
Abstract
This study attempted to better understand factors associated with relationship conflict between daughters and their parents with dementia. We examined data from 77 daughters self-identified as primary caregivers of a parent with dementia to test the hypothesis that daughters’ belief that a parent with dementia can control their symptoms is associated with more conflict, defined as high expressed emotion (EE). Participants completed self-report questionnaires assessing beliefs about parents’ ability to control symptoms, stress, relationship conflict, parent agitation, and cognitive status. Results indicated that greater intensity of daughters’ belief that their parent can control dementia-related symptoms was associated with more relationship conflict or “high EE” (β = 0.57, P < .001). Daughters’ beliefs about parental behavior may contribute to caregiver stress and exacerbate negative behaviors exhibited by individuals with dementia. Educating caregivers about parental behaviors and examining factors underlying caregiver interpretations of these behaviors hold promise for reducing caregiver stress.
Introduction
Daughters represent 37.5% of family caregivers of individuals with dementia. 1 Although caring for an individual with dementia is extraordinarily challenging and is often associated with adverse physical and mental health consequences for caregivers, this may be particularly true for daughters. 2,3 A growing body of evidence suggests that the experience of caregiving varies by kinship and daughters experience particularly negative effects. Specifically, the psychological experience of distress among daughters is impacted by potentially mutable psychological factors above and beyond concrete variables such as frequency of leisure activities or frequency of problem behaviors. 4,5 For example, caregiver guilt has been found to significantly moderate the relationship between frequency of leisure activity and depression among daughters but not so in sons, wives, or husbands. 4 Additionally, in contrast to wives, daughters do not show the expected relationship between stressors, stress, and depression. 5
“Expressed emotion” (EE), a construct originally developed in the context of family caregiving for individuals with severe mental illness, reflects the family’s general attitude toward a patient and has become one of the most studied frameworks for understanding the nature and quality of caregiving in the context of chronic illness. 6 Research on EE has increasingly focused on negative dimensions of family attitude such as criticism, intrusiveness, negative attitudes, and intolerance toward the care recipient, as these have been shown to predict both (1) behavioral patterns between caregiver and care recipient and (2) outcomes for care recipients and caregivers. For example, “high EE,” referring to greater levels of negative attitudes toward the patient, has been correlated with escalating negative behavior in interpersonal interactions and less reciprocal positivity between caregiver and care recipient. 7 -9 Furthermore, high EE is a robust predictor of relapse and escalating symptomatology in a variety of disorders. 6 For caregivers of individuals with dementia, high EE has been related to greater caregiver distress and greater care recipient aggression, anger, and tendency to wander. 2,10 High EE daughters experience greater strain and distress than “low EE” daughters over and above the impact of their parents’ cognitive status. 10 Thus, better understanding daughters’ EE may provide insight into the dynamics influencing strain and distress in a caregiving relationship where these negative outcomes may be particularly mutable through psychological intervention.
One potential factor that influences EE is the kind of attributions daughters make for their parents’ problematic behaviors, specifically whether those behaviors are believed to be within versus outside their parents’ control. 2,10,11 In nondementia family caregiving contexts, high EE tends to be associated beliefs that a care recipient’s problematic behaviors are within that person’s control (ie, “causal attributions”). 12,13 Two studies have also found an association between family caregiver causal attributions and high EE in the context of dementia. 2,14 However, these studies did not specifically examine the experience of daughters. Additionally, 1 study did not control for baseline characteristics of the care recipient making it difficult to assess if characteristics, such as greater agitation or cognitive impairment, accounted for the association between causal attributions and high EE (ie, caregivers of less impaired care recipients may report fewer causal attributions as well as low EE because of the lower frequency of symptoms). Moreover, investigators obtained both EE and attribution data by coding the same semistructured interview with caregivers, which may have resulted in confounding as the same moment when a caregiver blames a parent for their behavior is likely to also be coded as a moment when the caregiver displays high EE (eg, is critical or hostile). 2,15 The current study attempts to address these limitations to clarify the relationship between EE and causal attributions among daughters caring for parents with dementia. We hypothesized that a daughter who believes that her parent’s problematic behaviors are within that parent’s control (ie, make causal attributions) was more likely to experience high EE.
Methods
Procedure/Sample
A subset of data from the “Families and Caregiving Study” was used for the present research. 16 The Families and Caregiving Study was conducted at the University of North Carolina–Chapel Hill (UNC-CH) with the goal of better understanding factors that impact the relationship dynamics between individuals with dementia and their family caregivers. Participants in the Families and Caregiving Study were 100 self-identified primary caregivers for family members with dementia. They were recruited from nursing facilities, senior centers, and memory disorders clinics in the North Carolina, Research Triangle area, and from employees and students at the UNC-CH. Former participants in the Alzheimer’s Association’s Dementia Care Project were also invited to participate in the study. 17 The Alzheimer’s Association’s Dementia Care Project was a study of older adults with dementia residing in assisted living facilities and their caregivers. The participants of that study, conducted by the Cecil B. Sheps Center for Health Services Research at UNC-CH, were invited to participate in the present study. Of the 193 caregivers who participated in the Alzheimer’s Association’s Dementia Care Project, study staff were able to obtain updated contact information for 35 caregivers; of whom, 4 care recipients had died, 7 were unable to be contacted, 4 refused to participate, and 20 (of our total 100 participants) agreed to participate in the Families and Caregiving Study whose data are presented here.
Participants in the Families and Caregiving Study were interviewed over the telephone and completed a series of questionnaires designed to assess aspects of the caregivers’ relationship dynamics, stress, and attitudes toward the person with dementia. For the current analyses, we restricted the sample to daughters caring for a parent with dementia (N = 77), to specifically examine the dynamics within those relationships.
Measures
We surveyed participants using the 16-item short form of the Cohen-Mansfield Agitation Inventory (CMAI) to measure the frequency of behaviors such as wandering, agitation, physical aggression, screaming, and sexual disinhibition. 18 The CMAI is one of the most commonly used instruments to assess the level of agitation in patients with dementia. We used the Minimum Data Set—Cognition Scale (MDS-COGS), an 8-item measure completed by the family caregiver, to assess memory, orientation, and decision-making. 19 It has been found to be a valid measure of cognitive status, demonstrating convergent validity with the Mini Mental Status Exam (MMSE) (Spearman correlation coefficient = −0.88, P < .001) and good to excellent sensitivity and specificity for correctly discriminating cognitively impaired from cognitively intact participants as defined by the MMSE. 19 To measure EE, we used the caregiver version of the Level of Expressed Emotion (LEE) scale. 20 The LEE consists of 4 subscales that measure a caregiver’s tendency to (1) be intrusive, (2) respond in ways that exacerbate patient distress (emotional reactivity), (3) hold negative attitudes toward the illness (eg, doubts about the nature of the illness), and (4) have low tolerance for disturbed behaviors. The LEE has been shown to be reliable and internally consistent and correlates with ratings on the Camberwell Family Interview, the gold standard interview measure of EE. 20,21 We modified the Control of Symptoms Scale (CSS) from a measure developed for individuals with anxiety disorders and adapted it for relatives of individuals with dementia. 22 The CSS measures the degree to which daughters believe their parent can control 23 behaviors that are common for dementia. In the current study, the CSS was modified for use with relatives of individuals with dementia by substituting characteristic symptoms of dementia identified by the problem checklist for the anxiety disorder items originally measured. 23 The problem checklist is a list of 23 observed behaviors that are significantly more common in older adults with dementia than those without dementia. Examples of items on the checklist are always asking questions, temper outbursts, wandering, and physical aggression. 22 The scale was internally consistent (α = 0.90), normally distributed, and significantly associated with caregiver and patient distress and patient psychopathology in both current sample and among caregivers of individuals with anxiety disorders. 22 Additional survey items included the Gilleard Strain Scale (GSS), a 13-item self-report questionnaire of caregiver strain measuring caregiver report of experiences including embarrassment, frustration, danger, concern about finances, and anxiety, and the Marlowe-Crowne Social Desirability Scale, a 10-item measure of response bias toward answering in ways that would be viewed positively toward others. 23,24 In previous studies, high scores on the GSS have been associated with higher levels of EE. 2 Finally, the Marlowe-Crowne Social Desirability Scale has been shown to have high internal consistency (α = 0.88), test–retest correlation of 0.89, and convergent and divergent validity. 25
Analytical Approach
We used Stata version 12.1 for all data analyses. Following the examination of descriptive statistics for each variable to assess for appropriate range and distribution, we conducted a series of Ordinary Least Squares (OLS) linear regression analyses to examine the hypothesis that daughters’ perceptions of controllability (meaning that their parent with dementia could control their behaviors) are more strongly associated with EE than other caregiver and care recipient characteristics. Specifically, we ran a total of 5 regression analyses that examined the relationship between daughters’ perceptions of controllability and EE. Our dependent variable in each regression consisted of (1) overall EE and (2) 1 of the 4 LEE subscales to evaluate whether the relationship to controllability varied across aspects of EE. In all analyses, we standardized all variables, controlled for cognitive status and agitation for the person with dementia as well as daughter’s strain, education, degree of involvement, length of time as a caregiver, and social desirability. In prior studies, caregiver assessment of burden and stress was correlated with EE such that controlling for daughter’s strain allowed us to examine the relationship between caregiver attributions and EE above and beyond the effect of daughters’ stress. 10,26 Caregiver education, 26,27 -30 length of time as caregiver and/or amount of time devoted to caregiving, 26 -28 and location/living arrangements 29,31 are also common covariates in studies of EE. We also assessed social desirability to control for daughters’ reluctance to report behavior or attitudes that they anticipated might be viewed negatively. All variables were entered simultaneously in the regression model. We examined semipartial correlations of predictor variables to determine the variability in EE uniquely accounted for by controllability and each of the other predictors.
Results
Seventy-seven daughters who self-identified as the primary caregiver of a parent with dementia completed questionnaires about their experience as caregivers. The majority of the sample (71%) was students or employees of UNC-CH recruited via an e-mail advertisement about the study. The remainder (20%) were former participants in the Alzheimer’s Association’s Dementia Care Study, 17 referrals from previous participants (7%), and individuals who responded to flyers placed in nursing facilities, senior centers, and memory disorders clinics (2%). The majority of daughters were Caucasian (91%), highly educated (70% with a college degree or graduate degree), and had a household income greater than US$50 000 (88%). The majority (63%) of care recipients lived in an institutional setting (ie, assisted living, nursing facility, or special care unit), 26% were living alone in the community, and 11% were living with their daughters. The mean MDS-COGS score, based on daughters’ report, indicated mild cognitive impairment (mean MDS-COGS score: 15.71; standard deviation [SD] = 4.43; range = 7-23). The mean CMAI score (mean 27.42; SD = 7.61; range = 16-80) was indicative of mild parent behavioral problems. Also, daughters’ overall ratings of their perceptions of controllability were relatively low (mean 1.57 on a 5-point scale; SD = 0.69; see Table 1 for descriptive statistics of all variables).
Descriptive Statistics for All Variables.
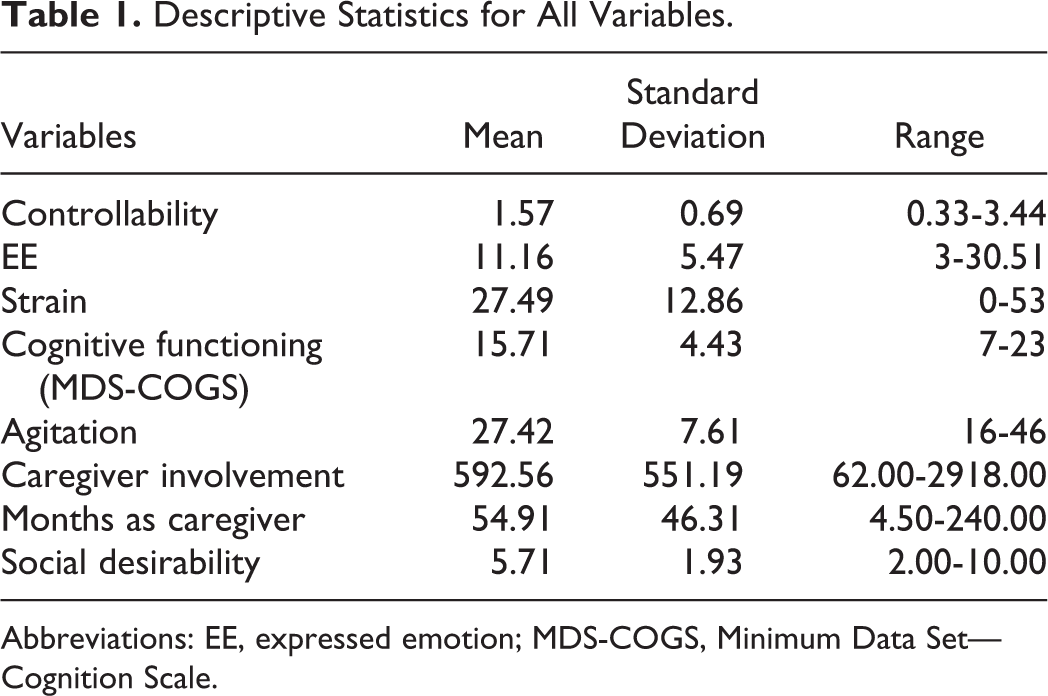
Abbreviations: EE, expressed emotion; MDS-COGS, Minimum Data Set—Cognition Scale.
Multiple Regression Analyses
Overall EE
We found a significant main effect for perceptions of controllability such that daughters who reported greater belief that their parent could control dementia-related behaviors reported higher levels of overall EE (β = 0.57, P < .001). In this analytic model, controllability accounted for 15.7% of the variability in EE when adjusting for all other covariates. Caregiver strain and caregiver involvement were also significantly associated with overall EE, accounting for 10.2% and 7.0% of the variability in EE, respectively.
Level of Expressed Emotion subscale analyses
Table 2 presents results from OLS regression analyses on each of the LEE subscales (Intrusiveness, Emotional Reactivity, Negative Attitudes, and Intolerance). Daughters who reported greater perceptions of parent control over dementia-related behaviors endorsed:
Simultaneous Multiple Regression Analyses Predicting Daughter Expressed Emotion Subscales From Controllability.a
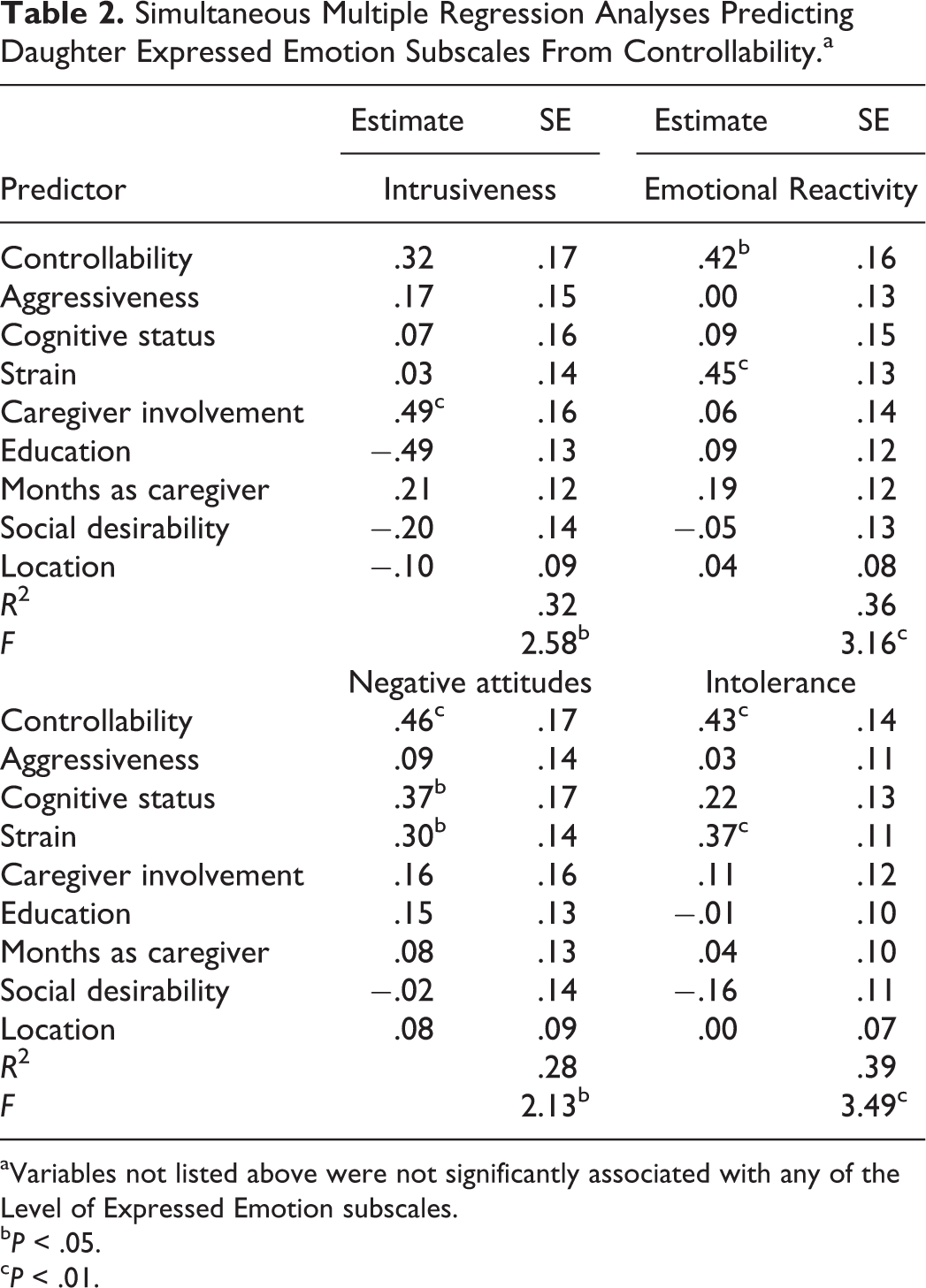
aVariables not listed above were not significantly associated with any of the Level of Expressed Emotion subscales.
b P < .05.
c P < .01.
being more emotionally reactive in ways that might increase parental distress (β = 0.42, P = .010), with controllability accounting for 9.1% of variability in emotional reactivity;
holding more negative attitudes (eg, belief that their parent “just wants attention” or “is exaggerating”) about their parent’s impairments (β = 0.46, P = .009), with controllability accounting for 10.8% of the variability in negative attitudes; and
being less tolerant of dementia-related behaviors (β = 0.43, P = .003), with controllability accounting for 12.1% of the variability in intolerance toward the care recipient (see Table 2).
Daughters who reported greater perceptions of controllability also reported higher levels of intrusiveness, but this finding was not statistically significant (β = 0.32, P = .07).
Discussion
These findings are consistent with our hypothesis that understanding what daughters believe about their parents’ dementia-related behavior is critically important to understanding the way a daughter interacts with their parent. For example, a daughter who believes her father’s aggressive behavior is due to his long-standing stubbornness (rather than dementia) is more likely to be emotionally reactive, hold negative attitudes, and intolerant toward that behavior.
Stress process models of caregiving (dating back to the 1990s) have conceptualized outcomes for both caregiver and care recipient as involving a complex interaction between background context, primary and secondary stressors, intrapsychic strains, and caregiver outcomes. 32 The findings from our study more specifically elucidate one aspect of the stress process model, bringing into focus the relationship between daughters’ interpretation of their parents’ behavior as controllable and its relationship to a range of negative aspects of the caregiving atmosphere. These aspects include emotional reactivity, negative attitudes, and intolerance for problematic behaviors. Although many aspects of caregiver experiences may be too difficult to alter (eg, secondary stressors such as financial strain or the care recipient’s cognitive impairment) or immutable (eg, caregiver personal history), psychological aspects of the caregiving experience offer an important target for intervention.
A focus on daughters’ attributions about their parents’ behavior may serve as an important strategy for intervention, as daughters’ high EE may contribute to or exacerbate the negative behaviors exhibited by their parent. Many caregiver interventions incorporate education regarding the anticipated symptoms, course, and nature of dementia. Such information may help daughters recognize aspects of the parents’ behavior attributable to the disease and not under the care recipient’s control. Making alternative attributions for problematic behaviors may translate into smoother interactions and less caregiver stress.
However, education about dementia can be a critical aspect of intervention for some caregivers, for others, this information may be redundant with material provided previously or researched by the caregivers themselves. In fact, the relationship between knowledge and caregiver outcomes may be complex, as greater knowledge of dementia may actually lead to more negative outcomes for some caregivers. 33 Among our sample of highly educated caregivers (70% having at least a college degree), it is possible that a significant portion of these daughters had reasonable expectations about the nature and course of dementia, thus it is particularly notable that subtle differences in the nature of caregiver attributions about care recipients in our sample remained associated with EE. Is it likely that the factors beyond knowledge about dementia, such as relationship history, contribute to the attributions that daughters make for their parents’ behaviors?
Caregiving occurs in the context of a family history that may impact a daughter’s attributions for parental behavior. For example, the relationship history for some parents and children can be fraught with long-standing conflict, frustration, or even abuse. Under these circumstances, it can be particularly challenging to evaluate the accuracy of attributions for problematic behaviors when those behaviors may have preceded the development of dementia. A long-standing history of problematic behaviors (such as aggression or abuse) by parents toward daughters may significantly complicate the caregiving dynamic in ways largely neglected by the caregiving literature. A thorough assessment of daughters’ needs and their relationship history may be helpful in identifying factors that impact daughters’ attributions and EE. These daughters may require more intensive psychosocial intervention to help process and mourn upsetting aspects of their relationship history and redefine the relationship with their parent in light of their new role as caregiver. Interventions that focus on family dynamics or address aspects of the daughters’ experience beyond dementia education may be critical for addressing the needs of these caregivers. For example, the New York University Caregiver Intervention is a family-based intervention that has been demonstrated to improve outcomes for both caregivers and care recipients. 34,35 Additionally, this intervention has been found to impact caregiver appraisal of the stressfulness of care recipient problem behaviors. 36 Although this intervention was designed for couples, the potential for the protocol to be adapted to address the unique dynamics associated with daughters’ caring for a parent with dementia offers 1 model for intervening in the interpersonal dynamics of daughters’ caring for a parent with dementia.
Limitations of the current study include the homogeneity in the sample’s demographic characteristics, which limit the generalizability of these findings to other populations. Additional studies are needed to compare and contrast these findings across cultural groups, kinship relationships, and educational levels. Additionally, given the cross-sectional nature of the study, beliefs in controllability may not have preceded EE, rather EE may result in increased behavioral problems that lead to greater frustration and more likely attributions of controllability. Studies that attempt to explore the trajectory of caregiver experiences over time would significantly clarify the temporal relationships among these variables. Finally, additional research on the interaction between relationship history, attribution patterns, and high EE would provide a better understanding of the impact of the historical context of the relationship dynamic between daughters and parents.
Footnotes
Authors’ Note
Work conducted at Department of Psychology/Institute on Aging, University of North Carolina–Chapel Hill, Chapel Hill, NC, USA.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants through the NIA/NIH (1T32 AG00272-01 A1) and the Sigma Xi Scientific Research Society. The PI’s continued work on the project is currently funded by a VA Health Services Research and Development (HSR&D) Career Development Award (CDA-2-10-023).