
Abstract
This cross-sectional study aimed to investigate the relationship between caregivers and care receivers, defined as home-dwelling family members with dementia. We used a self-rating questionnaire, the Felt Expressed Emotion Rating Scale (FEERS; 6 simple questions), to measure caregiver perceptions of the care receiver’s criticisms (CCs) and emotional overinvolvement (EOI) toward the caregiver. We performed factor analyses to rank single items on the FEERS pertaining to CC and EOI. We included 208 caregiver/care receiver pairs. Logistic regression analyses tested associations between FEERS items and caregiver and care receiver variables. The main contributors to caregiver perceptions of CC were the caregiver’s own distress and the amount of time spent with the care receiver. Socially distressed caregivers perceived the care receiver as emotionally overinvolved. When offering a psychosocial intervention, a tailored program should target the caregiver’s perceived relationship with the family member and the caregiver’s distress. The program should also endeavor to give the caretaker more opportunities for leisure time.
Introduction
Caring for a family member with dementia poses significant challenges. Caregivers are at increased risk of psychological 1,2 and physical morbidity. 3,4 Moreover, relationships between the individual with dementia and close family members have been shown to influence the course of dementia. A good relationship might slow the decline of cognitive and functional capacity 5 and delay nursing home admission 6 –8 ; in contrast, an attitude that reflects nonacceptance has been shown to predict a worse outcome. 9 The progression of dementia and the resulting disabilities are assumed to be stressful for both the patient and for the familial caregiver. This study addressed the emotional climate between these 2 individuals; that is, we examined how caregivers perceived the behavior and attitudes of a family member with dementia (familial care receiver) toward the caregiver.
Relationship quality has many facets that may vary according to gender and kinship, regardless of whether 2 relatives coreside or see each other regularly. Relationship factors have been extensively investigated. These factors have been linked to the concept of expressed emotion (EE), introduced by Brown and Rutter in the 1960s. 10 The EE concept reflects the relative’s attitude toward family members who are ill; the EE encompasses both positive and negative elements; thus, the scores are designed to indicate negative EE with high values and positive EE with low values. Critical attitudes and/or emotional overinvolvement (EOI) have been associated with a worse outcome, 11,12 and positive attitudes were regarded as protective against health problems. 13,14 Originally formulated for studies on psychosis, 10 the EE might also reveal influences on other medical and psychological conditions, including dementia. 11 A previous review demonstrated that high EE values were attributable more to criticism (CC) than to EOI; moreover, caregiver perceptions of CC were lower when the care receivers had dementia compared to other diseases. 11 However, few studies have focused on EE and dementia. Those studies showed that high caregiver EE values were related to strain, burden, distress, 15 –17 lack of psychological well-being, depression 18 –20 and gender, which is being a female. 21 High EE values can also result from problems in the interpersonal relationship, 21 and a poor social network for the caregiver. 17,19,21 These conditions may cause the caregiver’s coping strategies to become maladaptive, and the person with dementia may respond with increased negative behavior. 22 Overinvolved caregivers become worn-out, do not put limits on their care responsibilities, and they often make unrealistic claims about the quality of care they are giving. 17,21 When caregivers had high EE, they perceived the care receivers’ functional ability declined and more declined than the care receiver perceived own ability. 23 High EE relatives also tended to attribute the care receivers’ problems as personal factors that were controllable by the care receiver. 24 However, those studies mainly focused on the effect of EE on the family member who was ill, and less attention has been given to the caregiver’s perceptions of the attitudes of a familial care receiver toward the caregiver. Because relationships are based on reciprocity, we must assume that the caregiver’s responses and attitudes are influenced by their perceptions of the familial care receiver’s attitudes toward them (the caregiver). Investigation of the emotional and psychosocial factors within the family is warranted, because caregivers are at high risk of stress-related health problems, due to the burden associated with caring for a family member with dementia. Hence, it is important to identify which factors of the care receivers and caregivers themselves that explain caregivers’ perceived relationship quality and the strength of possible explaining factors.
To investigate caregiver perceptions of the familial care receiver’s attitudes toward them, we used a short questionnaire, the Felt Expressed Emotion Rating Scale (FEERS). 25 Based on the concept of EE where EE is measured in caregivers and related to care-receiver outcome, the FEERS measures perceived CC and perceived EOI from the perspective of the caregiver. We implemented the FEERS questionnaire to evaluate the quality of the relationship between a primary caregiver and a care receiver who was a family member with dementia.
We hypothesized that the caregiver’s perceptions of the attitudes projected by the person with dementia toward them would be influenced by (1) the caregiver’s own level of distress, (2) the caregiver being a female, (3) the mental and functional consequences of dementia, and (4) the behavioral symptoms of the family member with dementia (see Figure 1).

Caregiver and care receiver characteristics influence on caregiver’s perceived relationship.
Materials and Methods
This study had a cross-sectional design. Individuals with dementia and their familial caregivers were recruited from both memory clinics and home nurse districts by local project coworkers in 19 municipalities in Norway. Individuals with dementia and their familial caregivers (dyads) were eligible to participate in the present study, when the care receiver had been diagnosed with dementia according to International Classification of Diseases, Tenth Revision criteria, 26 had a score of at least 15 points on the Mini-Mental State Examination (MMSE), and having the capacity to give informed written consent to participate in the study. The care receivers were living at home and had at least weekly face-to-face contact with the caregiver. No specific exclusion criteria were defined. However, in the analysis process, 15 (7%) dyads were excluded from this study, because the caregivers were more distant relatives or friends. Six dyads with incomplete FEERS data were also excluded, leaving 208 dyads for the study. The data were collected by trained nurses and occupational therapists. Participants were enrolled from October 2009 to May 2011.
Measures
The questionnaires were completed by the participating caregivers and care receivers, eventually with some assistance from the coworker during the interviews.
The FEERS is a 6-item questionnaire based on the EE theory, which was developed by H. Bentsen in 1993 and used in a Phd-Thesis by Smeby.
25
Caregivers and their familial care receivers were asked 6 questions relating to their perceptions of their family member’s attitudes toward them during the past month. How critical do you feel he/she has been toward you during the last month? How much do you feel he/she has worried about you during the last month? How often do you feel he/she has treated you as an independent individual during the last month? How much do you feel he/she has appreciated you during the last month? To what extent have you felt yourself controlled by him/her during the last month? How often have you felt respected by him/her during the last month?
The questions were rated on an anchored Likert scale from 0 (not at all) to 5 (to an extreme degree). The Norwegian FEERS instrument was translated into English and back-translated into Norwegian to ensure optimal translation quality.
Caregivers also completed 3 other questionnaires. The first was the Geriatric Depression Scale (GDS), an instrument that screens for depression, tailored for older persons. 27 The GDS consists of 30 items, scored as absent = 0 or present = 1. A cutoff score ≥11 was used to identify probable cases of depression. 28 A sum score >11 indicates depression with a sensitivity of 84% and a specificity of 95%. 29 The second was the Relatives’ Stress Scale (RSS), 30 a questionnaire with 15 questions, scored at 5 levels of intensity, from 0 (not at all) to 4 (to a high degree). These scores were evaluated by a factor analysis method with a 3-factor solution to identify emotional distress, social distress (eg, feelings of being limited in terms of social life), and negative feelings. 2,30 The third was the short form of the Neuropsychiatric Inventory (NPI-Q), which covers neuropsychiatric symptoms in the patients. 31 This instrument included 12 items with a severity sum score that ranged from 0 (no symptoms) to 36 (severe symptoms). In this study, we used a dichotomous scale to indicate the presence or absence of symptoms, and the sum score ranged from 0 to 12.
Care receivers were evaluated with 3 standardized instruments: The Cornell, a proxy-based instrument, was designed for evaluating depression in persons with dementia. It consisted of 19 items with a score of 0 to 2 for each item.
32
A higher score indicated more symptoms of depression, and the total score was between 0 and 38. A cutoff score ≥8 was used to indicate depression.
33
The Instrumental Activities of Daily Living (I-ADL) Scale was used to assess function.
34
Each item was rated on a 3 to 5 level scale, from 1 (independent) to 5 (totally dependent), with a total score of 31. The MMSE was used to assess cognitive function.
35
The scale consisted of 20 items, rated on a scale from 0 to 30, where a higher score indicated better cognitive function.
For both caregiver and care receiver, we recorded the age, gender, kinship, and living arrangements. In addition, we recorded the duration of symptoms and the type and amount of formal and informal assistance from family or friends.
Statistical Analyses
Continuous variables were expressed as the mean and standard deviation (SD); categorical data were expressed as counts and proportions. The Spearman rank correlation coefficient was used to explore crude associations between the caregiver’s and care receiver’s perceived FEERS. Data from the 3 RSS variables (emotional, social, and negative feelings), and the NPI-Q variables were normally distributed; thus, differences were tested with parametric tests. The GDS and Cornell data were skewed; hence, differences were tested with nonparametric methods. The reliability of the FEERS questionnaire was assessed with a factor analysis and Cronbach α.
To assess the stability of the instrument, a separate group of 39 caregivers and care receivers from a memory clinic was asked to complete the questionnaire twice, separated by an interval of 3 days. We analyzed the test–retest reliability of the FEERS with intraclass correlation coefficients (ICCs).
For variables with 20% or fewer missing scores, the missing item scores were replaced by the total mean.
Crude differences between groups regarding continuous variables were assessed with t tests. The FEERS-CC, FEERS-EOI, and FEERS-total were modeled with univariate and multiple logistic regressions to investigate possible associations between selected variables and binary outcome variables. Variables with P values ≤.10 in the bivariate analysis were entered into the multivariate analysis. All multivariate models also included the ages and genders of caregivers and care receivers. Variables with a P value ≤.05 in the multivariate analysis were retained in the models. The results are expressed as odds ratios (ORs) with 95% confidence intervals. All tests were 2-sided. P values <.05 were considered statistically significant. Statistical analyses were performed with the statistical program SPSS, version 23.
Ethical Aspects
The study followed the ethical principles outlined in the Helsinki declaration. 36 The Regional Committee for Ethics in Medical Research, Southern-Eastern Norway, and the Norwegian Data Inspectorate approved the study. In brief, the participants were given oral and written information about the study, and written informed consent was obtained from each participant. The participants were also informed that they could withdraw consent and discontinue participation in the study at any time without giving a reason.
Results
Caregiver Characteristics
Compared to male caregivers (Table 1), female caregivers were significantly younger (P = .01) and reported more burden on the RSS (P = .02). Moreover, female caregivers reported more depressive feelings than males on the GDS (P < .001). In addition, female caregivers had higher scores than males on 2 of the FEERS clusters (FEERS-EOI, P = .005 and FEERS-total, P = .05). The FEERS-CC values were not significantly different between female and male caregivers.
Characteristics of the 208 Caregivers and Care Receivers.
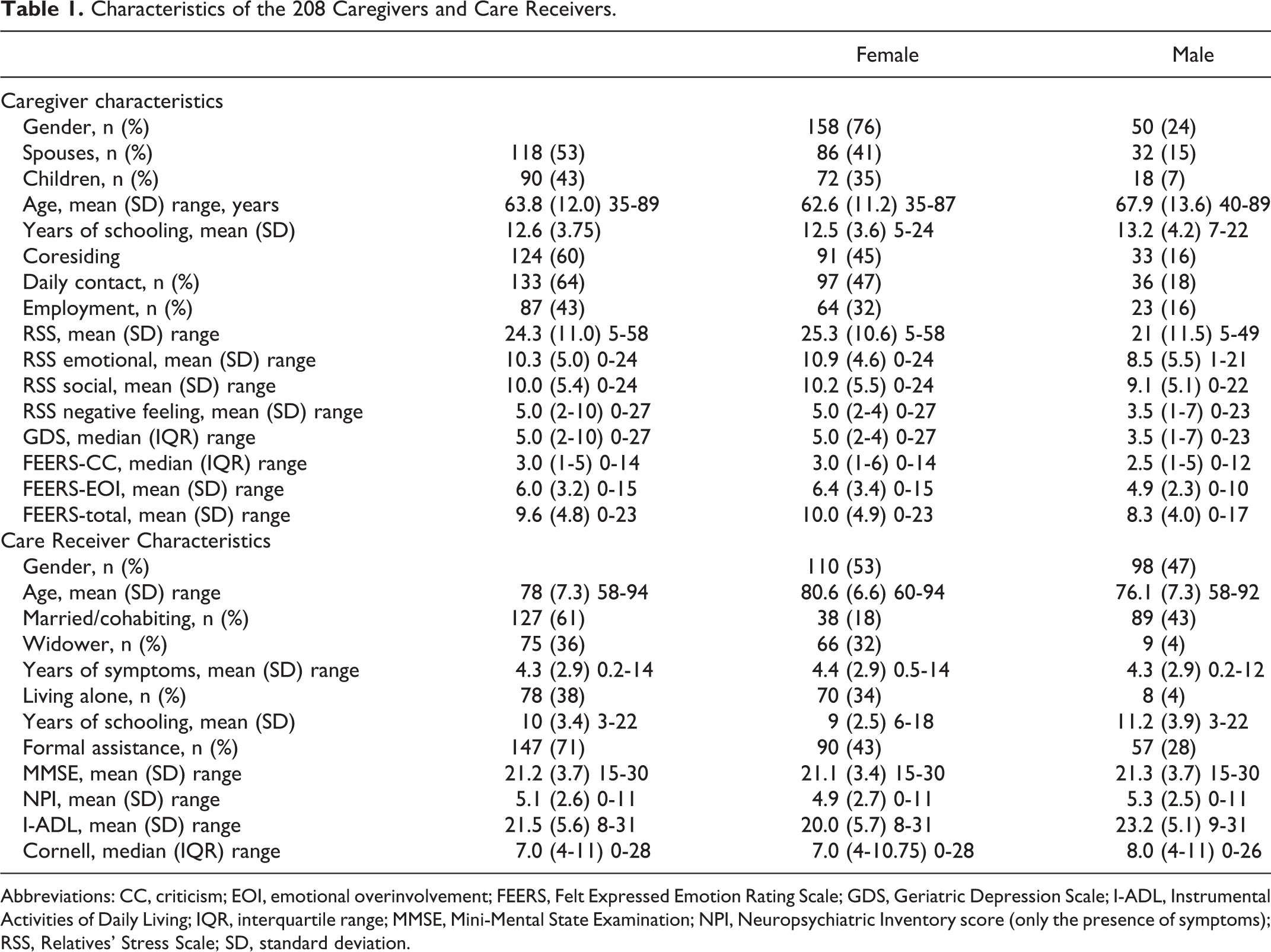
Abbreviations: CC, criticism; EOI, emotional overinvolvement; FEERS, Felt Expressed Emotion Rating Scale; GDS, Geriatric Depression Scale; I-ADL, Instrumental Activities of Daily Living; IQR, interquartile range; MMSE, Mini-Mental State Examination; NPI, Neuropsychiatric Inventory score (only the presence of symptoms); RSS, Relatives’ Stress Scale; SD, standard deviation.
Reliability Analysis of FEERS
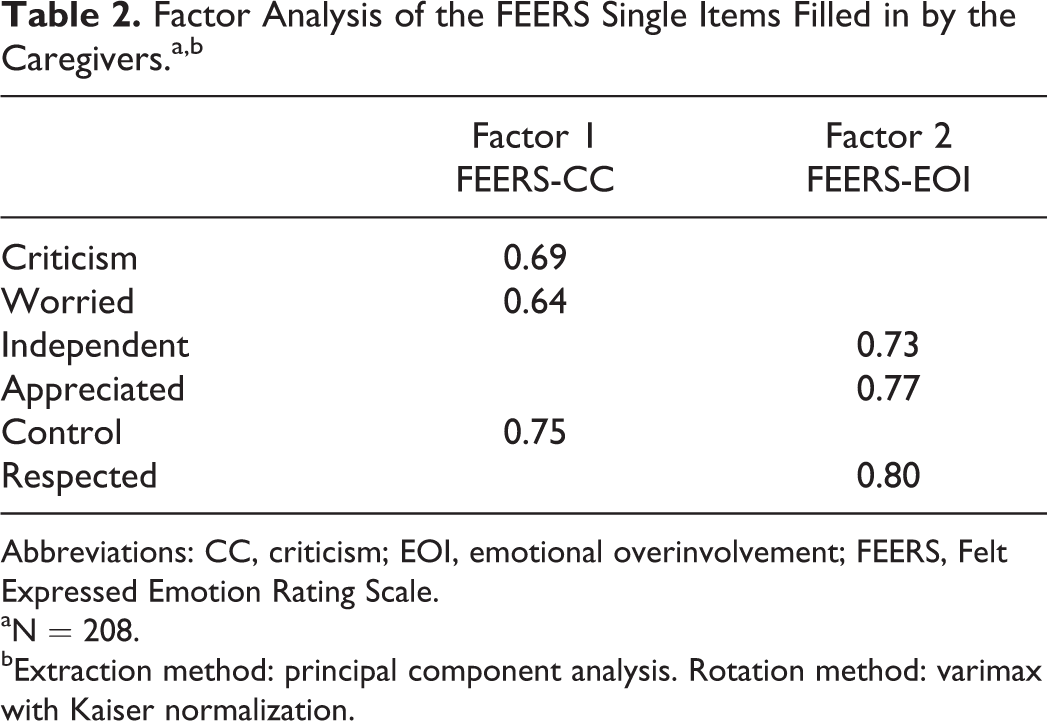
The factor analysis revealed that item numbers 1 (CC), 2 (worry), and 5 (control) contributed most to the FEERS-CC subscale (Table 2). In contrast, items 3 (independence), 4 (appreciation), and 6 (respect) contributed most to the FEERS-EOI subscale (Table 2).
Factor Analysis of the FEERS Single Items Filled in by the Caregivers.a,b
Abbreviations: CC, criticism; EOI, emotional overinvolvement; FEERS, Felt Expressed Emotion Rating Scale.
aN = 208.
bExtraction method: principal component analysis. Rotation method: varimax with Kaiser normalization.
Furthermore, reliability of the FEERS instrument was measured by calculating Cronbach α for the FEERS-CC and FEERS-EOI subscales. Internal consistency calculated for caregivers showed Cronbach α of .52 for FEERS-CC and .82 for FEERS-EOI. The item “worry” was weakly associated with CC and control; hence, excluding the worry item from the FEERS-CC cluster increased its Cronbach α to .66.
The test–retest reliability of the FEERS was measured with ICCs. The ICCs for the caregivers were FEERS-CC = 0.83, P < .001; FEERS-EOI = 0.94, P < .001; and FEERS-total = 0.73, P = .01. The ICCs for the care receivers were FEERS-CC = 0.70, P = .001; FEERS-EOI = 0.73, P < .001; and FEERS-total = 0.60, P = .001.
Correlation analyses were performed to investigate the agreement between the caregiver’s and the care receiver’s perceptions of the shared relationship. Our data revealed a statistically significant, but weak correlation between the 2 perceptions. The correlations were FEERS-CC: r = .32 (P ≤ .001), FEERS-EOI: r = .15 (P = .03), and FEERS-total: r = .23 (P = .001).
Bivariate Associations
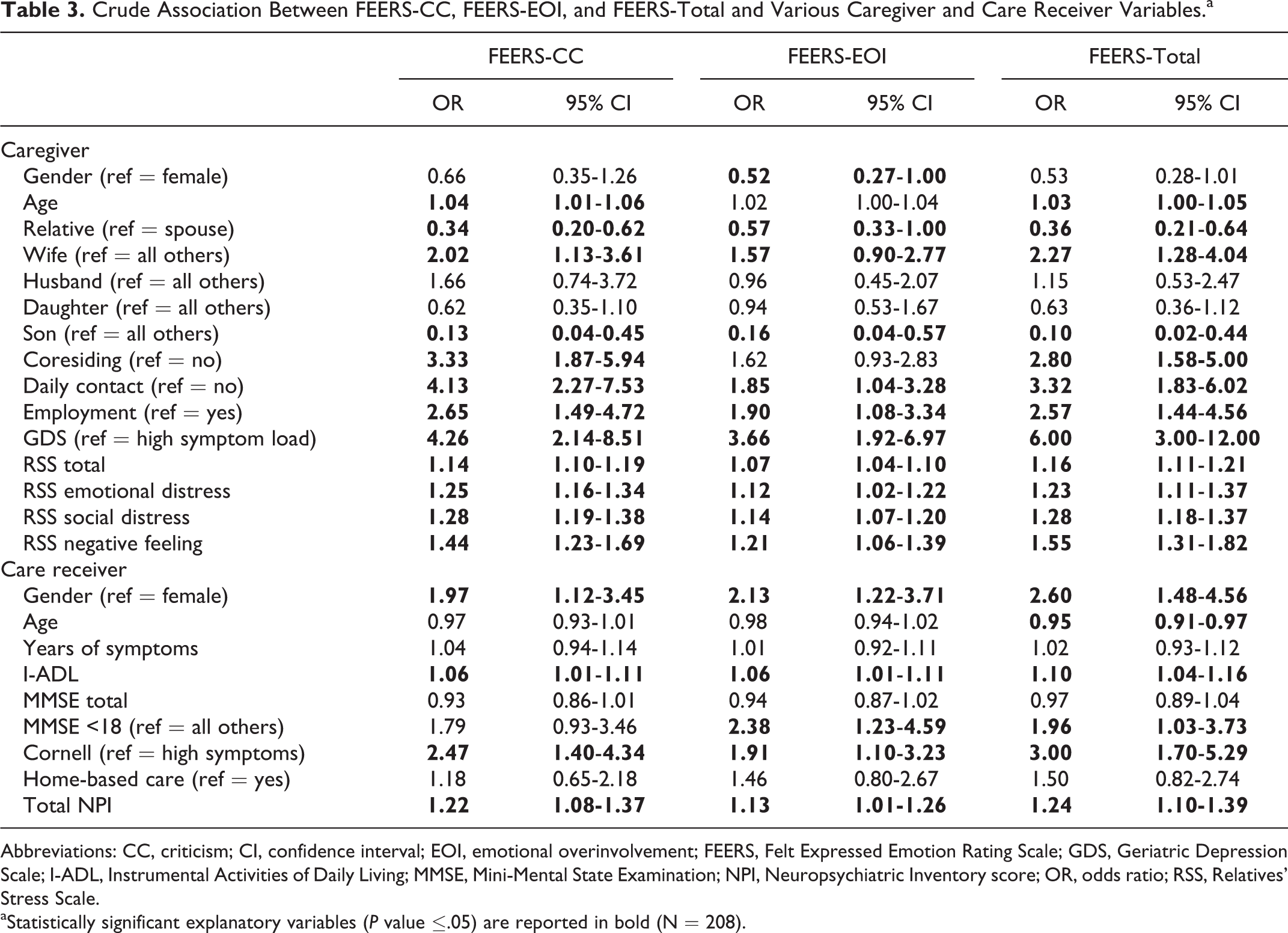
Logistic regression analyses were performed to explore crude associations between selected variables. The dependent variables were dichotomized using the medians as the cutoff: FEERS-CC <3.0≥; FEERS-EOI <6.0≥; and FEERS-total <8.0≥. Results from these analyses are shown in Table 3.
Crude Association Between FEERS-CC, FEERS-EOI, and FEERS-Total and Various Caregiver and Care Receiver Variables.a
Abbreviations: CC, criticism; CI, confidence interval; EOI, emotional overinvolvement; FEERS, Felt Expressed Emotion Rating Scale; GDS, Geriatric Depression Scale; I-ADL, Instrumental Activities of Daily Living; MMSE, Mini-Mental State Examination; NPI, Neuropsychiatric Inventory score; OR, odds ratio; RSS, Relatives’ Stress Scale.
aStatistically significant explanatory variables (P value ≤.05) are reported in bold (N = 208).
Our data revealed that the kinship between the caregiver and the care receiver was significantly associated with all FEERS items. Wives were twice as likely as other relatives to perceive their care receivers as both critical and emotionally over involved. Wives reported high scores on the FEERS-total compared to other caregivers. There was no difference between husband and daughter caregivers, but sons were less likely than other relatives to perceive the care receiver as critical or emotionally overinvolved. Caregivers that coresided or, in particular, had daily contact with their care receiver had higher odds of perceiving CC and EOI; these caregivers had high FEERS-total scores compared to caregivers with less care receiver contact. Furthermore, caregivers without work outside the home were 2.5 times more likely to perceive the care receiver as critical and emotionally over involved compared to caregivers with outside employment (for details, see Table 3).
For each point of increase in the RSS total, the likelihood increased by 14% that caregivers perceived their care receiver as critical toward them. The 3 components of RSS: emotional distress, social distress, and negative feelings, all contributed strongly to this marked increase of perception of CC (OR: 1.25, 1.28, and 1.44, respectively).
The likelihood that a caregiver would perceive a care receiver as critical and emotionally over involved was twice as high for male as for female care receivers. Other factors that contributed to high FEERS scores were reduced ADL function and depression in the care receiver. In contrast, only cognitive impairment with an MMSE <18 in the care receiver was associated with the caregiver FEERS-EOI score. Our data revealed that the use of formal care and the duration of symptoms were not associated with the caregiver’s perceptions of the care receiver’s attitudes.
Multivariate Analyses
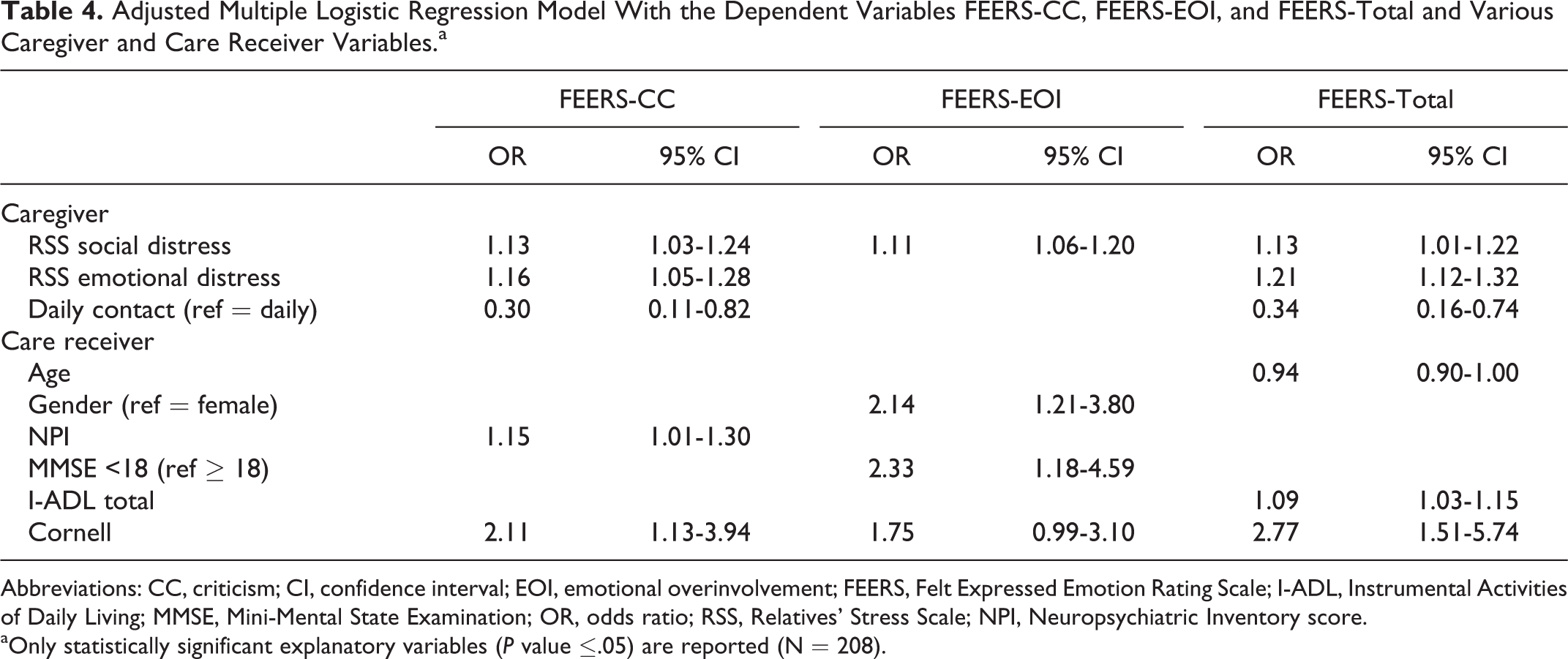
Results from the multivariate analyses on caregiver and care receiver characteristics are listed in Table 4.
Adjusted Multiple Logistic Regression Model With the Dependent Variables FEERS-CC, FEERS-EOI, and FEERS-Total and Various Caregiver and Care Receiver Variables.a
Abbreviations: CC, criticism; CI, confidence interval; EOI, emotional overinvolvement; FEERS, Felt Expressed Emotion Rating Scale; I-ADL, Instrumental Activities of Daily Living; MMSE, Mini-Mental State Examination; OR, odds ratio; RSS, Relatives’ Stress Scale; NPI, Neuropsychiatric Inventory score.
aOnly statistically significant explanatory variables (P value ≤.05) are reported (N = 208).
The results showed that the RSS item, social distress, was the strongest independent predictor of caregiver perceptions of their care receiver’s attitudes. This association was strong and statistically significant for FEERS-CC, FEERS-EOI, and FEERS-total. The FEERS-total model revealed that care receiver age, functional decline (I-ADL score), and depression (Cornell) were significantly associated with the FEERS-total score After controlling for the above-listed variables, compared to caregivers that were not socially distressed, socially distressed caregivers were 13% more likely to perceive their care receiver as critical and emotionally over involved, and 11% more likely to score their care receiver high on the FEERS-total. Additionally, emotional distress among caregivers accounted for 16% of the perceived FEERS-CC from the care receiver. Caregivers with daily care receiver contact had more than triple the odds of feeling criticized compared to caregivers with less frequent contact. The odds of caregivers perceiving CC were 15% higher for care receivers with more neuropsychiatric symptoms (NPI-Q assessment) and more than twice as high for care receivers with depression (Cornell assessment) compared to care receivers with fewer symptoms and no depression (for details, see Table 4).
When the models were controlled for both caregiver and care receiver variables, the remaining independent explanatory variables for FEERS-CC, FEERS-EOI, and FEERS-total scores were related to the caregiver’s own distress. Social distress, emotional distress, and daily contact contributed to the caregiver’s perceptions of their care receiver’s FEERS-CC. High level of social distress and female gender of the caregiver contributed to the perceived FEERS-EOI of the care receiver. The care receiver age and their ability to perform I-ADL assessment were significantly associated with the FEERS-total; however, these associations were weak, hence, they had low clinical relevance (for details, see Table 5).
Adjusted Multiple Logistic Regression Model With the Dependent Variables FEERS-CC, FEERS-EOI, and FEERS-Total and Selected Variables From Table 4.a
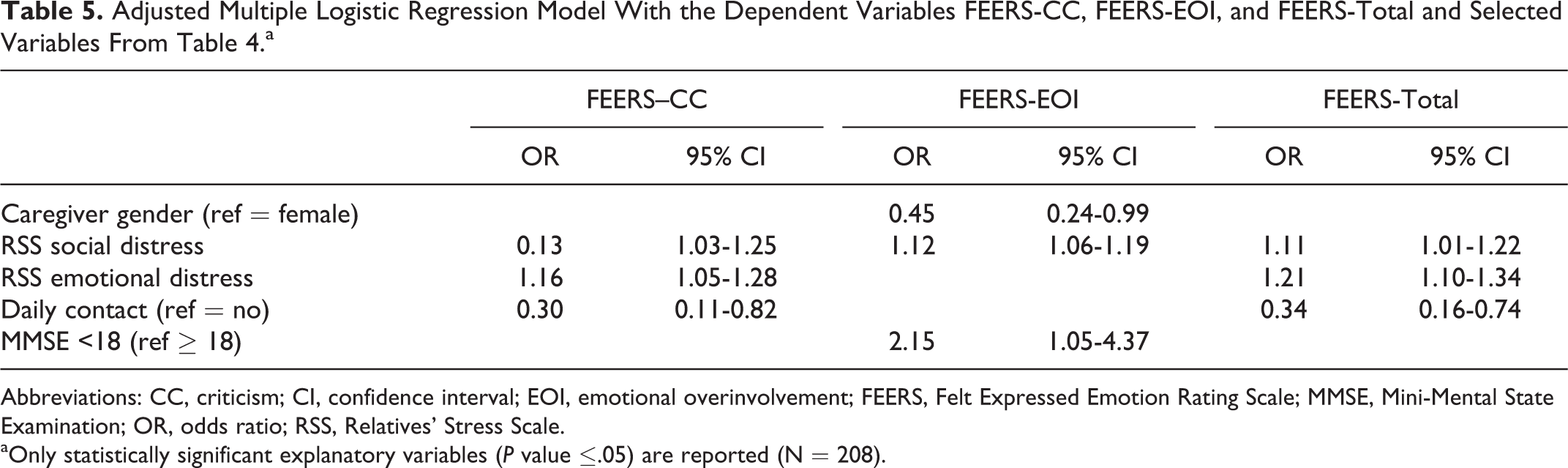
Abbreviations: CC, criticism; CI, confidence interval; EOI, emotional overinvolvement; FEERS, Felt Expressed Emotion Rating Scale; MMSE, Mini-Mental State Examination; OR, odds ratio; RSS, Relatives’ Stress Scale.
aOnly statistically significant explanatory variables (P value ≤.05) are reported (N = 208).
Discussion
Our main finding was that both caregiver and care receiver characteristics contributed to the caregiver’s perceptions of the care receiver’s CC and/or EOI according to the FEERS toward them. Moreover, the most important single factor related to the caregiver’s perceptions of care receiver’s attitudes was the caregiver’s own social distress (assessed with the RSS). Indeed, caregiver social distress contributed significantly to all 3 multivariate models (FEERS-CC, FEERS-EOI, and FEERS-total). One possible pathway is that, as dementia progresses, the care receiver becomes more dependent on their caregiver; then, overtime, this dependence might lead to restrictions on the caregiver’s social life, and subsequently, feelings of isolation. Our finding might be related to other studies that claimed that social isolation led to increased risk of caregiver burden. 37 –39
Furthermore, CC has been linked to the caregiver having a poor social network. 17,19,21 However, those studies focused on caregivers’ attitudes; in contrast, our study tapped caregivers’ perceptions of care receiver attitudes. Theoretically, we might assume that receiving assistance from the community might give the caregiver more opportunities for leisure time. However, our study results suggested that receiving formal assistance did not influence caregiver’s perceptions of their care-receiver’s attitudes toward them. This lack of effect may have occurred because formal assistance was primarily time-limited, and it focused on assisting the care-receiver with ADL-related functions; thus, this assistance did not alleviate the caregiver’s concerns. Additionally, some dyads might disagree on the need for assistance from the community, and this disagreement may lead to conflicts between the 2. For some patients, dementia makes it difficult to judge one’s own ability. Hanson and Clarke 23 found that disagreements in the dyad about the abilities of a care receiver with dementia most frequently occurred when the environment was characterized by CC and EOI. Hence, providing these dyads with effective assistance would require a thorough evaluation of both the caregiver’s and the care receiver’s situations. This strategy emphasizes the importance of developing services that are adapted to the family members needs during the early stages of dementia.
The 2 most important explanatory factors that contributed to the caregivers’ perceived CC were emotional distress (RSS assessed) and the amount of contact. Emotional distress could be considered a dimension of depression; thus, it may be linked to the proposal from Hooley and Teasdale 40 that individuals with depression were particularly sensitive to perceived CC from the spouse toward them. Additionally, they suggested that the perception of being criticized was crucial to the health of individuals with depression. When depressed, people are more prone to interpret ordinary interactions negatively, as conflicts within the family. 41 This susceptibility might induce stress in caregivers with depression. Consistent with other studies, 1,6,21 this susceptibility may explain our finding that caregivers that were emotionally distressed were more likely to interpret their care receiver as critical. On the other hand, the experience of being criticized may also increase the risk of depression. Moreover, caregiver perceptions of CC were also linked to the care-receiver’s neuropsychiatric symptoms (NPI-Q assessment) and depression (Cornell assessment). Hence, both the care receiver’s behavior and mood could contribute to the perceived attitude. This finding was consistent with other studies that found that neuropsychiatric symptoms contributed most to stress in caregivers. 2,42 –44 However, our last model (Table 5) showed that the influence of these factors disappeared when we controlled for all other variables. This result suggested that the care receiver’s attributes only contributed to the caregiver’s feeling of CC, when the caregiver was under significant stress from social distress, emotional distress, and/or extensive contact with the care receiver.
In contrast to the FEERS-CC, the caregiver’s perceived FEERS-EOI was somewhat influenced by the receiver’s cognitive function. This result was shown with the FEERS-EOI model, where more cognitive impairment (MMSE assessed) was associated with lower FEERS-EOI scores. That is, when the care receiver had poor cognitive function (MMSE < 18), the caregiver felt very little EOI from their care receiver. This result suggested that the caregivers might have understood that the care receiver’s attitudes resulted from the illness. Indeed, Bentsen et al 45 also showed that the care receiver’s cognitive ability had an impact on the caregiver’s attitude in a study on patients with schizophrenia. They found that caregivers were less negative toward patients with cognitive deficits compared to patients with normal cognition. In that study, the caregivers attributed the behavior to the illness, and they assumed it was not under the control of the patient. We speculate that this attribution might also occur among caregivers of family members with dementia.
Furthermore, the caregiver’s perceived FEERS-EOI was influenced by caregiver gender. Along with the RSS of social distress, caregiver gender remained a significant factor after controlling for all other variables (Table 5). This result suggested that watching the decline of their care receiver might influence male and female caregivers differently. Providing care was a new role for these family members, and they all had to adapt to changing circumstances as the dementia evolved. In our cohort, female spouses and daughters comprised a substantial proportion of the caregiver group. This observation suggested that female relatives might assume the role of caregiver more often than male spouses and sons. Some potential explanations for this propensity of female caregivers could be that women may perceive their responsibility differently than men, or they may become more emotionally distressed than men about a family member getting a chronic mental illness. The latter possibility is consistent with the stress model proposed by Pearlin et al, 46 which showed that women dealt with stress differently from men. They found that women were more emotional in their approaches, and men were more task-oriented. Furthermore, a daughter’s social distress could be related to her double role as the mother of her own family, having employment and her responsibility of caring for a diseased parent. Thus, although her children may have grown up, she must assume a new role of caring for her aging relatives. Going from one caring role to the next might cause her to feel isolated, unable to command her own life, and a desire for freedom from caring obligations.
Overall, this study showed that the FEERS scores were relatively low for caregivers’ perceptions of care receiver CCs and EOI. These findings were consistent with other studies, 11,22 which showed that caregivers tended to report lower EEs when care receivers had dementia compared to when care receivers had other diseases, for example, schizophrenia. The explanation for this finding might arise from either side; for example, care receivers may become less critical and less emotionally overinvolved, as they realize they are dependent on the caregiver; this attitude could lead to reduced conflict between the caregiver and care receiver. Another explanation could be the limited reciprocity in the caregiver’s and care receiver’s perceived attitudes; care receivers tend to have slightly more positive perceptions of their caregiver’s attitude. However, care receivers might not necessarily show these attitudes, and the caregiver’s own level of stress has great influence over their perceptions of their care receiver’s attitudes. This lack of reciprocity was supported by Wright, 47 who found that, among patients with dementia, couples showed little congruity in their perception of their relationship; also, Hanson and Clarke 23 found that individuals with dementia had more positive perceptions of the overall quality of the marriage than did their spouses. 47 This issue is worth investigating in the familial care scenario. Offering families community service assistance early in dementia progression might facilitate the process of dealing with changing relationships and expectations between family members; this facilitation may prevent adverse interactions that can increase stress and the risk of stress-related health problems.
Limitations
Although the FEERS subscales achieved acceptable values in the component analysis, it may be asked whether the FEERS subscales are comparable to the Camberwell Family Interview (CFI) subscales. The Cronbach α showed that the FEERS-CC had low internal consistency. The “worry” item seemed to abolish the internal consistency; thus, it might indicate another dimension of the FEERS-CC subscale. For example, worry might be considered a positive attitude. The “control” item might be discussed belonging to either of the CC and EOI subscale. As contradictory findings argue control belonged to EOI 48 (Peterson and Docherty, 2004), Hooley and Campbell 49 found controlling behavior was associated with CC in caregivers of patients with schizophrenia and depression. Typically, EE is measured with the CFI, 50 which is considered the gold standard. It is debatable to what extent the FEERS is comparable to the CFI, because the FEERS measures self-rated perceptions of the relationship quality. However, the FEERS is rapid, and it can be readily introduced into clinical practice to assess the caregiver’s experience. Hence, it could facilitate the development of an appropriate psychosocial intervention directed to the caregiver’s needs, including information about dementia. Additionally, the deliberate use of day centers where there is a need to reduce face-to-face contact between caregiver and care receiver due to high FEERS -CC and FEERS-emotional overinvolvement or high levels of burden.
Because this study was cross-sectional, we know little about how relationships between caregivers and care receivers developed over time. Thus, we could not determine whether the caregivers’ perceptions of their care receivers’ attitudes resulted from the dementia process or were related to a conflicted relationship that predated the dementia. Additionally, we could not determine whether the stress in caregivers represented a reaction to dementia progression or a personality trait. Hence, more studies are needed to elucidate the development of caregiver perceptions of care receiver attitudes. As dementia nowadays is diagnosed in earlier stages of the disorder, depth interviews with the care receiver could also shed light on their view of the caregiver. Such an interview could be useful to explore the veracity of caregivers’ perceptions as caregivers’ own stress influence their perception of their care-receivers’ attitude and behavior.
Conclusion
This study showed that caregiver distress and the amount of contact with the care receiver were the main contributors to their perception of CC from the care receiver. In particular, socially distressed female caregivers were most likely to perceive the care receiver as emotionally overinvolved. The FEERS measured the caregiver’s perceptions of care receiver attitudes, which did not necessarily reflect the care receiver’s actual attitudes. Large incongruities between the caregiver’s and care receiver’s perceptions of their relationship imply that distressed caregivers need assistance in modifying their perception of negative attitudes from their care receiver. Thus, a tailored intervention program should target the caregiver’s own distress and help them find opportunities for more leisure time.
Footnotes
Authors’ Note
Data for the study can be accessed by contacting first author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.