
Abstract
Background:
Asia has the greatest population and more patients with dementia in the world. Early recognition of clinical symptoms of Alzheimer’s disease (AD) is crucial for dementia care. In order to foster collaboration in AD care, a uniformed manner to report the early clinical symptoms of AD is necessary.
Methods:
We have recruited clinically diagnosed patients with AD at their very mild stage with Clinical Dementia Rating (CDR) 0.5 in Taiwan, Japan, China, Philippines, and Singapore. Demographic characteristics and psychometrics including Ascertain of Dementia-8 (AD8) questionnaire were administrated to collect and report the clinical presentation in these countries.
Results:
In total, 713 clinically diagnosed patients with AD at very mild stage, CDR 0.5, have been recruited from these 5 countries. “Repeats questions, stories, or statements” were consistently the frequently reported symptom across these countries. Taiwan, China, and Singapore have the higher AD8 total score compared to that in Japan and Philippines. Japan and Philippines have the gender-related differences in clinical presentation of early AD.
Conclusion:
Difficulties in using small trouble appliance and in handling complicated financial affairs were frequently reported in Japan female, compared to male, patients with AD. Identifying the clinical symptom of AD and the gender-related issues would be crucial in the dementia care in Asia.
Introduction
Alzheimer’s disease (AD) has been becoming one of the major impactions to the socioeconomic status in currently aged society. 1 -3 Although current treatments cannot totally cure it, the early diagnosis and treatment still be the golden standard to the care of AD. 4,5 Unfortunately, most patients with a dementing illness do not report cognitive problems or symptoms of dementia to their health-care providers and their family until several years after the symptoms worsen. The recognition of dementia by primary care physicians will be made until it is moderately advanced. 6,7 Lacking confidences for a physician to make the diagnosis of dementia are frequently met. 8 -10 In order to compensate the possible delayed diagnosis of dementia, the screening test or questionnaire with high sensitivity and specificity was recommended to achieve these goals. 11 Not only to capture dementia but also to capture dementia at its early stage are crucial in the dementia care. For such purposes, 3 stages of AD were proposed, preclinical stage of AD, mild cognitive impairment (MCI) due to AD, and AD. 12 Mild cognitive impairment due to AD, early stage of AD, has become a target for early diagnosis and treatment. Some psychometrics have been proposed and administrated for its capability in telling MCI from others. 13 -15 However, these psychometrics are necessary to be conducted by an experienced neuropsychologist with a required space and time and have to compare the testing results to norm, which is not easy and practicable to be used in routine clinic or in general population. Meanwhile, whether these psychometrics were related to genders were less addressed because male patients with AD more frequent exhibit apathy and anxiety, while delusion was more common in female patients. 16 -18
Ascertain of Dementia 8 (AD8) developed from Washington University, 19 which is capable of screening AD with higher sensitivity and specificity, even at its early stage, Clinical Dementia Rating (CDR) 0.5, has been extensively used and validated in several versions. 20 -24 In other words, AD8 can screen AD at its very mild stage with high sensitivity and specificity; these reported symptoms in AD8 questionnaire could be the early symptoms of AD.
The clinical symptoms of dementia would be related to the various cultural features, 24 -26 and could be related to gender, 27 but are not well examined in Asia, especially in a uniform manner. In order to foster and collaborate for AD study and care, we initiate a study to report the gender-specific clinical symptoms of very mild stage AD through AD8 in 5 Asian countries.
Materials and Methods
The study had initiated by Dr Yuan-Han Yang at Taiwan from 2012 till 2014. Participants were recruited from hospitals in Taiwan, China, Philippines, and Singapore, and from community in Japan.
All participants from Taiwan were recruited from several longitudinal projects conducted at the Department of Neurology, Kaohsiung Municipal Ta-Tung Hospital in southern Taiwan. Other recruited participants were from Philippines by Dr Jacqueline Dominguez, from Singapore by Dr Christopher Li-Hsian Chen, and from Beijing, China, by Dr Huali Wang. The diagnosis of AD was based on the Diagnostic and Statistical Manual of Mental Disorders IV (DSM-IV) criteria 28 with referring to the comprehensive medical evaluation, including clinical history, physical and neurological examinations, neuroimaging study, and blood chemistry examinations.
Participants from Japan were recruited from the Kurihara Project (2008-2010), 29 a community-based stroke, dementia, and bed-confinement prevention program for old–old adults, defined here as aged 75 years or older, in Kurihara, an agricultural town in Miyagi Prefecture, northern Japan. The diagnosis of AD was made by DSM-IV criteria with reference to magnetic resonance imaging and laboratory tests.
The ascertainment of AD with its clinical stage or nondemented status was made in accordance with the rule of assignment of a CDR score 30 by the senior neurologist or psychologist. A CDR score of 0 indicates no dementia and 0.5, 1, 2, and 3 very mild, mild, moderate, and severe dementia, respectively. The clinical diagnosis of AD is confirmed pathologically in 93% of cases, 30,31 even when diagnosed at the CDR 0.5 level, the earliest symptomatic stage of AD. 31
All procedures in Taiwan were approved by the institutional review board of the Kaohsiung Medical University Hospital, and written informed consents were obtained from all participants or their legal representative. For other recruited participants in other countries, each researcher in his country has got the approval from ethic committee. For each recruited participant, a series of neuropsychological assessments, including Mini-Mental Status Examination (MMSE), 32,33 CDR, 30 and AD8, 21 were administered by a senior neuropsychologist and an experienced physician based on information from a knowledgeable collateral source (usually a spouse or adult child). The staging of AD was ascertained with CDR. 30 The clinical symptoms were denoted as any of subitems of AD8.
Statistic
Data analysis was performed using SPSS (version 12.0.1 for Windows, SPSS Inc, Chicago, Illinois). All statistical tests were 2 tailed and an α of .05 was taken to indicate significance. Analysis of variance test was used to compare the age, education, MMSE score, and AD8 total score with its each subitem among these 5 countries for all recruited very mild stage AD. χ2 Examination was used to compare the gender and gender in relation to each subitem of AD8 among these countries.
Results
In total, 713 participants have been recruited, in which 201 from Taiwan, 292 from Japan, 70 from China, 85 from Philippines, and 65 from Singapore. For all recruited participants, the mean age (standard deviation [SD]) was 76 (7.4) years, education was 8.0 (4.0) years, MMSE was 22.0 (4.7), AD8 total score was 2.7 (2.3), Sum of Boxes of CDR (CDR-SB) was 1.7 (1.1), and the mean percentage of gender was female 60.9%. Gender (P = .023), age (P < .001), education (P < .001), MMSE (P < .001), AD8 (P < .001), and CDR-SB (P < .001) were significantly different among these countries (Table 1). The participants with AD from Japan were the oldest with age (80.4 [4.3]) among these countries in contrast to Philippines (70.5[7.4]), who were the youngest. For all recruited participants, female still consistently has the greater proportion across these countries, compared to male. The detailed demographic characteristics of these recruited participants are illustrated in Table 1.
Demographic Characteristics of CDR 0.5 Very Mild Stage of Alzheimer’s Disease.
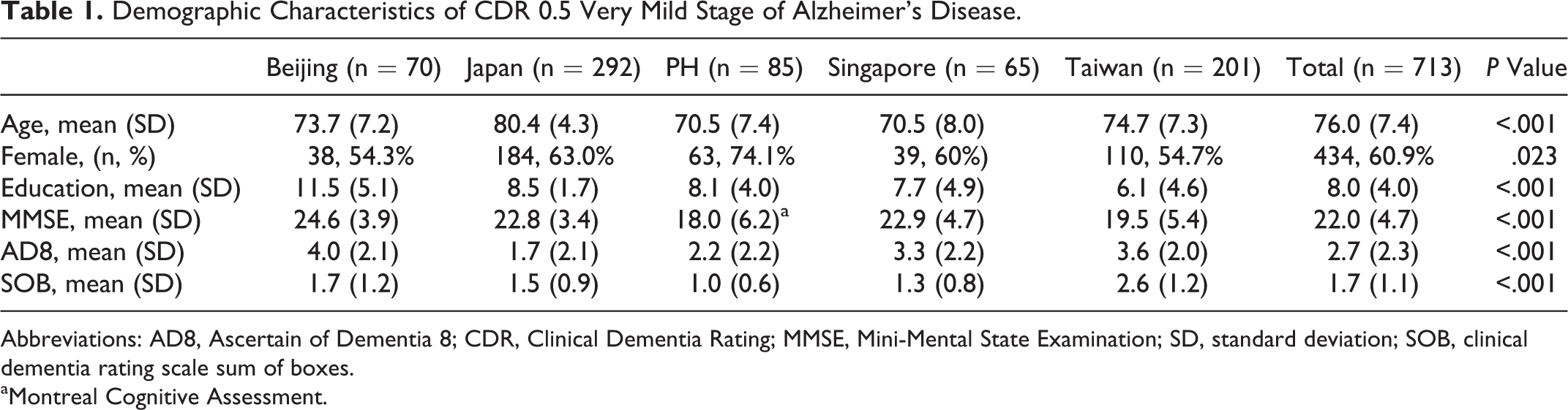
Abbreviations: AD8, Ascertain of Dementia 8; CDR, Clinical Dementia Rating; MMSE, Mini-Mental State Examination; SD, standard deviation; SOB, clinical dementia rating scale sum of boxes.
aMontreal Cognitive Assessment.
In the distribution of AD8 subitems in CDR 0.5 very mild stage of AD, all reported subitems of AD8 were significant among all countries (P = .004 to <.001; Table 2). In Beijing, the top 2 frequently reported subitems were AD8-3 (60.0%): repeats questions, stories, or statements and AD8-8 (60.0%): consistent problems with thinking and/or memory, which were similar to those in Taiwan where AD8-3 (67.2%) and AD8-8 (89.6%) were the top 2 frequently reported symptoms. In Japan, AD8-3 (36.6%) and AD8-4: trouble learning how to use a tool, appliance, or gadget (26.0%) were frequently reported, which were similar to Philippines where AD8-3 (30.6%) and AD8-4 (31.8%) were frequently reported. In Singapore, AD8-3 (64.6%) and AD8-7: difficulty remembering appointments (55.4%) were the top 2 frequently reported symptoms (Table 2).
Prevalence of AD8 Subitems in Alzheimer’s Disease With CDR 0.5.
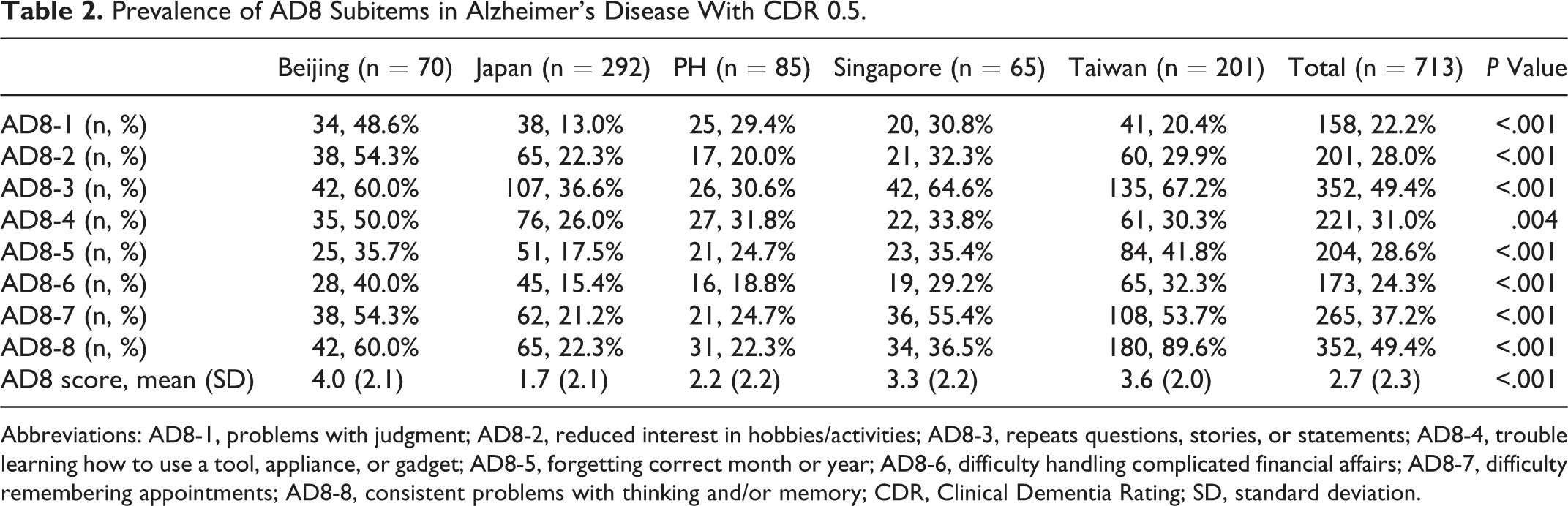
Abbreviations: AD8-1, problems with judgment; AD8-2, reduced interest in hobbies/activities; AD8-3, repeats questions, stories, or statements; AD8-4, trouble learning how to use a tool, appliance, or gadget; AD8-5, forgetting correct month or year; AD8-6, difficulty handling complicated financial affairs; AD8-7, difficulty remembering appointments; AD8-8, consistent problems with thinking and/or memory; CDR, Clinical Dementia Rating; SD, standard deviation.
For the total score of AD8, we have found that Beijing (4.0 [2.1]), Taiwan (3.6 [2.0]), and Singapore (3.3 [2.2]) were higher than the mean score of all recruited participants (2.7 [2.3]). Contrarily, Japan (1.7 [2.1]) and Philippines (2.2 [2.2]) had the comparably lower total AD8 score (Table 2).
In all recruited patients, AD8-4: trouble learning how to use a tool, appliance, or gadget (P = .004) and AD8-6: difficulty handling complicated financial affairs (P = .016) have significant difference in gender in which females were most reported having impairments. The gender-related differences in each AD8 subitem were found only in Japan and Philippines, not in other 3 countries. In Japan, like all recruited patients, the females, compared to males, have more frequently reported impairments in AD8-4 (P = .013) and AD8-6 (P = .029). Similarly, in Philippines, the female patients have more frequently reported impairments in AD8-1 (P = .015), AD8-3 (P = .001), and AD8-8 (P = .038; Table 3).
Gender’s Effect to Reported AD8 Subitems in Alzheimer’s Disease With CDR 0.5.
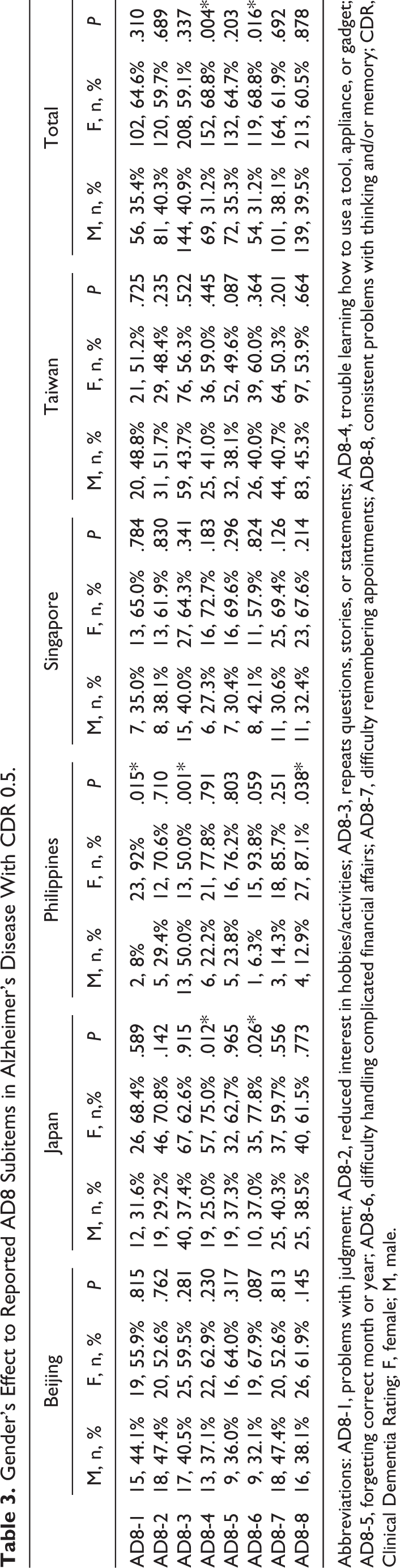
Abbreviations: AD8-1, problems with judgment; AD8-2, reduced interest in hobbies/activities; AD8-3, repeats questions, stories, or statements; AD8-4, trouble learning how to use a tool, appliance, or gadget; AD8-5, forgetting correct month or year; AD8-6, difficulty handling complicated financial affairs; AD8-7, difficulty remembering appointments; AD8-8, consistent problems with thinking and/or memory; CDR, Clinical Dementia Rating; F, female; M, male.
Discussion
Ascertain of Dementia 8 is used extensively in screening dementia in the world with the same cutoff value, 19 -21 but the reported symptoms for dementia, presented as AD8 subitems, could be varied with countries. 26 Also, in Taiwan and Philippines, their MMSE scores were comparably lower in very mild dementia; the lower MMSE could be related to cultural background, age, education, and gender in these 2 countries. 34,35
Interestingly, we have found AD8-3: repeats questions, stories, or statements were one of the top 2 frequently reported symptoms in all Asian countries. The frequently reported symptom, AD8-3, repeats questions, stories, or statements, in part, have reflected the impaired memory still was the cardinal issue for the diagnosis of dementia.
For the AD8 total score, Taiwan, Beijing, and Singapore have the higher score than that of Philippines and Japan. The consistence of having higher AD8 total score was found in Singapore, Beijing, and Taiwan, which could be related to the cultural backgrounds for Chinese population in these 3 countries. The Japanese society is more hierarchical in Asia. Living in such a hierarchical society, a Japanese might not tend to report his feelings to others who were not very familiar to himself. Under such social cultural constraints, Japanese will less report his symptoms as reported in AD8 subitems. 27 These 2 groups of countries in AD8 total score, in part, have reflected some features of cultural background such as Chinese people were tended to report their symptoms compared to other races in Asia.
Besides, compared to Japan, the higher AD8 scores in Taiwan, Beijing, Philippines, and Singapore were owing to fact that the participants recruited were hospital-based samples, not community-based sample, recruited in Japan. People visiting hospital, even they were not with dementia, always have their own purposes or disease so that they would report or complain their symptoms. Such reports or complains would increase the AD8 total score, compared to community participants. 36
In Japan, the gender-related difference of impairments in AD8-4: trouble learning how to use a tool, appliance, or gadget and AD8-6: difficulty handling complicated financial affairs have frequently reported in females because Japan is a hierarchical society and the gender equality is still lagging. 37 The lagging equality in gender would make the function evaluated in AD8-4 and AD8-6 mainly handled by male so that female is more frequently impaired in the ability to maintain the maintenance of appliances and to handle the complicated financial affairs when they are getting older.
The gender-related differences have also been found in Philippines for AD8-1: problems with judgment, AD8-3: repeats questions, stories, or statements, and AD8-8: consistent problems with thinking and/or memory. However, owing to the limited sample size of patients recruited in Philippines and to be examined whether they present these symptoms, the detailed relationships between gender and clinical presentation of early dementia could be clarified further. Recently, the possible mechanisms of gender’s difference to dementia have found in the female brain, 44.2% of genes significantly have been changed in their function during the reproductive transition from premenopause to perimenopause. The changes for these genetic functions would lead to the decreased bioenergetic capacity and increased amyloid dyshomeostasis. In contrast, in the male brain, only 5.4% of genes were altered during this time period. After that period, the subsequent changes in the female brain were relatively small in contrast to those in the male brain, where most changes occurred at a much older age. 38 Such differences might lead to the different clinical presentation of very mild dementia. The detailed mechanism so far is still to be determined.
Our study has strengths that we have reported the symptoms frequently met and reported by informant or caregivers of patients with AD, especially at the very mild stage and for several countries, especially for China, the greatest population in the world. To my knowledge, our study is the first one to report the gender’s effects to early symptoms and the early symptoms of AD in a uniformed manner in several Asian countries, although the various cultural backgrounds would make the clinical presentation of early-stage dementia heterogeneous. Importantly, every diagnosed patient with very mild dementia in our samples has received a serious examination and evaluation including neuroimaging study, so the diagnosis would be more accurate than that in the general population study.
There were limitations to our study. Although the early detection of very mild dementia in all Asian countries was not easy, the sample sizes for each country could be increased. Meanwhile, for these recruited participants who were not by randomized sampling method, the statistical methods with nonparametric or matched participants for comparison in each countries could be applied to interpret and analyze the results. Our participants were from 2 styles, community-based and hospital-based individuals so the total score of AD8 with their reported frequencies of reported subitems could be different, and the interpretation of screening procedures could be difficult. However, for the screening procedures to different sample sources, the standard operating procedures have been established and published. 21 -24 It could be difficult but practicable to interpret the procedure to administrate AD8 to participants. Meanwhile, these early clinical presentations of AD, identification through subitem of AD8, would less likely to be different to where AD was diagnosed, community or hospital, for AD has its original natural course in each country. Patients with diagnosed AD, community based or hospital based, still live at the community with its clinical manifestations and pathological changes. Finally, we did not recruit other variables such as apolipoprotein E genotype, vascular pathology, psychiatric comorbidity, disease duration, or other possible biomarkers into statistical analyses. A future study is necessary to determine whether such parameters would be related to early symptoms of AD.
The significance of the study provides the early symptoms of AD in Asian countries so that primary physicians, bombarded by demands of care by increasing numbers of medical conditions and available treatments, are sufficiently sensitive to symptoms of early dementia.
Footnotes
Acknowledgments
The authors acknowledge and appreciate the contribution from all executive committees of Asian Society Against Dementia.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the Kaohsiung Medical University Hospital, KMUH102-2T05.