
Abstract
Despite the prevalence of dementia among residents in assisted living (AL), few researchers have focused on the length of stay (LOS) in AL among this population. Little is known about the factors that may contribute to LOS in these settings, particularly for residents with dementia. In the current study, a sub-set of AL residents with dementia (n = 112) was utilized to examine whether marital status was associated with LOS in AL as this has received sparse attention in previous research despite studies suggesting that marital status influences LOS in other health-care and long-term care settings. The Andersen-Newman behavioral model was used as a conceptual framework for the basis of this study of LOS, marital status, and dementia in AL. We hypothesized that persons with dementia who were married would have longer LOS than unmarried persons with dementia in AL. Cox regression was used to examine the association between marital status and LOS in AL of residents with dementia and whether activities of daily living were related to discharge from AL settings among married and unmarried residents with dementia. Main effects for marital status and the interaction between marital status and mobility with LOS were examined. Study findings provide information related to the psychosocial needs of AL residents with dementia and offer implications for assessing the on-going needs of vulnerable AL residents.
Background
Across the United States, assisted living (AL) is one of the fastest growing areas of long-term care services and supports for older adults. 1 The AL is broadly defined as a residential care facility providing 24/7 supervision and assistance related to personal and health services in activities of daily living (ADLs). 2 Based on the projected growth in the number of older adults, AL settings have become an important platform for the delivery of housing and supportive services for this population. 3,4 Although AL settings are designed to minimize the needs of older adults to relocate to more institutional care settings, 2 more research is needed to better examine the factors that influence length of stay (LOS) in AL, particularly for residents with dementia. Recent statistics suggest that almost half (42%) of residents in these communities were diagnosed with Alzheimer’s disease (AD) or other dementias. 5 Some experts have estimated that as many as 7 of 10 residents in AL settings have cognitive impairment or dementia. 6 Thus, AL has become a leading provider of residential care for older adults with dementia.
Despite the prevalence of dementia among residents in AL, few researchers have focused on the LOS in AL among this population. In addition, most AL settings are committed to helping residents “age in place,” that is, live in the same residence for as long as possible to avoid the traumas associated with frequent relocations. However, little is known about the factors that may contribute to LOS in these settings, particularly for residents with dementia. The symptoms of dementia are often an influential factor for residents relocating from an AL to a nursing home setting. 7 Research further suggests that residents with behavioral symptoms associated with cognitive deficits are more likely to be discharged from AL, although this varies among AL settings. 6 Previous research suggests that a significant number of residents in dementia-specific AL settings transferred to skilled nursing facilities over 9 months. 8 However, residents in specialized AL dementia settings may be more likely to age in place as they are less likely to be discharged for behavioral symptoms. 6 Researchers also found significantly longer LOS to be associated with the utilization of an aging in place model coupled with a willingness to provide palliative care. 9
Many persons with dementia will ultimately face nursing home placement, which adds significant stress on the person with dementia as well as family members. 10 Depression, agitation, decreasing cognition, frailty, and falls in people with dementia are factors most highly linked to nursing home placement. 10 The primary reason for direct admission from a hospital to a nursing home facility in older adults with dementia is a disturbance in behavior. Once dementia has been identified, older adults with the condition are rarely included in decisions regarding their treatment and the discharge destination. 11 Although family members and caregivers report improvement in quality of life following institutionalization, older adults with dementia often experience a significant decline in quality of life. 10 Research also suggests that many AL facilities may have difficulty in managing the care of persons with dementia. 12 Furthermore, AL staff may have inadequate training to manage the care needs of persons with dementia in these settings. 13
In a seminal study that focused specifically on the effects of dementia on time to discharge from AL settings in 22 facilities located in central Maryland, researchers found that residents with dementia remained in the facility 209 fewer days than residents without dementia using t tests to compare the 2 groups. They also suggested that the LOS might be influenced by activity participation and improved mobility. 14 Several other studies 15 have found that residents with dementia in AL settings have a shorter LOS and that as these residents’ behaviors and functional limitations worsen, most facilities transfer these older persons to nursing homes. Unfortunately, these researchers did not control for marital status, which could influence LOS in AL. In the current study, the researchers examined whether marital status was associated with LOS in AL as this has received sparse attention in previous research despite studies suggesting that marital status influences LOS in other health-care and long-term care settings.
Marital status has been examined as a factor for LOS in a variety of clinical settings that serve older adults including in-patient rehabilitation, 16 hospitals, 17 and nursing homes. 18 Furthermore, according to previous research, older adults who do not have spouses are more likely to be admitted to nursing homes. 19,20 Given that previous research suggests that marital status influences LOS in clinical settings and admission to nursing homes, we hypothesized that persons with dementia who were married would have longer LOS than unmarried persons with dementia in AL. Our intent in this study was to increase the knowledge about factors influencing LOS in AL. To our knowledge, this study is the first to focus on the role of marital status on LOS among residents with dementia in AL.
The Andersen-Newman behavioral model 21,22 is one of the most widely used frameworks to explain health-care utilization, including LOS, in care settings that serve older adults such as hospitals, 23 nursing homes, 24 and home health. 25 Therefore, this model was used as a conceptual framework for the basis of this study of LOS, marital status, and dementia in AL. The Andersen-Newman framework encompasses 3 domains—(1) predisposing factors for service use (eg, age, gender, and marital status), (2) enabling factors that provide individuals with the ability to secure services (eg, family and community supports), and (3) need factors that reflect the reason why services are needed (eg, physical and functional problems). 22 In this study, the authors will explore marital status as an enabling as well as a predisposing factor.
Previous applications of the Andersen-Newman model have neglected to consider the role of family helpers or social networks, which can substantially influence how well a person reacts and adjusts to use of services. 26 Although in their original presentation of the model Andersen and Newman discussed how enabling conditions can be measured by family resources, few experts have included such resources in the model or analyzed how these factors might influence service use. No one has studied how family resources and, in particular, marital status might influence adjustment to AL.
We conceptualize and operationalize marital status as a predisposing and enabling factor in this research. Previous research 26 supports our conceptualization suggesting that enabling characteristics of older person with dementia and their caregivers can offer resources that promote or enable service use. For example, 1 study 27 found that a spouse is often available to serve as a “helper.” Another study further suggests that caregivers of those with dementia are especially influential given the chronic care involved with this condition. 28 Finally, other researchers found that family relationships, including marital status, affected satisfaction with care in AL and expectations for aging in place in these settings. 29
Given that dementia is a chronic illness in which care needs grow progressively higher, we use functional capacity, that is, limitations in ADL and instrumental activities of daily living, to operationalize need in this study. Many previous researchers have operationalized illness level or the severity of illness by considering functional limitations as a measure of disability.21,30 Other research found that care recipients with higher levels of clinical needs (eg, functional limitations) were more likely to use services. 31
Unlike many investigators who have used a discrete measure to operationalize service use, we view dementia as a chronic illness that involves stages of care including the preillness phase, onset of the health problem/s, first involvement of a family caregiver, and concluding in the later stages that typically lead to the placement of the care recipient in an institution, such as in AL. We use a continuous variable, specifically LOS, to assess adjustment to service use. Andersen and Newman 21 originally argued that utilization should be characterized by purpose, such as considering differences among primary care, tertiary care, and custodial care, where a service provides for the personal needs of a patient without trying to treat the underlying illness condition.
Finally, although Andersen and Newman 21 recognized the need to test for interaction effects between 2 variables, few scholars have considered such interactions in the application of this model. We recognize that the underlying domains potentially interact. As a result, we include the interaction effect between marital status and functional capacity in our analysis.
Based on the Andersen and Newman model and our focus on marital status as a potential enabling factor in successful adaptation to AL settings, we hypothesized that (1) marital status will positively enhance LOS among persons with dementia and that (2) marital status will remain a significant factor associated with LOS among residents with dementia even when controlling for ADLs.
Having an improved understanding of these factors will provide allied health professionals and other providers in residential care settings the knowledge to help in maximizing LOS in AL and in enhancing quality of life for AL residents with dementia. The findings from this study will provide information related to the psychosocial needs of AL residents with dementia and offer implications for assessing the on-going needs of vulnerable AL residents.
Methods
Sampling
Only ALs considered “residential care facilities” were included in this study, thereby eliminating more restrictive long-term care residential settings (eg, skilled nursing facilities, nursing homes). The sample for the larger study consisted of AL residents (N = 218) in 3 AL settings located in Ohio. A subset of AL residents with dementia (n = 112) was utilized for this study. A dementia-related diagnosis was measured as a categorical measure of no or yes if diagnosis of AD or other dementing illness by a physician was noted on the admitting history and physical form, with 0 = no (n = 98) and 1 = yes (n = 104).
One suburban and 2 rural AL settings were the subjects of this study. Although the majority of AL settings nationally are located in metropolitan areas, there has been an interest in examining the availability of and access to long-term care services for older adults living in rural areas. 32,33 Of the AL settings included in the sample, 2 buildings were considered large (licensed for 50 residents and 100 residents) and 1 building was considered extralarge (licensed for 150 residents). Nationally, large residential care facilities (50-100 residents) serve 52% of all AL residents and extralarge facilities (more than 100 residents) serve 29% of all AL residents. 34
A purposive sample was selected because the AL settings in the study were all affiliated with one of the nation’s largest not-for-profit developer and manager of affordable senior housing and services in the United States. Furthermore, by having all of the AL settings in the sample affiliated with 1 provider, the administrative data were uniform and followed a formalized and manualized admission and charting procedure. The population for this study consisted of residents admitted to AL between the years 2006 and 2011.
Administrative records included AL residents’ demographic and health-care information as well as dates of admission and discharge. A uniform data collection instrument was created to build a case record for all of the participants in the study and was used to record information extracted from the administrative records of AL residents, including the length of time that residents resided in the AL. Data were collected from the following forms—resident admitting face sheet; physician’s history and physical nursing assessment; level of care form; and functional assessment form. Twenty-two resident charts were reabstracted and compared for evidence of agreement on major variables (95.6% agreement). Data collection took place on-site at each AL from August 3, 2011, through May 13, 2012.
Measures
Outcome measure: LOS
We use LOS as the outcome measure in this analysis because previous investigators have used LOS in AL as a proxy indicator for aging in place. 35 In addition, it has been used as an outcome variable related to personal and environmental factors associated with discharge from AL settings. 36 In this study, LOS was operationalized as the number of weeks/months/years a resident lived at the AL beginning with the date of admission and ending with the discharge date. Discharge from AL was operationalized as a resident no longer paying to hold or live in their unit. Temporary discharges to hospitals or nursing homes when the intention is to return and the room is held were not included. Hospital stays and skilled nursing facility stays did not count as discharge from the AL. Residents who had not discharged or died by the end of the study were assigned a discharge date of May 13, 2012, the date on which the data collection was completed. Residents without a discharge date were considered “censored cases” and could therefore be included in the planned analyses to calculate an estimated LOS. Discharges from the facility were measured as either discharge or death. Discharge locations were measured as acute hospital stay (other than short stay), nursing home (other than skilled nursing), independent living residence, another AL residence, back to existing home, to relative’s home, and hospice in another setting (eg, nursing home). Although LOS was measured in days, months, and years, we focused LOS in years for this analysis.
Predisposing/enabling domain: marital status
Although helping tasks or social support among family members could include adult children, cousins, and other kin, we focus on spousal caregivers in this analysis conceptualizing this relationship as both a predisposing and enabling domain similar to other research. 30 Marital status was measured by the client and/or caregiver’s report upon admission (1 = single, never married, 2 = married, 3 = separated, 4 = divorced, 5 = widowed, and 6 = other). For this analysis, marital status was recoded into categories—0 = no (n = 159) and 1 = yes (n = 43).
Need domain: functional capacity
We replicated previous studies, 30,31 using functional capacities as our need domain. As a part of the nursing assessment, the admitting nurse and/or administrator of the AL completed a standardized form (called a level of care and functional assessment tool) documenting functional status and ADL. This standardized form was included in the Clinical Administrative Manual and is utilized by staff (eg, nurse or administrator) upon every AL admission. Per activity of daily living, a score was given for level of assistance—mobility (1 = independent, 2 = 1 person assist, and 3 = 2 persons assist), eating (1 = independent, 2 = staff setup, 3 = staff assist, and 4 = staff feed), medication (1 = self-administers, 2 = occasionally requires staff assistance, and 3 = staff administers medications), bathing (1 = independent, 2 = staff assistance, and 3 = dependent), hygiene grooming (1 = independent, 2 = staff reminders/prompt, 3 = staff assistance, and 4 = total staff assistance), dressing (1 = independent, 2 = staff reminders/prompt, 3 = staff assistance, and 4 = total staff assistance), and continence (1 = resident is continent, 2 = occasional episodes of incontinence and requires staff assistance, 3 = requires staff assistance from staff to change/obtain incontinence products, and 4 = total staff assistance).
Statistical Analysis
Quantitative data were analyzed using SPSS version 22.0 software. Initially, descriptive statistics including frequency, measures of central tendency, and standard deviations were used to describe the study population. Survival analysis was selected as the method of analysis for the hypotheses as it allows the researcher to study the timing of events (ie, AL discharge) and because the outcome variable of interest is LOS (ie, time until an event occurs). 37 Cox regression was used to examine the association between marital status and LOS in AL of residents with dementia and whether ADLs were related to discharge from AL settings among married and unmarried residents with dementia. Main effects for marital status and the interaction between marital status and mobility with LOS were examined. Given that our preliminary analysis revealed that only mobility was significantly associated with LOS, we limited our test of interaction effects to this ADL. Discharge from AL was operationalized as a resident no longer paying to hold or live in their unit. Temporary discharges to hospitals or nursing homes when the intention was to return and the room was held were not included. If discharge from the AL had not occurred by the end of the study, the survival time was the interval between the time of entry into the study (ie, admission to the AL) and the date of the last data collection point.
Results
Descriptive statistics are provided in Table 1. The results from the Cox regression testing are shown in Table 2. There was a significant main effect for marital status and a significant interaction effect between marital status and mobility. Residents with dementia who were married had longer LOS than unmarried residents with dementia. The graph of the cumulative survival function in months in Figure 1 indicated a sharper discharge risk for unmarried residents with dementia. Unmarried residents with dementia and mobility impairment have higher risk for discharge (Figure 2).
Sample Description.a
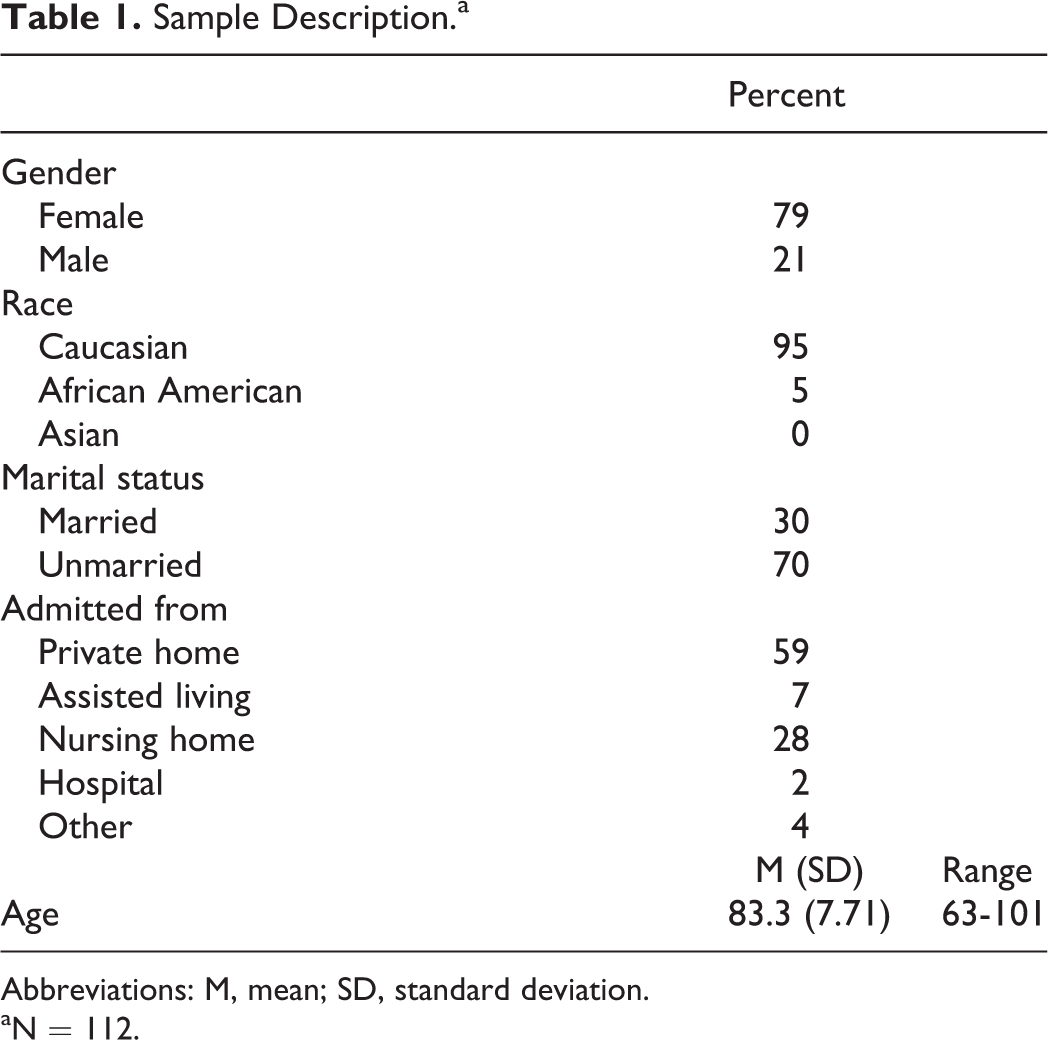
Abbreviations: M, mean; SD, standard deviation.
aN = 112.
Cox Regression Model.
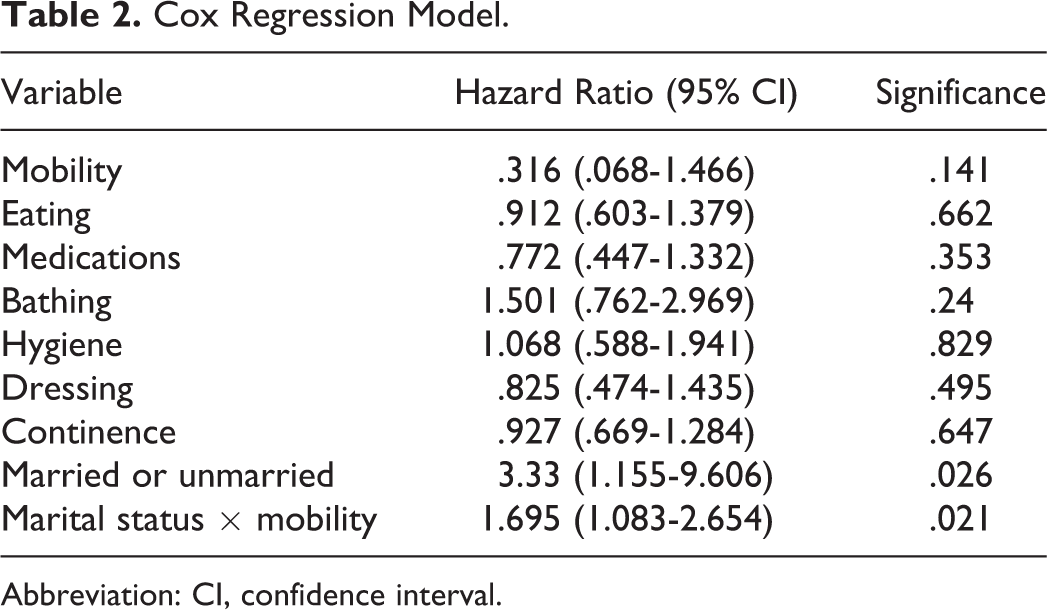
Abbreviation: CI, confidence interval.
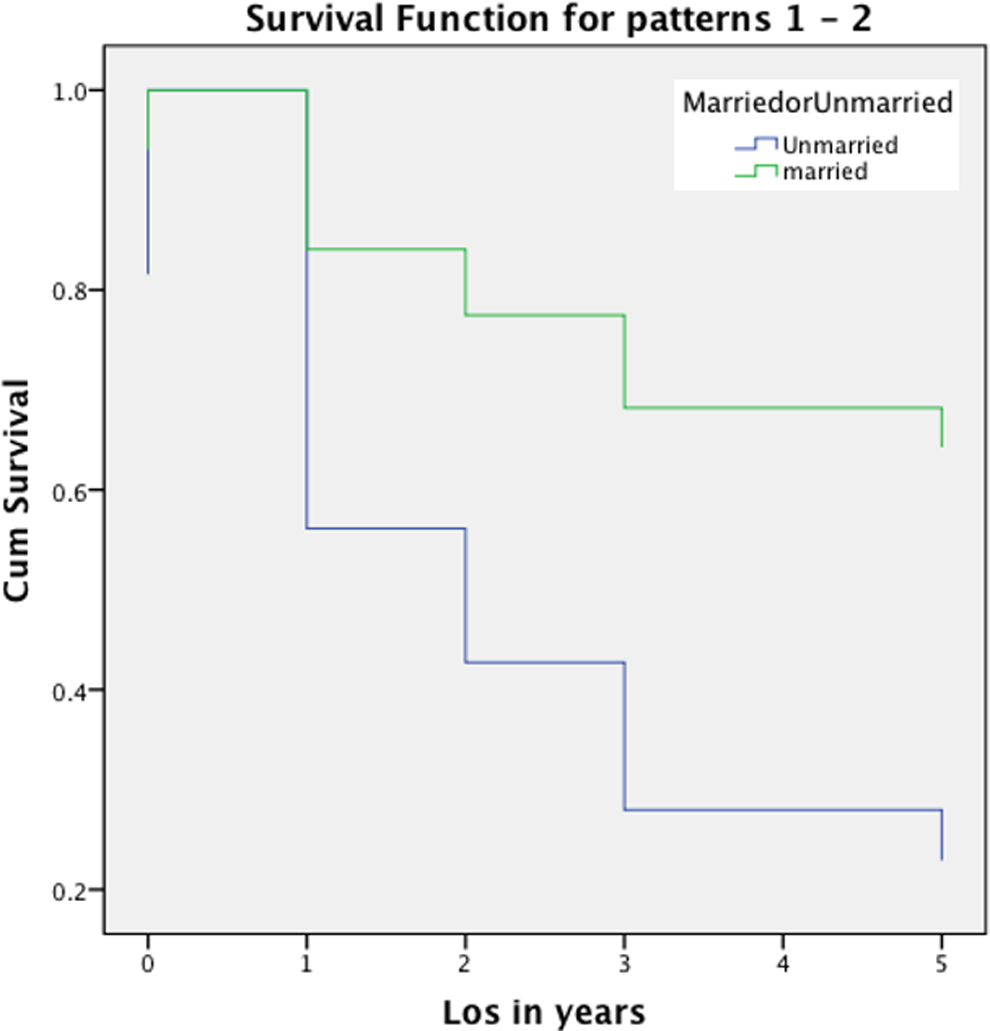
Cumulative survival function (years).
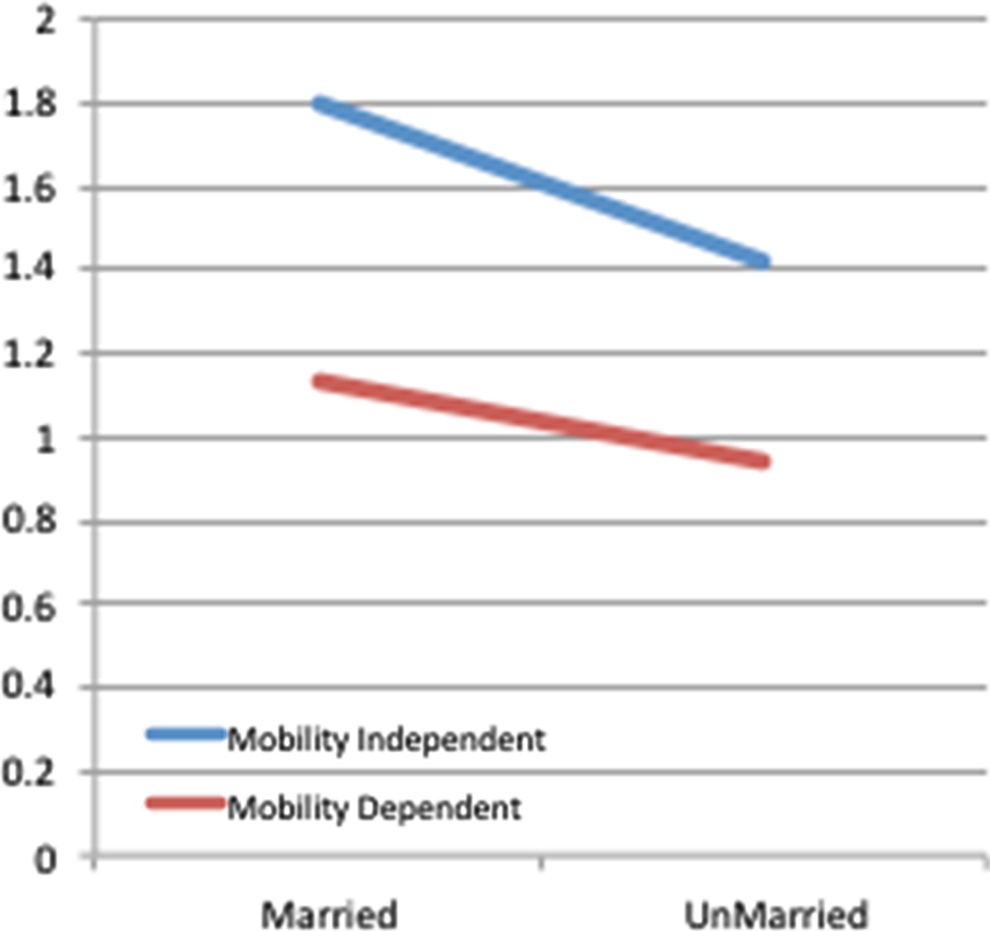
Interaction effect marital status × mobility.
Discussion
We hypothesized that marital status would increase LOS among persons with dementia in AL, and our findings supported this hypothesis. These results are consistent with previous research related to familial involvement in AL suggesting that family members play a critical role in aging in place in AL settings. 38 Married residents with dementia remain in AL longer than those who do not have the support or assistance of a spouse, suggesting that marital involvement may be integral to LOS in these settings. Research also suggests that the spouse of a person with dementia is often responsible for decision-making and increasingly assumes a caregiver role. 39 Our findings suggest that unmarried residents with dementia living in AL may be more vulnerable to nursing home discharge.
Experts have suggested that family resources and social networks might have more influence than what Andersen and Newman originally proposed. This supports previous researchers 40 who concluded that enabling factors (ie, assistance from informal supports) are more influential than need or predisposing factors. Other researchers 28 argue that support networks of individuals with AD are also a crucial factor in maintaining relations with professionals. They explain that these family helpers might directly affect a care recipient’s behaviors and indirectly influence LOS, for example, by mediating interactions with staff and other professionals employed in AL settings. In this study, marital status enhanced the duration of stay in AL.
In our second hypothesis, we proposed that marital status would remain significantly associated with LOS even when we considered need, specifically, mobility, the only activity of daily living that emerged as significant in the initial analysis. The interaction effect between LOS and mobility was statistically significant. Marital status evidently moderated the association between mobility and LOS. That is, mobility impairment for unmarried residents with dementia had shorter LOS in AL settings than mobility impairment for married residents. Previous research has shown that functional mobility limitations are higher in persons with dementia compared to cognitively healthy older adults 41 and that persons with dementia are vulnerable to mobility impairment and in turn are at greater risks for fall-related injuries and transfer to a nursing home. 42,43 Thus, the association between mobility and LOS in AL settings is more complex that experts have previously assumed.
Our findings have important theoretical and practical implications. First, they support Andersen-Newman’s 22(p4) original interest in identifying enabling resources that might “…increase the likelihood that use will take place.” Andersen 22 was especially interested in uncovering potential barriers to care that were “mutabile,” that is, could be altered to improve access and successful use of services. One original purpose implementing this model was to reveal inequitable access, when social structure, health beliefs, and enabling resources influence who gets care. 22 Furthermore, Andersen and Newman originally recommended testing for interaction effects among domains, which we completed in this study by examining the interaction effect between marital status, an enabling factor, and mobility, a need variable. Future scholars applying this model need to test for interaction effects in this model.
In addition to these conceptual contributions, we offer recommendations for practitioners and policymakers concerned with improving long-term care especially for persons with dementia based on our findings. For example, although marital status presumably is an immutable influence, practitioners and policymakers might recruit other supports or helpers, who might serve as “proxies” to marital status, which might help residents adapt better to AL. The caregiver role and decision-making of spouses may make the difference in preventing or delaying discharge or transfer from AL to higher levels of care such as a nursing home. Dementia units in AL typically offer support groups for their residents; however, some residents might become agitated, inappropriately verbose, or wander. Assisted living settings that successfully integrate family members such as spouses who might calm the resident could decrease disruptive activities overall in the AL. Although presumably paid caregivers have been trained to manage these disruptions, some AL settings do not provide dementia-specific training.12,13 Even if they have, staff-to-resident ratios sometimes preclude caregivers from providing the interventions needed to soothe a resident. If a resident continues to disrupt activities and other functions within the facility, the person might be discharged. As we previously noted, residents with dementia in AL who consistently disturb other residents or activities are more likely to be transferred to a nursing home. 7 The study findings underscore the role of family members, in particular, spouses, to provide additional supports for loved ones with dementia in AL as a way of augmenting AL services.
Connecting with adult children and extended family members may also be recommended for AL providers caring for unmarried residents. Practitioners in AL might more routinely integrate spouses who are willing into support groups or activities. Too often families are excluded from dining at the facility or from joining activities. The need for additional psychosocial support for residents has been identified as important for LOS in AL settings. 44 The results from our research confirm family involvement, and specifically, spouses are important for LOS among AL residents. Previous studies suggest family interventions such as regular visitation, oversight of care, and advocating for the resident with dementia have been cited as key to averting transfer from AL settings. 45
As the study suggests, unmarried residents may struggle with social supports that promote LOS in AL settings. Given that changing demographics indicate that future cohorts of older persons with dementia are more likely to be single, AL providers will need to find alternative helpers other than spouses if they expect residents to successfully age in place. The study findings have implications for AL providers and practitioners, as unmarried residents with dementia may be more vulnerable to discharge than their married counterparts. Findings suggest that opportunities exist to improve the AL admission process for AL residents, in particular, the assessment of the psychosocial needs and supports of unmarried persons with dementia who have higher mobility impairments. Recent research suggests that the preadmission process is especially important in terms of resident assessment. 46 Consistent with previous research, 47,48 the findings from the present study also suggest that AL providers could benefit from ancillary support such as social workers or nurse case managers who are trained to assist with the social needs of older adults and who can provide support during the transition to AL for unmarried residents with dementia.
This study has several limitations, thus findings should be interpreted cautiously. This exploratory study utilized a convenience sample of an administrative data set with data that were gathered from existing client charts. The majority of participants in this study were white, thereby limiting comparisons to diverse groups. The lower number of residents participating in the Medicaid Waiver program may also limit comparisons to older adults with lower socioeconomic status. However, the study population reflects the realities of the AL population nationally, and this is an important consideration in need of further examination that is beyond the scope of this study. Furthermore, the data collected did not incorporate time-varying measurements that could have provided more information about the dynamic aspects of factors related to LOS. In addition, our design was cross-sectional precluding the possibility of testing for causality. Finally, the data were only collected from AL providers in 1 Midwestern state, thus generalizability to other types of AL settings and other states is limited.
Despite these limitations, this study meets a gap in the literature by providing insight into LOS in AL among persons with dementia, particularly in regard to marital status. This information is critical given the rapid growth in the AL industry and the growing numbers of persons with dementia are moving to these settings. Future research is needed to understand the role of other family members, such as adult children, to consider if they, too, might increase LOS in AL and prevent premature transfer to a nursing home by joining in and helping staff especially when their loved ones are agitated. The potential benefits from such an integrated approach are numerous. Not only can family involvement potentially decrease behavioral disturbances but it might also strengthen the relationship between the spouse and the loved one in the facility. Future research should assess how this involvement from family might improve the well-being of residents, family members, and paid staff.
Future research should also examine the role of marital status and LOS in AL settings for residents with dementia and mobility impairment. Study findings suggest that there is a need for more comprehensive assessments in AL that include psychosocial care planning. Comprehensive assessments may better inform care planning and allow for the targeting of psychosocial services to the most “at risk” residents, including those who are unmarried with dementia. This study provides a first look at the role of marital status on LOS for residents with dementia in AL. Further work on outcomes in AL settings is extremely crucial considering that there is an expected increase in the numbers of older adults utilizing home and community-based services, including AL, instead of nursing homes. Finally, in order to maximize LOS in AL settings, a closer examination of the person–family–environment fit, 38 including the role of spouses, is warranted.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the John A. Hartford Doctoral Fellows Program.