
Abstract
Background:
Assisted living (AL) is a growing and operationally diverse option in our nation's long-term care system. Many consumers view AL communities as a viable option to receive needed services and age in place. However, little is known about the factors that influence residents’ ability to age in place when experiencing cognitive decline.
Objective:
To estimate the association of resident and site characteristics to length of stay, reason for leaving and destination for residents with dementia in assisted living. In particular, this study sought to assess the impact of an ‘Enhanced’ Program intended to facilitate aging in place.
Method:
Data were gathered from a retrospective evaluation of residents’ clinical records (N = 312) in five dementia-specific ALs (3 with robust enhanced programs) in the Northeastern United States.
Results:
The time to 50% survival for the full cohort (N = 312) was 20.2 months. Both age at move-in and gender were statistically significant predictors of length of stay. Sites with robust support for aging in place exhibited a statistically significant longer length of stay compared to sites with limited support. Of the residents who left or died (N = 165) nearly one quarter (24%) were able to stay until the end of their lives, while 52% moved to a nursing home, primarily because of family, financial, or medical concerns. Few residents left these settings because of behavioral problems. Conclusion: AL sites with a more robust commitment to an aging in place model and a willingness to provide palliative care demonstrated a significantly longer length of stay.
Introduction
Assisted living (AL) is an important and growing option in our nation’s long-term care system. Due to differences in state regulations and in the philosophy of care among AL providers, there is considerable variation from one AL residence to another in structure, process (eg, staffing ratio and nursing hours), 1,2 type (eg, specialized and nonspecialized care), and size of setting. 3,4 Physicians and other health care professionals, AL providers, policy makers, investors, consumers, and advocates wish to understand the impact these various processes and structures have on length of stay and ability to “age in place” in AL settings. 2,5 This desire to obtain reliable information was echoed by a national consensus conference that identified the lack of information on average length of stay and discharge destinations in AL as an important gap in knowledge. 6 Although the literature includes some estimates of how long residents stay in AL, 7 there is little data available on tenure of various subgroups of AL residents or on the factors that impact resident length of stay and destinations. Even less information is available regarding length of stay among the growing AL dementia population. 8 –11
Assisted living residents and their families typically value the ability to age in place. 12 However, a survey of providers and health care professionals suggests that the attitudes and expectations of health care professionals may be barriers to aging in place. 13 Thus, a fuller understanding of the variations among AL settings, and the factors that may contribute to the length of stay, may be helpful to both professionals and consumers. This study investigates the possible relationship of resident and site characteristics to length of stay in a subset of AL settings dedicated to serving people with dementia. The study also seeks to identify the rates of nursing home and other placement following discharge as well as to describe the reasons for discharge in these specialized settings.
Methods
Data Collection
The data were collected from a purposive sample of 312 residents living in five AL residences that specialized in dementia care. There was considerable variation among the five study sites with respect to the size and duration of their “enhanced” programs designed to allow residents to age in place (further described subsequently). All sites, regardless of the existence or duration of the enhanced program, were part of the same AL chain. This affiliation led to similarities in organizational mission and goals, hiring, and staff training procedures. Nurses received consistent training across all sites, and the organizational philosophy was geared to accommodating the needs of those with behavioral symptoms of dementia. These cross-site similarities allowed for statistical analyses that addressed the impact that site variations had on the residents’ length of stay.
There was considerable variation in characteristics among the sites. Site #1 had, at its height, 44 beds, of which 16 were enhanced, although by the time of data collection its size was reduced, including a reduction to 6 beds in its enhanced Special Care Unit. With the greatest experience in enhanced care, this site offered 2-person assistance with transferring and complete feeding assistance. Several residents at this site utilized hospice. The next largest of the enhanced units in this study (site 2) was also in a Special Care Unit that had 44 beds. Site #2’s 12-bed enhanced wing was added five years before the data were collected. Site #3 was the only one in the study that never had an enhanced wing. It was comprised of 30 beds and was on a campus with an affiliated nursing home. Site #4 was the smallest site in the study, with a total of 28 beds and only four were converted to use for an enhanced program less than two years before data were collected. Site #5 was in an upscale urban area. Although it had a 6-bed enhanced unit, residents were financially able to afford private duty help and operationally it had more access to nursing through an on-site home health agency, allowing those with a higher level of need to remain even if the enhanced program did not have an available bed.
The data for the study were obtained by retrospective chart review, performed by the nursing director at each of the sites. Data were collected on both enhanced and regular Special Care Unit residents who were living in the site at the time of data collection as well as any other individuals who had resided there at any time over the past five years. For each resident, the following items were recorded: gender, resident's year of birth, date of arrival, date moved out (if applicable), and move-out reason, and destination. All data were deidentified prior to being entered into the research database. The research protocol was approved by the Chesapeake and University of Maryland, Baltimore County Institutional Review Boards.
A total of 373 chart review summaries from six sites were collected by the research team. Of the 373 summaries, 38 were excluded from further analysis: two had missing data while 36 were only short-term respite or day clients. In addition, all data from the sixth site (23 patients) in the original sample were excluded from the analyses, since this relatively new facility had only three residents with an observed discharge. In total, 61 case summaries from the original sample were excluded in these analyses (n = 312).
Description of the Intervention: The Enhanced Program
The enhanced program was designed to operate within a Special Care Unit to serve those with end-stage dementia or with dementia combined with other diagnoses that require a higher level of care than is normally offered in AL settings. A descriptive pilot study 14 –16 was completed in these settings to describe the enhanced units and categorize the extent of the intervention program. It was found that enhanced units offered a staff ratio of approximately one direct care staff person for every three residents as well as on-site nursing 16 hours per day. Staff members were hired who had both the desire to work with and the strength to lift the residents in the enhanced unit. They received additional training, including proper body mechanics for lifting and education regarding end-stage dementia and the dying process. Staff members in the enhanced program also received bereavement counseling from a hospice provider. Staff also received unique training on topics such as appropriate activities programming and how to recognize signs of discomfort/nonverbal communication to minimize challenging behaviors. The direct care staff members on the enhanced unit had higher pay grades than that of the staff members in the regular dementia unit. Residents in the program paid approximately US$1000 more per month than in the nonenhanced program in the same site or about 90% of the local skilled nursing home private pay rate.
The pilot study found that enhanced residents had from 0 to 7 (mean 2.44) diagnoses in addition to their dementia. The most common nondementia diagnoses were heart disease (57%) and respiratory diseases (31%). Eighteen percent had cancer. Patients were taking anywhere from 2 to 16 medications, with an average of 8.5 different medications. Of these 36 enhanced residents, 27 had medications crushed and 19 had one or more as needed (PRN) medications ordered and given with the nurses' not the residents’ judgments.
Enhanced program residents used hospice and end-of-life services at higher rates, a similar proportion used nurses from an outside home health agency or occupational therapy/physical therapy services on site, and some received x-rays from a mobile machine at some point during their stay. The majority of enhanced residents who used end-of-life services also used a wheelchair at some point during their stay, slept in hospital beds or used bed and chair pads, and were on positioning programs to avoid skin breakdown. Many of the residents in the enhanced program used a commode and had access to other devices or special medical equipment to better accommodate their health care needs. At one site, a Hoyer Lift was installed and was used with some success for one, especially heavy resident. Half of the residents in the enhanced program were on formal toileting programs, while most were on a formal feeding program and received mechanically altered foods.
These findings from the pilot study were used to delineate and distinguish between “robust” and “limited” enhanced units. The five sites in the study offered varying levels of enhanced services. Of the five sites in the current study, three had robust enhanced units (sites 1, 2, and 5). To be classified as having a “robust” enhanced program, the site was required to (1) have at least six residents receiving enhanced services; (2) use hospice/palliative care or have more nursing staff with advanced clinical expertise (eg, registered nurses or nurse practitioners); (3) an established commitment to the enhanced program (in place for at least three years); and (4) resident to nursing staff ratio lower than 1:4. Of the five sites, two had limited or no enhanced support (sites 3 and 4). These sites did not meet all of the criteria for having an established, robust program to focus on the needs of those with end-stage dementia or dementia with other serious health problems. The primary objective of this study was to examine the comparative impact of 2 levels of dementia-specific services in one AL organization: (1) robust enhanced programs and (2) Special Care Units with limited or no enhanced services.
Statistical Methods
Hypothesis tests for continuous variables across sites were conducted using one-way analysis of variance (ANOVA). Fisher exact test was used for categorical variables. Because many patients were still in residence at the time of data harvesting, the complete time of residence was not observable but instead censored. To analyze censored time-to-event data, the Kaplan-Meier estimator 17 was used to obtain unadjusted estimates for time to 50% remainder in the facilities and the log-rank test 18 was used to test hypotheses of differences with such data. The Cox proportional hazards regression model 19 was used to conduct hypothesis tests while adjusting for potential confounders. All tests of hypotheses were 2 sided and conducted at an α = .05 significance level, and analyses were conducted using Stata/SE 10.0 (College Station, Texas).
Results
Of the study patients, 47% (N = 147) were still living in one of the study sites while 53% (N = 165) had left or died as of the time of the study. Of the study sample, 70% (N = 218) were female. Age at move in was distributed as follows: 85 (27%) participants younger than 80 years old; 188 (60%) were aged 80 to 90; and 39 (13%) were older than 90. For the full cohort of 312 patients, the time to 50% remaining in the facility was 20.2 months while for those who died or left the average length of stay was 8.3 months.
Resident Factors Associated With Length of Stay
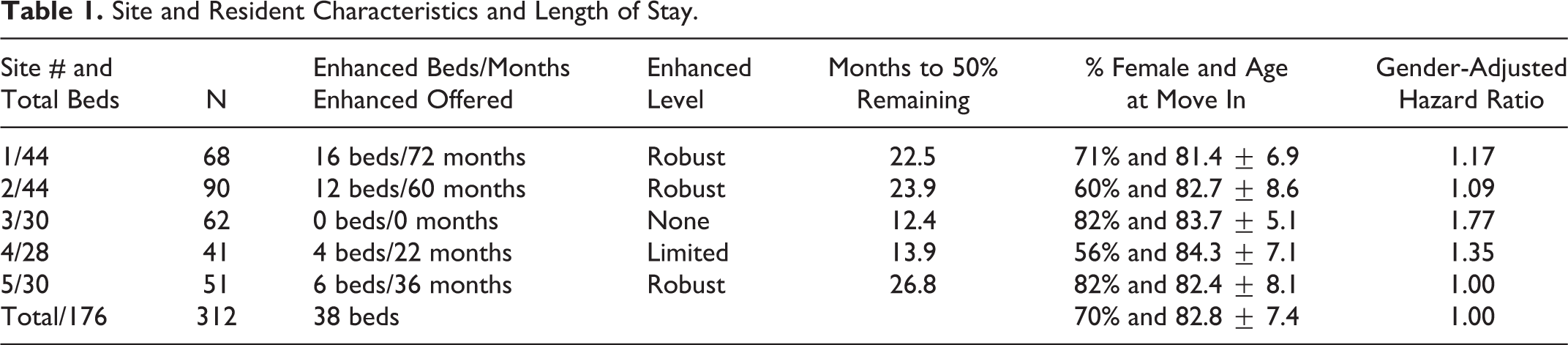
Age at move in did not vary significantly across study sites (1-way ANOVA: F = 1.29, df = 4, P = .27). The time to 50% remainder for residents younger than 80 years old (N = 85) was 22.7 months, for residents in their 80s was 21.5 months, while, as might be expected, people who moved to AL at ages more than 90s (N = 39) had the shortest stays, with an average time of remainder of only 11.6 months. Time to 50% remainder for women was 26.3 months while for men it was 11.0 months, and this difference was highly statistically significant (log-rank test: chi square [χ2] = 19.6, df = 1, P < .001; Table 1).
Site and Resident Characteristics and Length of Stay.
Site Factors Associated With Length of Stay
There was a statistically significant difference in the time to 50% remainder between sites with robust support and sites with limited or no enhanced support (22.7 vs 14.8 months, respectively; log-rank test, χ2 = 4.77, df = 1, P = .03). This was still statistically significant after adjusting for age at move in and gender, using a Cox proportional hazards regression model (P = .04; Figure 1).
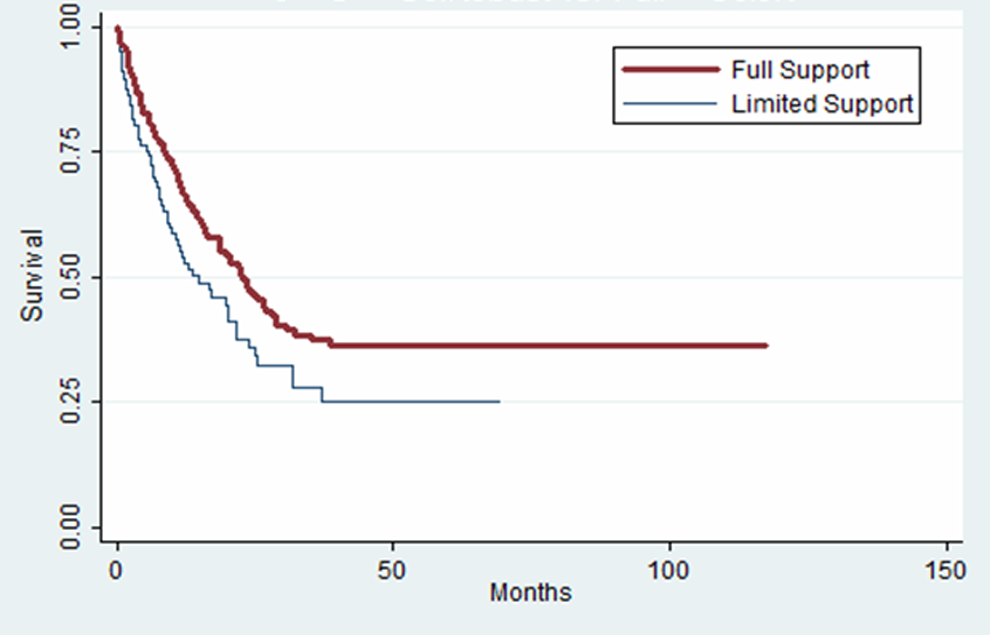
Robust versus limited support for aging in place. Kaplan-Meier graph displaying curve for length of stay for residents remaining in full support units versus limited support units. Vertical axis represents percentage of original residents remaining in assisted living.
Reasons for Leaving and Destinations of Residents Who Left
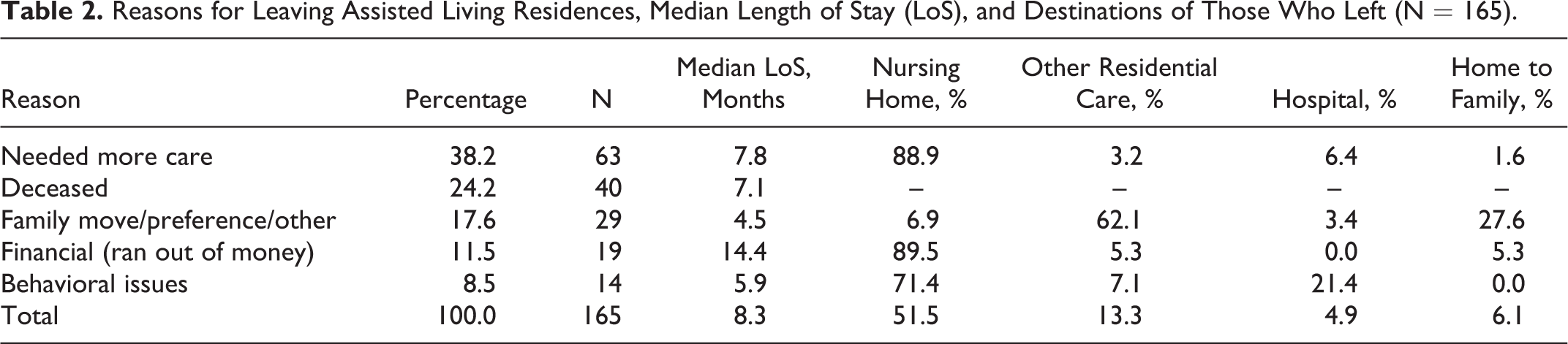
Among the 165 patients who had ended their residency at the time of data harvesting, the primary reason for termination was the need for more care (38%), followed by death (24%), family-related issues (18%), money problems (12%), and finally behavioral issues (8%). Fifty-two percent of these residents went to a nursing home. However, this percentage varied considerably depending on the reason for leaving: a nursing home was the destination for 89% of patients who needed more care and similarly for 89% of residents who left because of money problems, but for residents with behavioral issues, 71% went to a nursing home while for those who left for family or other reasons only 7% went to a nursing home. Residents who left because of financial issues had the longest length of stay (14.4 months), followed by those who needed more care (7.8 months), those who had behavioral issues (5.9 months), and those who had family problems (4.5 months; Table 2).
Reasons for Leaving Assisted Living Residences, Median Length of Stay (LoS), and Destinations of Those Who Left (N = 165).
Discussion
This is a nonrandomized retrospective study based on the chart review of clinical information. Thus, causal interpretations of observed associations are not possible. Other variables, such as differences in functional and cognitive status at time of move in and number of residents on antipsychotic medication for behavioral problems, were not collected and thus could not be controlled for. Further studies investigating the impact of enhanced support on length of stay for people with dementia living in AL should collect data on cognitive status, functional ability, use of antipsychotic and pain medication, and other potentially influential factors. Considering these resident characteristics and additional health care services will help delineate the combination of services that can facilitate aging in place for residents of varying levels of functioning. Further, two of the study authors were affiliated with the study sites at the time of data collection, creating the possibility of unconscious bias in interpretation.
Many of the results were consistent with preconceived notions regarding length of stay. For example, gender was a very strong predictor of length of stay, with women staying over twice as long as men. Age was also a strong predictor of length of stay with an indication of a threshold effect at age 90: residents who moved in after the age of 90 exhibited a sharp decrease (11.6 months). However, perhaps surprisingly, there was little difference in length of stay between residents who were younger than 80 years of age at move in (22.7 months) versus those who were between 80 and 90 years of age at move in (21.5 months). Most encouragingly, those who lived in a unit that had robust support for aging in place did in fact have longer lengths of stay (22.7 months) than those who lived in units with more limited end-of-life support (14.8 months).
A substantial proportion (24%) of the residents in this study who left were able to remain at the dementia AL site until they died. Most of the rest moved to nursing homes, most often because they needed more medical care. Despite the fears of referral sources and advocates, a relatively small proportion of residents (12%) left for financial reasons, and those who did had a considerably longer length of stay (14.4 months) than those who left for other reasons.
Conclusions
In planning for their long-term care needs, people with dementia and their families can anticipate that women will remain in AL settings longer than men, and similarly those younger than age 90 will remain in AL settings longer than those older than 90. More importantly, in planning for a move to an AL setting, people with dementia and their families should take into account the commitment of the AL provider to serve those with end-stage dementia, as, at least in this study, those sites with a more robust commitment to an aging in place model demonstrated a significantly longer length of stay. Consumers should be aware there is wide variation and the extent of services that an AL organization can and will provide to their residents. This variation is in part due to the AL regulatory differences in each state as well as differences in organizational policies related to dementia care, end-of-life services, behavioral issues, assistance with transfer, and incontinence care. This study examined an enhanced program developed and run within one AL organization, and all of the focal sites were located in two states. In many states, the enhanced care described in this study may violate state regulations. As such, the extent to which an AL organization will go to retain their residents will vary based on a number of factors. Consumers should do independent research on the services and care that can be provided by AL settings in the state and ask each provider questions about their specific organizational policies regarding discharge criteria.
Footnotes
Acknowledgments
We wish to thank Calixte Ahokpossi, PhD, for his central role in the collection and analysis of the data. There were also many staff members in the study sites who contributed their time and expertise during the data collection process. We are indebted to all these devoted individuals.
Authors’ Note
This study was undertaken with encouragement from John Hennen, PhD, MPH, when he served as Chief of Biostatistics at McLean Hospital, Harvard University Medical School. John died of a heart attack in 2005, as we were collecting data. The first two authors (Joan Hyde and Rosa Perez) were affiliated with the organization from which the data were collected.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.