syndrome (CBS) and 1 of them to the behavioral variant frontotemporal dementia (FTD).
Considering the secondary end point related to reversibility of the dementia after at least 1-year follow-up and the supplementary examinations carried out, from 432 patients, 288 (66.7%) had no comorbidities found, and 144 (33.7%) patients had comorbidities related to cognition impairment. Nine from the 144 (2.1%) were not treated. Those patients were diagnosed with idiopathic normal pressure hydrocephalus (iNPH) with CDR ≥2 or with a negative Tap Test. The remaining 135/144 were treated accordingly.
From the sample of 432 patients, 24 (5.7%) had a reduction in the CDR score. Sixteen (3.7%) patients from the 24 had a CDR reduction of 0.5 (CDR 1.0-0.5) and the remaining 8 had a CDR reduction of 1 point (CDR: 2.0-1.0). It is important to stress that 20 from the 24 patients who had a CDR reduction were treated for the comorbidities found, meanwhile 4 patients had a CDR reduction of 1 point (2.0-1.0) treated only the dementia with anticholinesterase inhibitors. From the 16 that had a reduction in the CDR score from 1.0 to 0.5 after treatment, 8 had only change in the depression triage with normal neuroimaging, 3 had a surgical treatment for iNPH as their only finding, 3 presented with severe microangiopathy in CT/MRI and depression, 1 had depression and OSA, and 1 had depression, OSA, and hypothyroidism.
Discussion
This work assessed the role of supplementary examinations in the differential diagnosis of demential syndromes in an expressive sampling of 432 patients in a Brazilian reference hospital. The longitudinal assessment was relevant for the completion of the ancillary examinations and diagnostic review after at least 2 medical evaluations. Based on the results found, it is clear that, except for neuroimaging and depression triage, none of the other examinations considered to be mandatory had a direct relationship with the final diagnosis or the cognitive status after at least 1-year follow-up. The use of biomarkers was not added in this work due to its unavailability in Brazilian public health system, the lack of local parameters and the lack of formal indications. 20
As a primary end point, the diagnostic change occurred in 110 (25.4%) of the 432 patients. Among these patients, the main reason was the addition of the vascular disease as a contributor, or even as a final demential diagnosis, passing from 87 (20.1%) patients to 161 (37.3%) patients , leading to an 85% increase in the vascular dementia cases after the minimum 1-year follow-up. The depression triage was also relevant in the differential diagnosis, as depression was initially understood as comorbidity or even ignored, but later showed to be a significant cause of the cognitive loss demonstrated by the improvement after proper treatment. The increase value was 62%, from 36 (8.3%) patients to 58 (13.4%) patients . Other 3 patients demonstrated change regardless of the examinations.
The examinations with isolated impact on the diagnosis of dementia change were structural imaging examinations (CT/MRI), depression triage, and SPECT. Liquor, and polysomnography, contributed to the change only when associated with other examinations. On their turn, vitamins B12, VDRL, TSH, HIV, and EEG did not contribute to the change in the diagnoses of patients.
Assigning an underlying pathological process to a patient with dementia is essential for clinical practice and research. However, few works have discussed so far the diagnostic evolution of patients with dementia in a longitudinal manner. To this date, we have identified only 1 study related to the diagnostic stability of patients with dementia. 21 Other studies are related to early-onset dementias, 22 mild cognitive impairment (MCI), 23 or the clinical–pathological correlation. 24
Koepsell et al 21 performed a prospective evaluation of 4141 patients from 32 centers in the United States, from 2005 to 2009, who presented a clinical diagnosis of dementia or MCI. The patients were evaluated at least twice, with an interval of at least 1 year, as done with our sample. The objective of the study was to evaluate the stability of the diagnosis of dementia and evaluate the factors related to such stability. Most of the patients (91%) had the same diagnosis in at least 2 medical appointments. Older patients (older than 70 years), non-white patients, patients with milder conditions (CDR 0.5 or 1.0), lower education level (<80 years), patients with more than 1 initially associated comorbid diagnosis, patients not accompanied by close family members, and patients evaluated by different physicians in the 2 medical appointments presented a higher chance of change. The main changes were caused by vascular disease, depression, and clinical change independent of examinations, which is exactly the data found in our sample.
Koepsell et al 21 describes that the diagnoses that presented the highest concordance were those of atypical Parkinsonism (progressive supranuclear palsy [PSP] κ = 0.78, CBS κ = 0.79, and Lewy body dementia [LBD κ] = 0.77) and PPA (κ 0.76). On the other hand, diseases with lower concordance between the initial and final diagnoses were depression (κ 0.46) and vascular dementia (κ 0.69), while the latter presenting a 35.5% increase in diagnoses as a final comorbidity. Likewise, in our sample, atypical Parkinsonism had the highest diagnostic stability (PSP κ 1.0, Lewy 0.96; CBS 0.94), whereas vascular dementia and depression had the lowest correlations between the initial and final diagnoses (κ: 0.53 and 0.75, respectively; Table 3).
The importance of the vascular and depressive cognitive impairment was made evident for the diagnostic stability/change in this sampling. However, a small group of patients presented diagnostic changes independent of the examinations. Three patients had the initial diagnosis of PPA and evolved to CBS or FTD after at least 1 year. What may initially seem to be random may actually hide a paradigmatic change in the study of demential syndromes. The new approach that attempts to unify the circuitry and the molecular pathology is referred to as molecular nexopathies. 25 This approach is about a pathological construction that unifies the study of pathogenic proteins, using biomarkers, and the characteristics of vulnerable brain networks and connections that are going to define the signature and progression of each demential syndrome.
The secondary end point was to evaluate the role of the supplementary examinations in determining reversible dementia. In this study, from 432 patients, 144 (33.8%) show evidence of potentially reversible dementia cause; however, after treatment, only 16 (3.7%) had a sufficient improvement of the cognitive status to reach a CDR score of 0.5 and only 8 (1.8%) had a partial recovery with a reduction of the CDR score from 2.0 to 1.0. The 2 main reversible diagnoses were major depression and iNPH. The only tests therefore that had an isolated impact were CT/MRI, for the possibility of iNPH (3/16 patients), and the depression triage (13/16 patients). Venereal disease research laboratory test, vitamin B12, HIV serology, and EEG had no role, while polysomnography (2 patients), TSH (1 patient), and SPECT only had an impact when associated with depression. The spinal fluid contributed only on confirmation of iNPH, not being relevant for the reversibility when altered. None of the 12 patients with a positive VDRL had changes in spinal fluid or MRI to confirm neurosyphilis. None patient in our sample with alcoholic dementia presented with spontaneous improvement after withdrawal, although the literature suggests reversibility up to 21% of the patients. 26
The prevalence of the reversible causes is hard to define due to the misconception about cognitive deficits and by the diversity of the environment where the data are gathered ranging from specialized clinics to geriatric nurseries and general hospital to the community justifying the wide range prevalence of 0% to 77%. 27 However, the prevalence in most studies revolves around 1.5% to 6%, reaching 20% in MCI. The most common cause in the literature is depression; followed by drugs, alcohol, brain tumors, or hematomas; iNPH; and metabolic conditions. 28
Hej et al 29 evaluated prospectively 1000 patients with MCI and dementia in a memory clinic states a prevalence of 19% of reversible conditions in MCI and 4% in dementia. Three main causes were (corresponding 82% of the patients) depression, iNPH, and alcoholism. In 1 meta-analysis regarding 32 articles with 2889 patients, Clarfield 30 found a frequency of 13.2% of reversible causes. In 1995, Weytingh et al 27 published a review of 16 studies and found a range from 0 to 37.5% (mean 15.2%). A more recent study, 28 with 116 outpatients, showed a high prevalence of possible reversible causes (31.2% in new cases and 18.2% in ancient cases). Depression was the most prevalent (13.1%), followed by B12 deficiency (9.8%), NPH (8.2%), and alcoholism (3.3%). However, as in our study, after proper treatment, only depression and iNPH reversed. It was analyzed also metabolic changes such as renal, hepatic, ionic, or hematological. As expected, their correction did not result in benefit for cognition.
Besides all difficulty in defining the prevalence and the real conditions that can be considered reversible causes of dementia, it gets even blurrier when one try to identify the real benefit of the treatment intervention. Weytingh et al 27 found a mean frequency of 15.2%. After treatment, only 1.5% showed complete reversion, 9.3% partial recovery, and 4.2% no change. Walstra et al 31 in a prospective study of 170 elderly demented patients showed a prevalence of 19% of reversible causes, and none of the patients had a complete recovery after proper treatment. In the same direction, a Brazilian study 32 enrolling 275 outpatients, revealed 22 (8.0%) patients with possible reversible conditions. The 2 main diagnosis were syphilis, (9 cases) and hydrocephalus (6 cases). Full recovery were observed in only 2 (0.8%) patients and partial in 10 (4%) patients.
Regarding partial recovery, it is worth to highlight that from the 8 patients in our study whose CDR score changed from 2.0 to 1.0, 4 were treated for depression overlapping dementia and 4 had a change only using cholinesterase inhibitors for vascular and Alzheimer’s dementia. This improvement is described in these 2 types of dementia and related to better survival rates. 33 It is clear, therefore, by the literature and reinforced by this article, that there is a big difference between looking for and preventing common comorbidities in the elderly patients and believing that the laboratory test will change the diagnosis or detect reversible causes of dementia. Although we did not considered the neuropsychological assessment or triage a supplementary examinations due to its huge importance as part of the basic medical evaluation, it must be stressed, as recently reported in literature, that it can be another diagnostic tool useful to discriminate irreversible from reversible dementia, as iNPH. 34
This work presents some limitations that must be taken into consideration. As for the sampling, it involves a reference center that receives patients previously evaluated by other services, which reduces the clinical and neurosurgical causes typically described by works done in primary services. For the same reason, random and systematic errors are likely to decrease with the reproduction of this kind of this study in a multicenter environment including different settings and tests. One example is that a percentage of supplementary examinations were not carried out. For instance, 15% of patients were not evaluated with the depression scale and 13% of patients did not have their b12 vitamin serum level measured. It must be emphasized that this work was based on the clinical diagnosis (possible or probable) and not pathological diagnosis (definite). 24 The use of spinal fluid or imaging biomarkers is established as a diagnostic tool in the differential diagnosis of dementia; however, due to its unavailability in our health public system and lack of standardized parameters in our population, it was not included in our analysis. Finally, to consider only the CDR score as benefit for the comorbidities treatment may be undermine the power of the interventions.
For the patients with typical dementia syndromes, the use of indiscriminate supplementary examinations, except for neuroimaging and depression triage, brings little additional diagnostic information, which is not true for atypical cases or MCI with a broader differential diagnosis. Considering that developing countries will have the highest prevalence of dementia in the world, 8 one of the most significant unfolding of this work is to emphasize the importance of the quality of the medical training, so that we can do a good use of the examinations in our hands and even better use of the clinical skills needed for an accurate diagnosis and proper care of the patient and his family. In addition, this work urges a public health policy that contemplates the cardiovascular and mental health as pillars in prevention and treatment of the dementia syndromes.
Footnotes
Authors’ Note
The study was approved by the Research Ethics Committee of the Federal University of São Paulo, Brazil.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.