
Abstract
Background
To update the characteristics of patients with Alzheimer’s disease (AD) and their informants in Taiwan and compare them from 12 years ago.
Methods
1218 patients with AD and their informants were recruited from six hospitals in Taiwan. The uniform data set version 3.0 (UDS3, form A1-A3) were administered.
Results
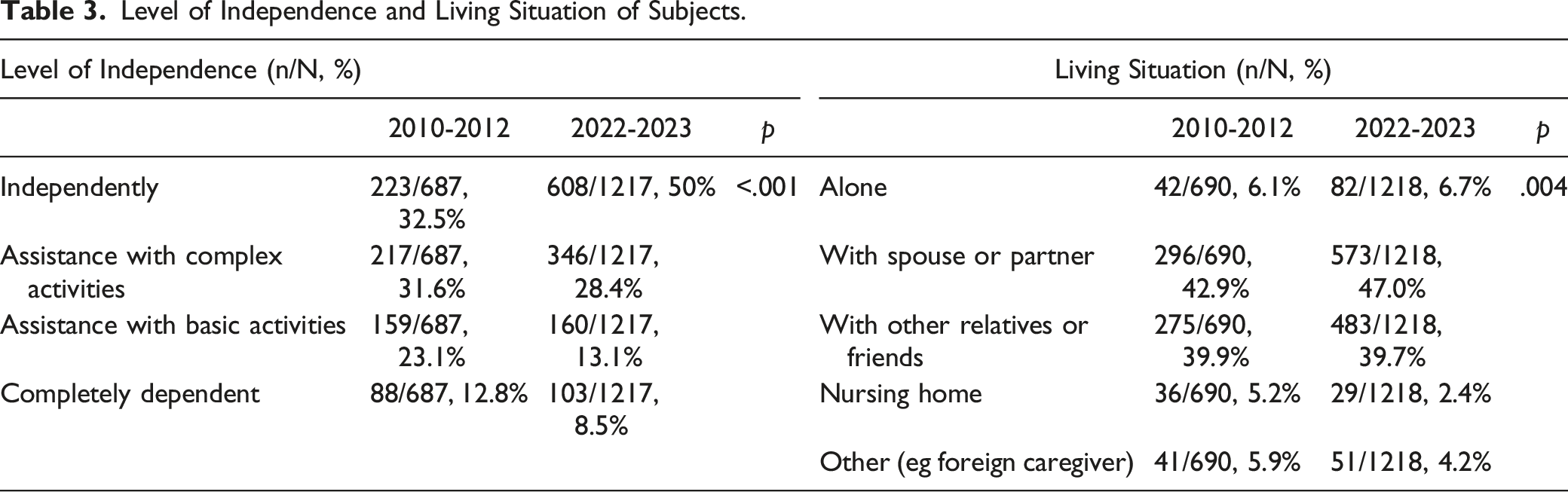
Compared with the first registration from 2010-2012 (n = 691), the mean clinical dementia rating sum of boxes score was significantly lower, more patients living independently, and more informants not living together with the patients. A total of 11.2%, 4.1%, 12.8%, and 0.5% of the patients had a reported history of cognitive impairment in their mothers, fathers, siblings, and children, respectively.
Conclusion
Compared with the data from 2010, patients have been diagnosed at a milder disease stage, and their informants used telephone contact more frequently instead of living with the patients. Family histories of cognitive impairment in patients with AD remain frequent.
Keywords
Introduction
The number of individuals with dementia is increased worldwide. According to the World Alzheimer Report 2015, 46.8 million people were living with dementia in 2015 and this number is expected to double every 20 years. 1 Taiwan has become an “aged society” since 2018 and is predicted to become a super-aged society by 2025. The number of patients with dementia has increased dramatically with the rapid increase in the elderly population. The age-stratified prevalence rate approximately doubles every 5 years after the age of 50 years, and the prevalence of dementia was estimated to be 7.54% in the population aged >65 years in Taiwan.2,3
Alzheimer’s disease (AD) accounts for approximately 60% of all dementia in Taiwan. 4 Using the Uniform Data Set (UDS) of the National Alzheimer's Coordinating Center database, 5 the demographic characteristics of patients with AD and their informants were reported from 2010 to 2012 in Taiwan. 6 Family histories were also recorded, with 6.7%, 2.7%, and 13.1% of mothers, fathers, and siblings, respectively, having a reported history of dementia. Collaborative research across multiple sites in different countries is accessible in a uniform data format. The clinical picture for patients and informants, as well as family history, is very different among Asian countries.7,8
In 2015, the US Alzheimer’s Disease Centers (ADC) implemented Version 3 of the Uniform Dataset (UDS3). 9 The recoding of demographic data in UDS3 was comparable to that in the first version. However, a more detailed family history was recorded, such as the etiological diagnosis and evaluation method of family members reported to have cognitive impairment. Renewing the most recent characteristics of AD and their informants provides clues for understanding the status of the clinical picture of AD in Taiwan. We then administered the second registration from 2022 to 2023 to obtain updated data on patients with AD and their informants and compared them with the first evaluation.
Methods
Measurement
The present registration selected A1 to A3 components from UDS version 3.0 and enrolled six hospitals in Taiwan (one from the north, two from the middle, two from the south, and one from the east of Taiwan). The A1 component included subject demographics, including sex, education, living situation, and marital status. The A2 component was informant demographics, including the relationships and visits between the informant and the subject. There were no major changes in the A1 and A2 components compared with UDS version 1.0. The A3 component represents a family history of cognitive dysfunction. The cognitive status of the participants’ parents, children, and siblings, including mild cognitive impairment (MCI) (single or multiple, amnesic or non-amnesic domain) or dementia (specific etiology coded if known), was recorded. UDS 3.0 added family history of AD or frontotemporal dementia (FTD) mutations and recorded associated neuropsychiatric diagnoses (such as amyotrophic lateral sclerosis (ALS), parkinsonism, or stroke) in the A3 component. 9
Participants
All subjects were recruited between March 1, 2022 and January 30, 2023, from six sites: a regional hospital in the north, one regional hospital and one medical center in the middle, one regional hospital and one medical center in the south, and one regional hospital in the east of Taiwan. All subjects underwent a comprehensive medical evaluation, including clinical history, physical and neurological examinations, neuropsychological tests including the Cognitive Ability Screening Instrument (CASI) 10 and Clinical Dementia Rating (CDR) scale, 11 brain imaging, and blood chemistry examinations, to exclude other possible causes of the current cognitive status. The Mini-Mental State Examination (MMSE) score used in the present study was converted from the CASI, which has been reported to have a moderate to excellent equivalence with the original MMSE score. 12 Diagnosis of AD was based on the NINCDS-ADRDA criteria. 13 Patients with other conditions that may have contributed to the diagnosis of dementia were excluded.
All procedures were approved by the institutional review boards (IRB) of the six sites, and written informed consent was obtained from all participants or their legal representatives. For each recruited subject, a series of neuropsychological assessments, including the CASI and CDR, were evaluated by neuropsychologists, and the clinical history and information of the subjects and informants were recorded by trained study assistants.
Statistical Analysis
All data collected in the present study were compared to the first AD registration in Taiwan. 6 All statistical analyses were performed using R Statistical Software (version 4.1.0; R Foundation for Statistical Computing, Vienna, Austria). 14 All statistical tests were two-tailed and an alpha value of .05 was taken to indicate significance. Descriptive statistical analyses were conducted for all continuous variables with mean ± standard deviation. Differences between categorical data were calculated using Pearson’s chi-square test or Fisher’s exact test. Numerical data were analyzed using Student’s t-test or the Kruskal–Wallis rank-sum test.
Results
Demographic Characteristics of Subjects and Informants in Taiwan.
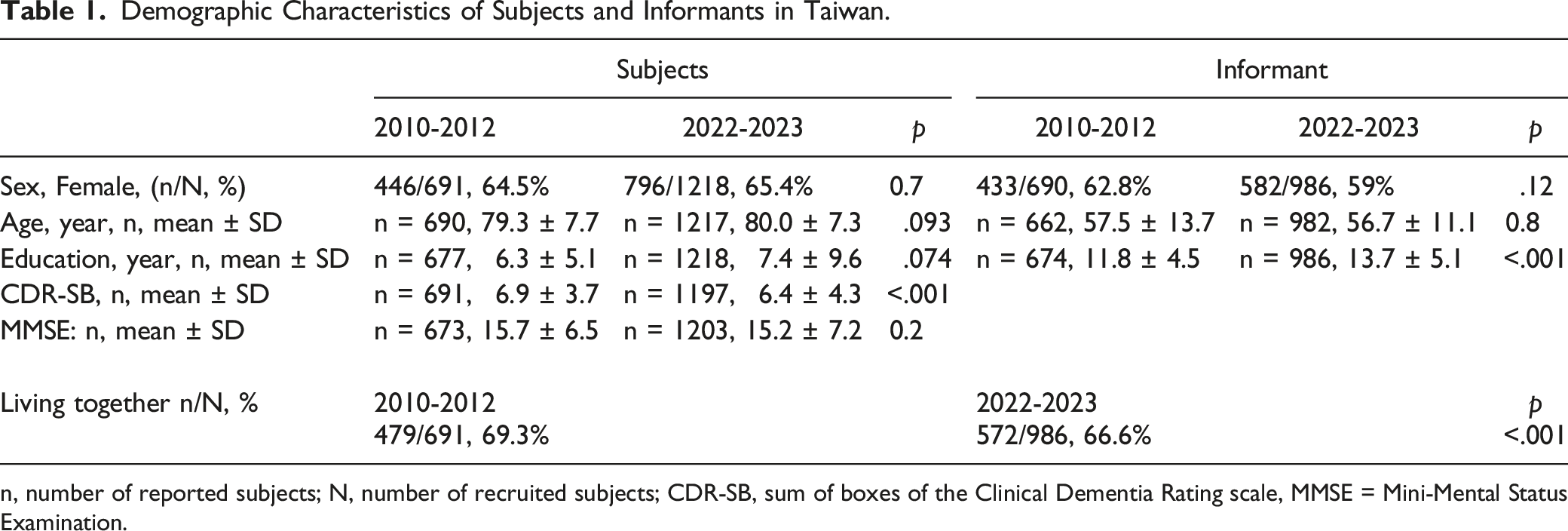
n, number of reported subjects; N, number of recruited subjects; CDR-SB, sum of boxes of the Clinical Dementia Rating scale, MMSE = Mini-Mental Status Examination.
Handedness, Language and Current Marital Status of the Subjects.

n, number of reported subjects; N, number of recruited subjects.
Level of Independence and Living Situation of Subjects.
Frequency of Contact Between Informants and Subjects not Living Together.

Family History and Number of Dementia or Cognitive Impairment for Subjects in Taiwan.

n, number of reported subjects; N, number of recruited subjects.
Family History and Number of Other Neuropsychiatric Disorders for Subjects in Taiwan. (Only 2022-2023 Data).

n, number of reported subjects; N, number of recruited subjects.
Discussion
This study reports the current status of AD in Taiwan. Compared to a decade ago, AD subjects had milder severity and more of them lived independently, while more informants did not live with the subjects and used more telephone contact.
In response to the rapid growth in the dementia population, the Ministry of Health and Welfare in Taiwan has implemented the Dementia Care Policy since 2013. To further help families with dementia, Taiwan’s government established the Long-Term Care Act 2.0 since 2017, which includes people with dementia over the age of 50. 15 As part of this reform, the government implemented innovative dementia care programs and settled “Dementia integrated care centers,” which are hospitals or sites that diagnose, provide patient and caregiver education, introduce social resources, promote health literacy of dementia, and educate healthcare providers. As of September 2021, there are 103 dementia-integrated care centers covering all counties in Taiwan. Proper education of clinicians about the diagnosis of cognitive dysfunction and increased health awareness of dementia in the general population both facilitated the earlier identification of subjects with probable or possible AD. The milder severity in the present registration may reflect that people in Taiwan seek medical advice earlier in response to the government’s policy. The frequency of living independently was higher, indicating more patients were diagnosed at the stage of mild cognitive impairment.
Regarding living situation, 86.7% of the participants were living with a spouse, partner, or other relatives (most of them were children). Less AD patients living in nursing homes or with foreign caregivers when compared with the first registration, which may also reflect that the patients were diagnosed earlier. The present study was comparable to the World Alzheimer Report; most patients with dementia were still living at home, and 94% of people living with dementia in low- and middle-income countries were cared for at home. 1 In addition, 6.7% of patients with AD lived alone, higher than the 6.1% in 2010. People with dementia who live alone are placed into nursing homes earlier because of the potentially increased risk of malnutrition, illness, and fall-related injuries.16,17
Of the informants, 66.6% lived with the participants, significantly less than 69.3% in the previous survey. The frequency of in-person and telephone contact increased. Family organizations have changed over the past 50 years in East Asia, with a sharp decline in fertility, later marriages, and non-co-residence with parents. 18 A couple's economic resources facilitated the breaking away from patrilocal co-residence in Taiwan. 19
Taiwanese was the most common first language spoken by the subjects, significantly more than at the first registration, because more of the subjects were recruited from middle to southern Taiwan (88% vs 73%), where the most common spoken language is Taiwanese, not Mandarin.
When compared to the UDS3 demographic data reported by the US ADC in 2018, the mean age of our recruited subjects was higher, and they had lower education levels. 9 There were no family members with known AD or FTD mutations in the present study, compared with .6 and 1.1% in the USA, respectively. However, the USA report included dementia with other etiologies, and 45.7% of the participants had a global CDR score of 0, which made it difficult to compare between studies. Considering only AD patients reported by the ADC in 2005, the participants’ age and sex were similar to those in the present report. 20
The percentages of patient’s mothers, fathers, and children with dementia were 11.2%, 4.1%, and .5%, respectively. The Rotterdam Study found that 25.6% of patients with AD had first-degree relatives with a history of dementia. 21 The higher percentage in the Rotterdam cohort may be because each first-degree relative was evaluated by the study physician to confirm a diagnosis of dementia. Female sex is a risk factor for AD, and most subjects recruited in UDS studies were female.9,20 The higher percentage of female patients with AD also contributed to a higher percentage of the patients’ mothers having dementia (11.2%) than their fathers (4.1%). Similar trends have been observed in other Asian countries. 7 The reported maternal history of cognitive dysfunction was significantly higher than that reported during the first registration in Taiwan. The possible explanations were the higher education level of informants to provide a detailed family history and included the diagnosis of both MCI and dementia in the UDS3. The present study may also indicate that the UDS3 provides a more accurate recording of family history through etiological coding.
To the best of our knowledge, no family history of other neurological or psychiatric disorders for patients with AD was reported in Taiwan. Psychiatric history has been suggested to be an integral part of family history, especially in individuals with FTD. 22 Approximately 40%–50% of patients diagnosed with FTD have a family history of neurological or psychiatric disorders. 23 Devi et al reported that the incidence of any psychiatric disorder in family members with late-onset AD was 15%. 24 Further research is needed to determine the family history of these disorders in individuals with dementia.
The strength of this study is its multicenter registration covering all regions of Taiwan, providing an updated clinical picture of patients with AD and their informants compared with 12 years ago. However, this study has some limitations. First, the recruited AD subjects may not be generalizable to all patients with AD in Taiwan owing to selection bias. Second, all family histories were reported by informants or patients, and a reporting bias may exist. It is difficult to determine whether the family histories of dementia are truly indicative of a genetic risk factor for AD. Third, the present study only included patients with clinical diagnosis of AD, therefore, whether the findings are specific to AD or they are also seen in other types of dementia were uncertain. Approximately 30% of the parental history of dementia is unknown, and more than 80% of the etiological diagnoses are uncertain.
Conclusion
This study updated the demographic data of patients with AD and their informants in Taiwan. Compared to 12 years ago, AD patients were diagnosed at a milder disease stage, and their informants used telephone contact more frequently instead of living with the patients. Family histories of dementia in patients with AD remain frequent. The percentages of patients’ mothers, fathers, siblings, and children who reported having dementia were 11.2%, 4.1%, 12.8%, and .5%, respectively. UDS3.0 help establish a platform for further studies and supports collaborative research.
Footnotes
Acknowledgments
The authors gratefully acknowledge all the sites and their primary investigators for participating in the present and first registrations: Professor Jung-Lung Hsu at New Taipei Municipal Tu Cheng Hospital, Professor Pai-Yi Chiu at Lin Shin Hospital, Professor Yu-Te Lin at Kaohsiung Veterans General Hospital, Professor Chaur-Jong Hu at Shuang Ho Hospital, and Jong-Ling Fuh at Taipei Veterans General Hospital.
Author Contributions
YHY, KMJ, LCH, KNH, SCH, SHY and WFW designed the study. YHY and KMJ analyzed the data. KMJ and WFW wrote the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Health Research Institutes (NHRI-11A1-CG-CO-06-2225-1,NHRI-12A1-CG-CO-06-2225-1) and Kaohsiung Medical University Research Center (KMU-TC111B02).
Data Availability Statement
According to the nature of the research, supporting data is not available due to ethical restrictions.