
Abstract
Background:
To obtain updated data of patients with Alzheimer’s disease (AD) and their informants in Taiwan with the aim of fostering and supporting collaborative research.
Methods:
In total, 691 patients with the diagnosis of AD were recruited at 6 sites in Taiwan. The Uniform Data Set (UDS; form A) was administrated.
Results:
The mean age of the patients with AD was 79.3 ± 7.7 years and the mean age of informants was 57.5 ± 13.7 years. In all, 69% of the informants lived with patients and 77% of patients lived with spouse, partner, or children; 11% had 1 sibling with dementia, 1.8% had 2 siblings with dementia, and 0.5% had 3 or more siblings with dementia.
Conclusion:
We have reported the updated status of AD in Taiwan through a UDS that will foster future collaboration among countries using UDS. The updated information of patients with AD and their informants will direct the future care of AD in Taiwan.
Background
A rapidly increasing elderly population has become an important medical issue in developed countries. 1,2 More than 35 million people live with dementia, a number that is expected to double every 20 years. 3 The percentage of aged persons (≥ 65 years old) in the total population of Taiwan has risen continuously over the past three decades from 4.1% in 1980 to 10.7% in 2010, 4 the highest rate of aging worldwide. An increasingly aged population will lead to increases in mental decline and dementia as they occur mainly in the elderly population. 5–7
Alzheimer’s disease (AD) is the most frequent cause of dementia and has been estimated to cause approximately 60% to 70% of all cases of dementia in Taiwan. 8,9 However, these studies were conducted decades ago, and there is a lack of updated information on the demographic characteristics of patients with AD and their informants. In addition, there is no uniform data format to record the information and data for patients with AD from different sites in Taiwan. Even though these sites share common components and features, they have developed unique and varied research questions and methods. Therefore, bringing together the different sites in a coordinated effort to use standard assessment methods to gather reliable clinical and neuropsychological data from individuals participating in research studies has been encouraged. In order to reach this goal, we translated the English version of the Uniform Data Set (UDS) of the National Alzheimer's Coordinating Center database 10 into Chinese, containing forms A1 to A5 (demographic and administrative data), B1 to B9 (clinical evaluation data), C1 (neuropsychological data), D1 (diagnostic data), and E1 (imaging and specimen data inventory). The Chinese version of UDS was translated and revised by senior neurologists according to Chinese cultural background and country-specific issues. Back translation of the Chinese version of UDS was made in order to make it as effective as the English version.
We then administered form A at 6 sites in Taiwan from 2010 to 2012 to obtain updated data of patients with AD and their informants, with the aim of fostering and supporting collaborative research.
Methods
The A components, from A1 to A5, were selected from the UDS and conducted at 6 sites in Taiwan. The A1 component was patient demographics including sex, race, ethnicity, and marital status. The A2 component was informant demographics including relationships and visits between the informant and patient. The A3 component was family history related to dementia, focusing on dementing illnesses experienced by the participant’s first-degree relatives. The definition of these dementing illnesses was progressive loss of memory and cognition and was often described as senility, dementia, AD, hardening of the arteries, or other causes that compromised the patient’s social or occupational functioning and from which they did not recover. Components A4 and A5 were medications and health history, respectively.
Patients
All patients were recruited between October 1, 2010, and January 30, 2012, from 6 sites, 2 of which were medical centers in the north, 1 area hospital, and 1 medical center in the middle, and 2 medical centers in the south of Taiwan. All patients received a comprehensive medical evaluation, including clinical history, physical and neurological examinations, computerized tomography of the brain, and blood chemistry examinations to exclude other possible causes of the current cognitive status. The diagnosis of AD was based on the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer's Disease and Related Disorders Association criteria 11 referring to a series of comprehensive neuropsychological tests, including the Mini-Mental State Examination (MMSE), 12 Clinical Dementia Rating (CDR) scale, and sum of CDR boxes. 13 Patients with other conditions possibly contributing to the diagnosis of AD were excluded.
Evaluation
All procedures were approved by each institutional review board of the 6 sites, and written informed consent was obtained from all participants or their legal representative. For each recruited patient, a series of neuropsychological assessments including the MMSE and CDR and clinical history and information of the patients and informants were recorded by a senior neuropsychologist and an experienced physician based on information from a knowledgeable collateral source (usually a spouse or adult child).
Statistical Analysis
Data analysis was performed using SPSS (version 12.0.1 for Windows, SPSS Inc, Chicago, Illinois). All statistical tests were 2-tailed, and an α value of .05 was taken to indicate significance. Descriptive statistical analyses were conducted for all continuous variables with mean ± standard deviation.
Results
In total, 691 patients with AD (64.5% female) were recruited into the statistical analysis, including 186 (27%) from the north, 175 (25%) from the middle, and 330 (48%) from the south of Taiwan. The mean age of the patients was 79.3 ± 7.7 years, and the mean age of the informants was 57.5 ± 13.7 years. Importantly, 69.3% of the informants lived with the patients (Table 1). Most of the patients were right-handed (94.6%) and spoke the first language of Taiwanese (63.9%) in contrast to Mandarin (32.2%; Table 2).
Demographic Characteristics of Patients and Informants in Taiwan.
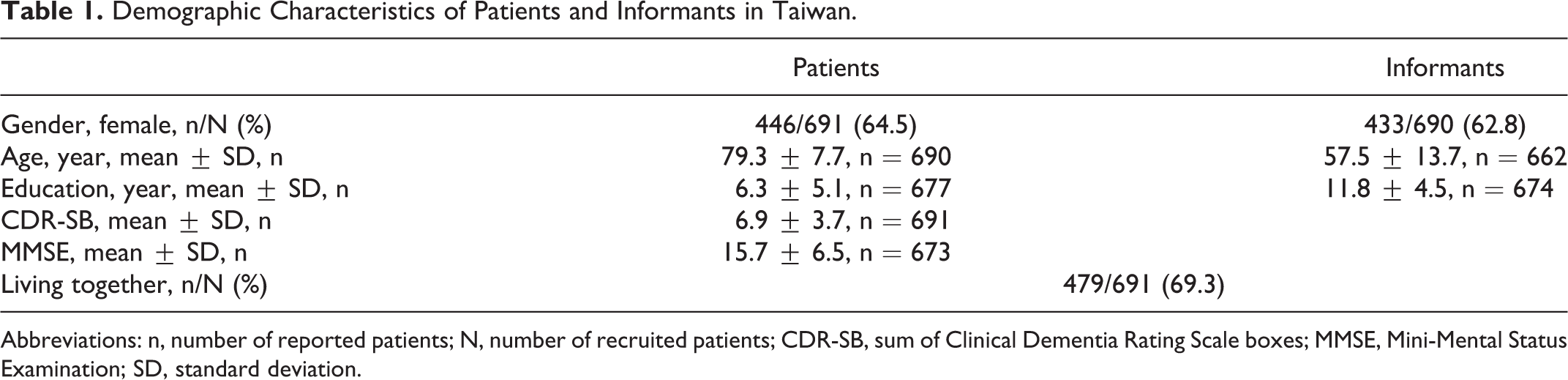
Abbreviations: n, number of reported patients; N, number of recruited patients; CDR-SB, sum of Clinical Dementia Rating Scale boxes; MMSE, Mini-Mental Status Examination; SD, standard deviation.
Handedness, Language, and Current Marital Status of the Patients.
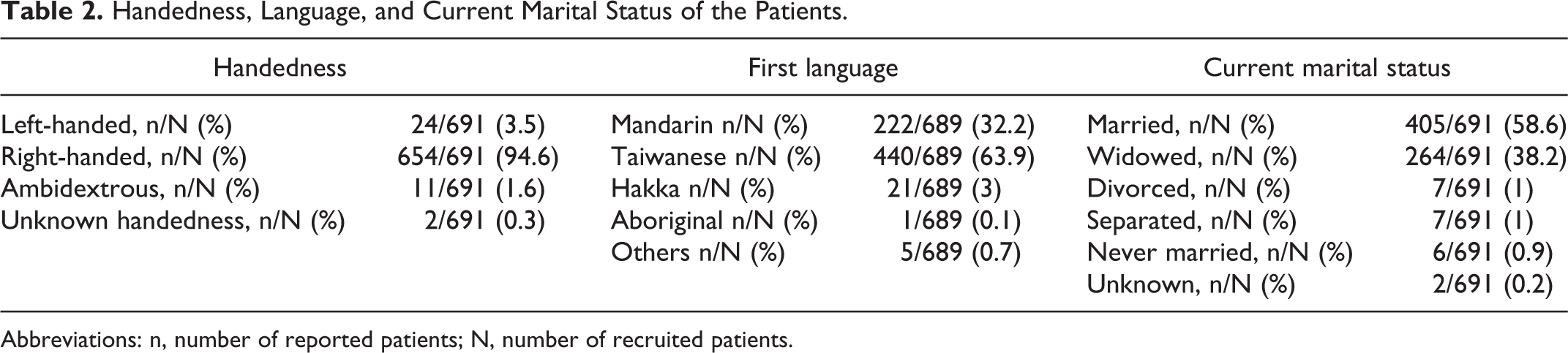
Abbreviations: n, number of reported patients; N, number of recruited patients.
Most of the recruited patients lived independently (32.5%) or with some assistance for doing complex activities (31.6%; Table 3). With regard to the living situation, 76.9% of the patients lived with a spouse, partner, or children, and 11% lived with friends or other relatives (Table 3). With regard to marital status, 58.6% of the patients were married, 1% were divorced, 0.9% had never married, and 1% were separated (Table 2).
Level of Independence and Living Situation of Patients.
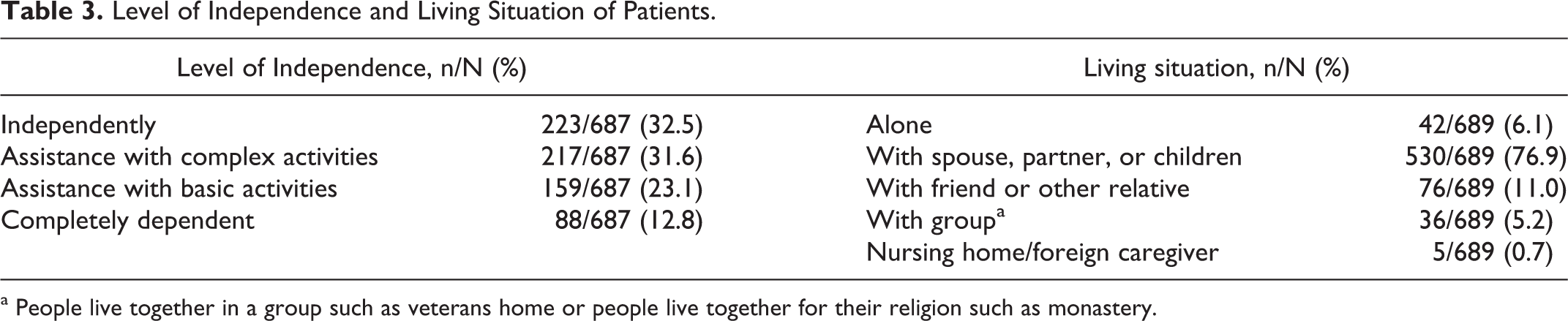
a People live together in a group such as veterans home or people live together for their religion such as monastery.
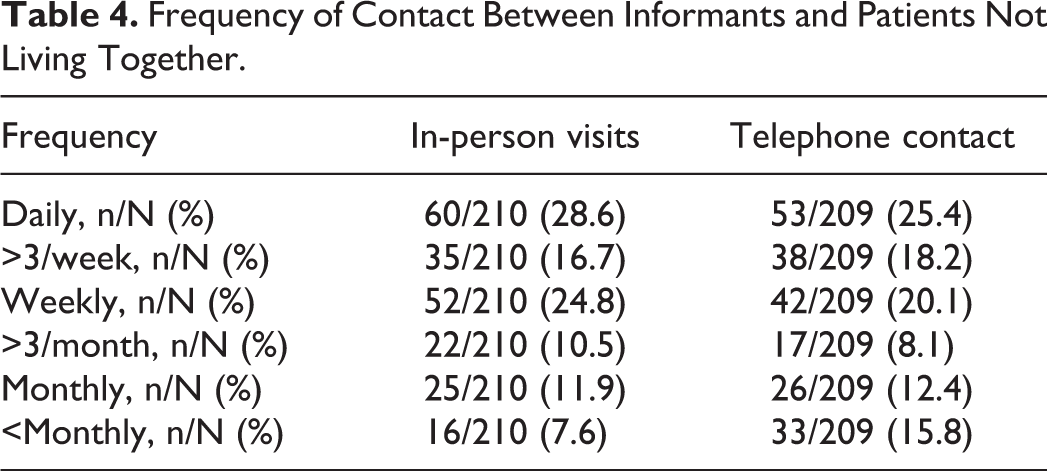
For the informants who did not live with the patients with AD, the frequencies of making in-person visits once daily, once weekly, and once monthly were 28.6%, 24.8%, and 11.9%, respectively, and of telephone contacts were 25.4%, 20.1%, and 12.4%, respectively. Interestingly, the frequency of more than 3 in-person visits per week was 16.7%, which was less than the frequency of daily and weekly visits. Similarly, the frequency of more than 3 telephone calls per week (18.2%) was also between that of daily and weekly telephone contact (Table 4).
Frequency of Contact Between Informants and Patients Not Living Together.
With regard to a family history of dementia of these recruited patients, 6.7% had a reported history of dementia in their mothers, in contrast to 2.7% in their fathers, and 0.3% in their children (Table 5). Among all patients, 10.8% had 1 sibling with dementia, 1.8% had 2 siblings with dementia, and 0.5% had 3 or more siblings with dementia (Table 5). The number of siblings of patients with dementia ranged from 0 to more than 12 (Table 6), and 6 siblings had the highest percentage (13.9%) The majority of patients had 3 (20.3%) or 4 (25.7%) children (Table 6).
Family History and Number of Dementia for Patients in Taiwan.
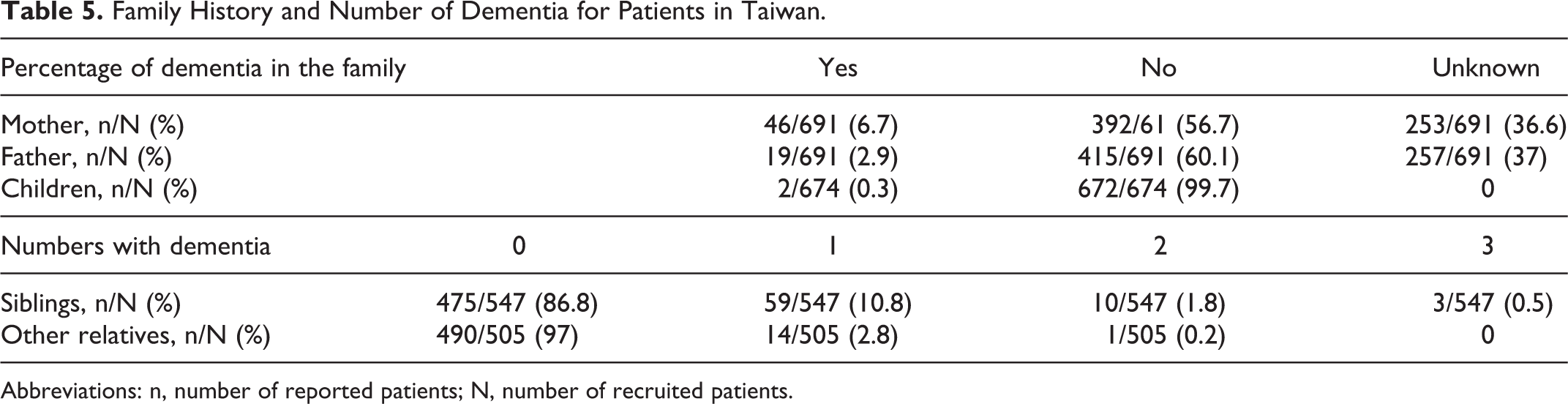
Abbreviations: n, number of reported patients; N, number of recruited patients.
Number of Siblings and Children of the Patients With Dementia.
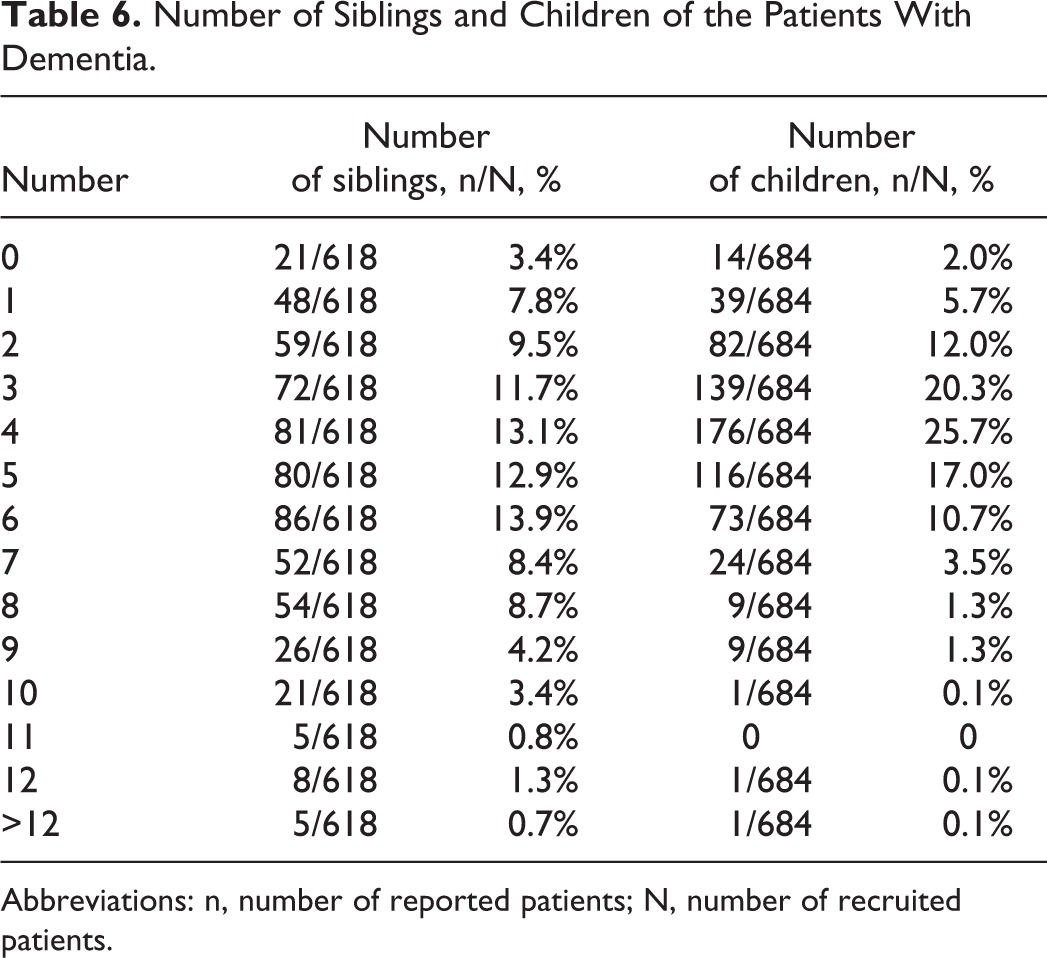
Abbreviations: n, number of reported patients; N, number of recruited patients.
Discussion
We recruited the patients with AD through a UDS to establish a platform for further studies and reported the updated status of AD in Taiwan. Only a few studies have reported on the clinical characteristics of patients with AD and their informants, and to the best of our knowledge, no other study has addressed the family history of patients with AD in Taiwan using the UDS.
With regard to the living situation, only 76.9% of the patients were living with a spouse, partner, or their children, in contrast to a study by Lin et al in Taiwan, in which 95% of patients with dementia were cared for by their family. 14 However, the authors did not further stratify the family members and did not clarify the difference between informants and caregivers, which is important because caregivers and informants are not always the same person for an patient with AD. Our findings are similar to a report from the United States, and despite the decline in function associated with AD, many studies have shown that the majority of older people prefer to live in their homes for as long as possible. 15,16 Our findings also revealed that 6.1% of the patients with AD lived alone, and the significance of living alone is that people with dementia who live alone are placed in nursing homes earlier, on average, than otherwise similar people with dementia who do not live alone 17,18 because of the potentially increased risk of malnutrition, illness, and fall-related and other injuries.
An important finding is that 69.3% of the informants lived with the patients and that 28.6% of the informants who did not live with the patients made daily visits, with 16.7% making more than 3 visits per week. This is important with regard to the clinical diagnosis and evaluation of dementia because the diagnosis of dementia requires an informant to provide accurate information about the patient including changes in condition. The frequencies of more than 3 in-person visits and telephone calls per week were less than those of the daily and weekly values. This also reflects the condition of current care of patients with AD in Taiwan, in that the relationship between the patient and informant may be “2-sided”, that is, either daily or weekly.
With regard to the first language spoken by the patients, most (63.9%) spoke Taiwanese because a most (48%) of the patients were recruited from southern Taiwan where Taiwanese is the language spoken most commonly, not Mandarin. Few studies have reported on the handedness of patients with AD, and in this study, 94.6% of the patients with AD were found to be right-handed. This is a little different from a study in which 90% of the general population were reported to be right-handed, 19 however we do not have enough data to examine possible differences in the handedness of patients with AD, and further studies are needed to elucidate this issue.
The mean age of our recruited patients (79.3 ± 7.7 years) was higher than that reported in a study from the United States (76.7 ± 9.2 years). 20 However, this difference may be related to the bias of sample selection and because the study from the United States was published 7 years ago.
The marital status of AD in Taiwan was less reported than that in the United States. 21 However, this might highlight the existing problem. Recent studies 21,22 have indicated the burden of spouse caregivers should be estimated and released because of the demented spouse, and the marriage condition will affect the survival of patients with dementia. 23 Patients with AD are generally institutionalized more rapidly if the caregiver is not a spouse. 24
As with other reports, 20,25–27 female gender was a risk factor for AD, and most of our recruited patients were female. The higher percentage of female patients with AD is mainly because of the higher percentage of the patients’ mothers having dementia (6.7%) than their fathers (2.7%). The low percentage of dementia in the patients’ children (0.3%) may be because their children were not old enough to have AD.
There are some limitations to this study. We recruited the patients with AD from several referral and medical centers, which may not be generalizable to all patients with AD in Taiwan. There may be selection bias, although we recruited the patients from north, middle, and south Taiwan to minimize this. A more extensive study recruiting more patients with AD through a uniform data is warranted.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.