
Abstract
Light therapy is applied to older people with dementia as a treatment to reset the biological clock, to improve the cognitive functioning, and to reduce behavioral symptoms. Although the methodological quality of light therapy studies is essential, many aspects concerning the description of the lighting applied are missing. This study reviewed light therapy studies concerning the effects on people with dementia as a way to check the methodological quality of the description of light from a light engineering perspective. Twelve studies meeting the inclusion criteria were chosen for further analysis. Each study was scored on a list of aspects relevant to a proper description of lighting aspects. The overview demonstrates that the overall quality of the methodologies is poor. The studies describe the lighting insufficiently and not in the correct metrics. The robustness of light therapy studies can be improved by involving a light engineer or specialist.
Introduction
Light therapy is studied and used as a nonpharmacological treatment of a variety of health-related problems, such as the therapy for a variety of skin conditions, 1 circadian rhythm-related problems, 2 -5 and mental conditions. 6,7 It can be administrated in various ways, from exposure to daylight to exposure of light emitted from wall, ceiling, or table-mounted devices and luminaires. 8 -11 A specific niche of light therapy focuses on older people with dementia as a target group. This type of light therapy aims to improve the cognitive behavior and to enhance the extent of behavioral symptoms by exposure to (high) levels of (ambient) light aiming to reset a free-running biological clock. Studies on any form of light therapy on (older) people with dementia 12 -17 found a number of short- and long-term effects: a more stable sleep–wake rhythm, improvement in restless and agitated behavior, and beneficial effects on the cognitive functioning.
The health-related effects of light therapy that are associated with dementia have been reviewed by Forbes et al 18,19 in a Cochrane systematic review. These reviews concern the effects of interventions for prevention, treatment, and rehabilitation and assess the accuracy of a diagnostic test for a given condition in a specific patient group and setting. The review by Forbes et al 18,19 included all relevant, randomized clinical trials in which any form of light therapy or treatment was compared to a control group for the effect on managing cognition, sleep, function, behavioral, or psychiatric disturbances (as well as changes in institutionalization rates or cost of care) in people with dementia of any type and degree of severity. The studies included were randomized controlled trials (RCTs) in which the participants were diagnosed with dementia (Alzheimer’s disease, dementia with Lewy bodies, vascular dementia, or dementia due to another cause). One group received a type of light therapy for any intensity and duration for the management of cognitive, sleep, functional, behavioral, or psychiatric disturbances associated with dementia. Results were compared to a control group. The conclusions drawn by Forbes et al 18,19 were “[T]here is insufficient evidence to assess the value of light therapy for people with dementia. Most of the available studies are not of high methodological quality and further research is required” (Forbes et al 18(p2)) and “There is insufficient evidence to recommend the use of bright light therapy in dementia. (Forbes et al 19(p2))” The studies were basically reviewed on their methodological quality from a medical point of view. In addition, van der Ploeg and O’Connor 20 reviewed the studies by Forbes et al and proposed guidelines for research methods in future studies. Again, these recommendations were related to study design, participant selection, light delivery modalities, and outcome measures, not on the more technical aspects of light and lighting. Van der Ploeg and O’Connor 20 anticipated that the quality of this evidence will be improved if researchers refine their study methods and adopt a more uniform approach.
For future research and application of light as a therapeutic means, the methodological quality of effect studies is of high importance. Originally, light was predominantly studied for the visual aspects. Therefore, the nomenclature as we know is directly related to these aspects of light. We use radiometry as the measurement of optical radiation, which is electromagnetic radiation within the frequency range between 3 × 1011 Hz and 3 × 1016 Hz (0.01-1000 μm). Photometry is the science of measuring radiation in units that are weighted against the visual sensitivity of humans. It is a quantitative science based on a statistical model of the human visual response to light under carefully controlled conditions. The quantity “illuminance, E[lx],” for example, is the human vision-related quantity of the irradiance [W/m2]. This only takes the part of the electromagnetic spectrum into account ranging between 380 and 780 nm with a peak at 555 nm. Illuminance, or the areal density of the luminous flux, is expressed in the metric system in lumens per square meter or lux. When considering a nonimage-forming aspect such as melatonin suppression, the most effective wavelength is approximately 460 nm, 3,21,22 which is more in the bluish part of the spectrum. Since most research points out that for specific health-related effects, the exposure duration, timing, light flux density, and the wavelength are of influence, such a visual-related quantity is not appropriate for describing non-image forming effects. 4 Bellia et al 23 suggested a theoretical approach to enable to implement both effects in indoor lighting design. Analogue to the expressions “luminous efficiency in the visible field, V(λ),” the need for a “circadian efficiency in the visible field C(λ)” is obvious. The need to describe light sources in terms of the visible aspects in the 2 dominant quantities, luminous flux (Φ) and correlated color temperature (Tcp), are missing the sensitivity to describe non-image forming aspects. In both quantities, the spectral distribution, the duration and timing aspects are not incorporated. This has also been acknowledged by a group of researchers within this specific domain of light-related effects on humans. 24
Van Hoof et al 9 pointed to the flaws in the methodological approaches in light therapy studies from the point of view of building services engineers and building physicists. They provided an overview of errors and shortcomings made in studies performed by researchers with a (bio) medical, psychological, or otherwise nonengineering background in terms of the description of light systems and the light exposure. These types of shortcomings are not considered in the latest appraisal of the methodological quality of studies by Forbes et al, 19 although concluded was that further research is required in order to draw final conclusions on the effects of light therapy for the treatment of people with dementia. Within the domain of medical studies, Cochrane systematic reviews represent the highest degree of evidence. To practitioners and physicians, the quality of evidence is very important, but the focus can be limited. Anything but an RCT cannot be appreciated as a proper study, completely overlooking other quality indicators. A limited understanding of engineering and physics may lead to a narrow horizon, in which the RCT character of a study becomes more important than a sound methodology from an engineering perspective.
There are two parallels that can be drawn between the methodological weakness in light therapy and medicine using the following 2 examples: When engaging in pharmacological research and testing new drugs on human beings, it is of the utmost importance to know the exact substance and the exact doses in which this substance is administered to a research participant or patient. In the case of light therapy, people are being exposed to a type of radiation (light), which can be compared to administering pills that are either a placebo or contain ibuprofen, paracetamol, or aspirin in unknown doses. Light therapy without an adequate description of the equipment and characteristics of the exposure is like doing pharmacological research of which the methodology section only states “we tested a pill.” A similar parallel can be drawn to radiotherapy in oncology. When patients, for instance, a woman with mamma carcinoma, receive treatment, the physician involved knows exactly the dose and the properties of the radiation, including the source of the radiation and the type of particles. Light therapy without describing the source of light and the spectral distribution and wavelength of light can be compared to uncontrolled radiotherapy in terms of methodological error, although the negative side effects of improper radiotherapy are potentially more severe.
Therefore, this study critically reappraises the studies that were included by the Cochrane systematic review by Forbes et al 19 in terms of the methodological quality from the light engineering perspective. The goal is to point the light therapy community to the need for sound and robust methodological approaches in light therapy research from a medical, statistical, and engineering perspective.
Methodology
The 13 studies included in the review by Forbes et al
19
were considered for a secondary analysis of the methodological quality from an engineering perspective. Of these studies, 12 were included.
25
-36
The 13th study by Nowak
37
was left out because it concerned a dissertation that was not publically available. The important methodological elements that are adopted from van Hoof et al
9
are: the description of light measurements, the description of the lighting system, the description of the building/room, and the exposure to other light sources, most likely to be daylight.
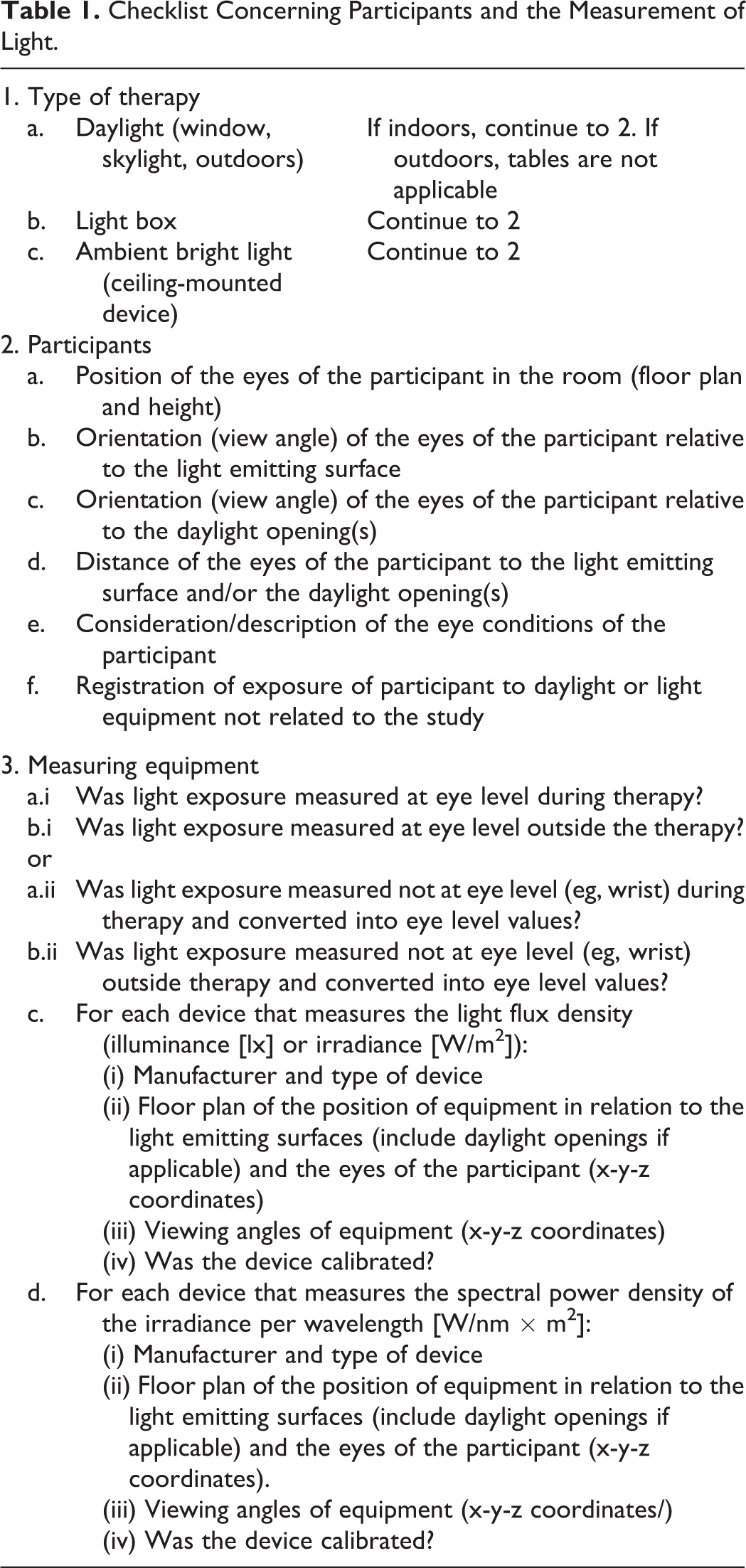
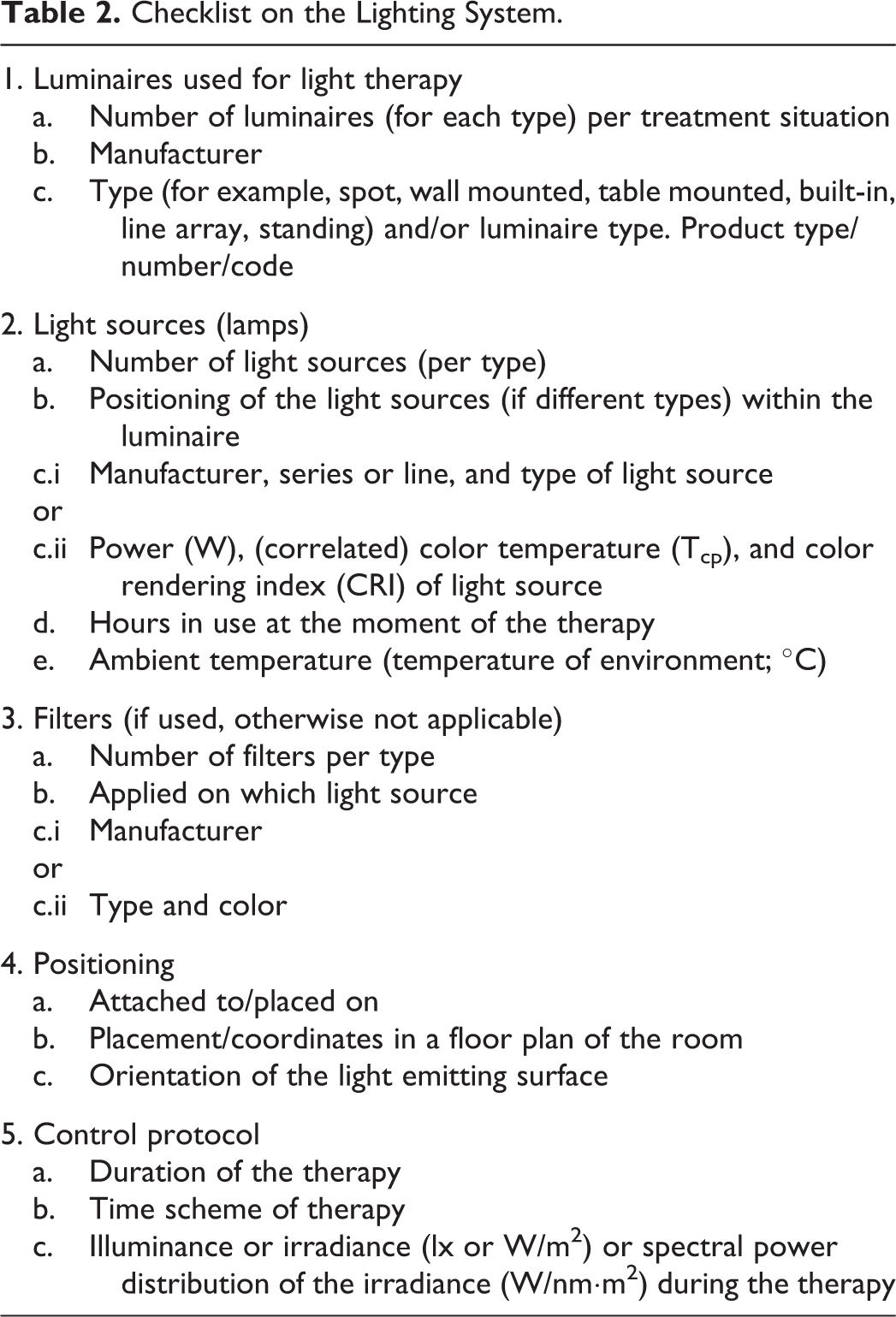
Based on these elements, a protocol was developed to be used as a checklist on what to describe and if necessary adjust the used research methodology. These checklists can be found in Tables 1 to 3.
Checklist Concerning Participants and the Measurement of Light.
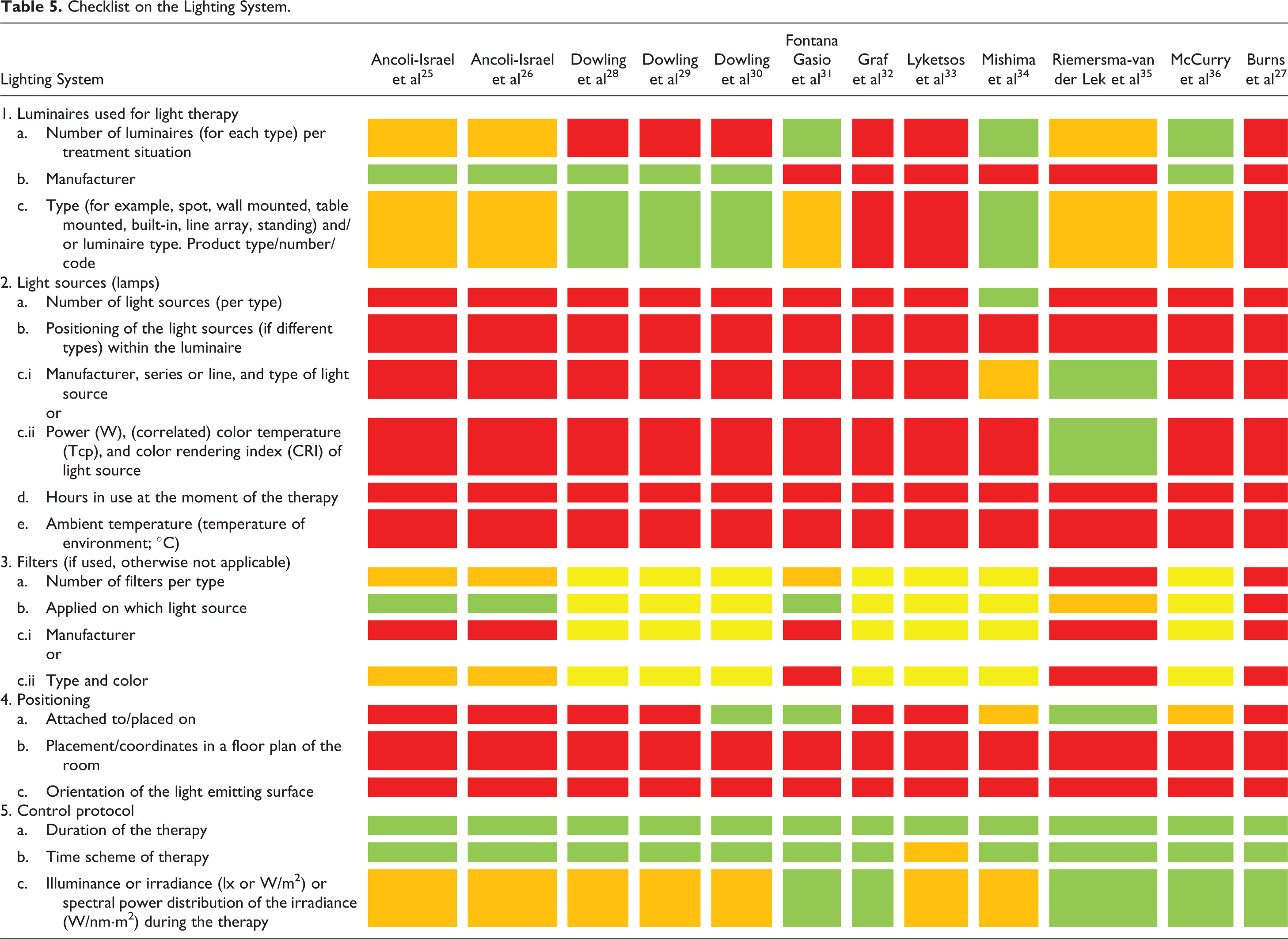
Checklist on the Lighting System.
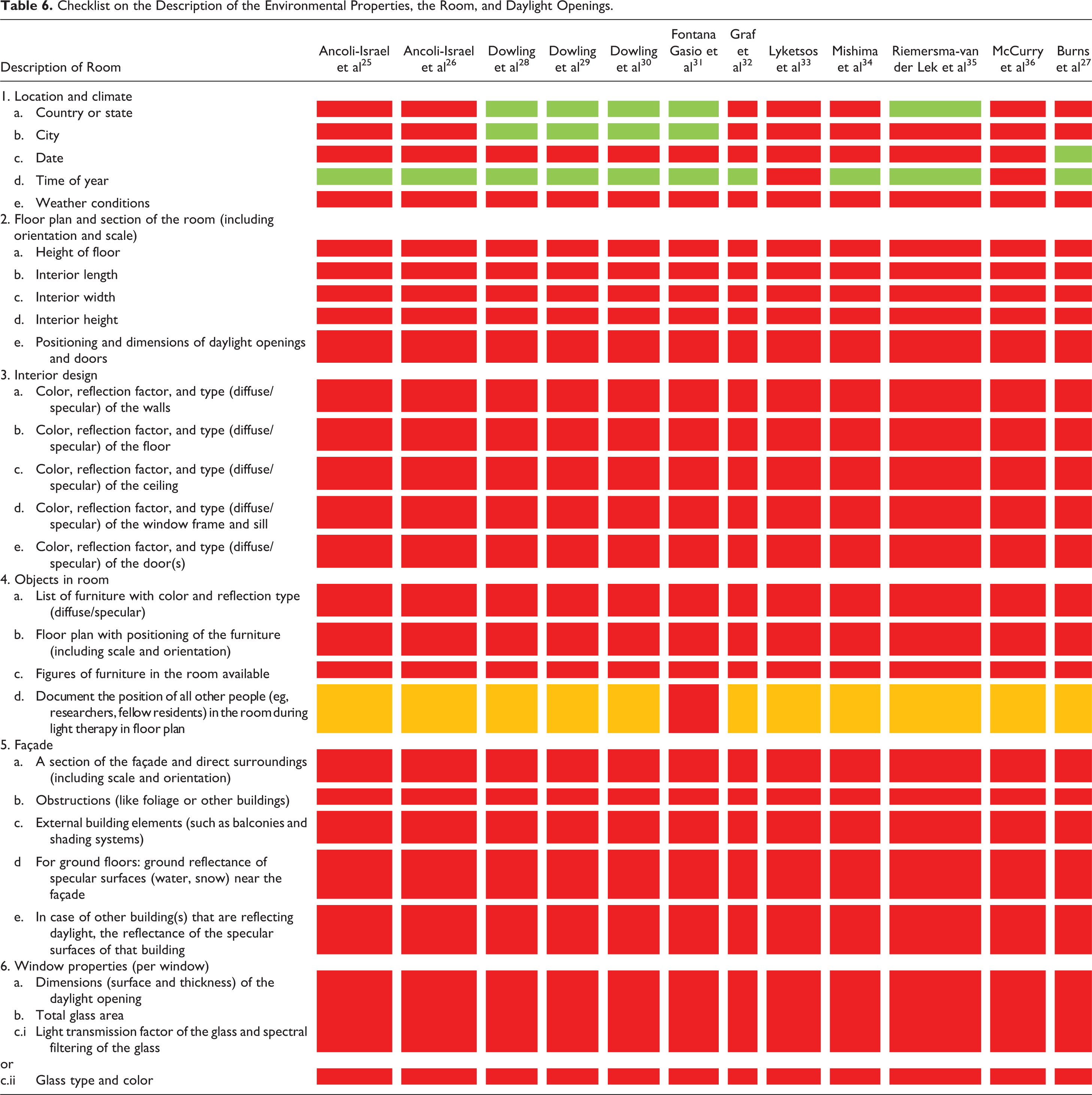
Checklist on the Description of the Environmental Properties, the Room, and Daylight Openings.
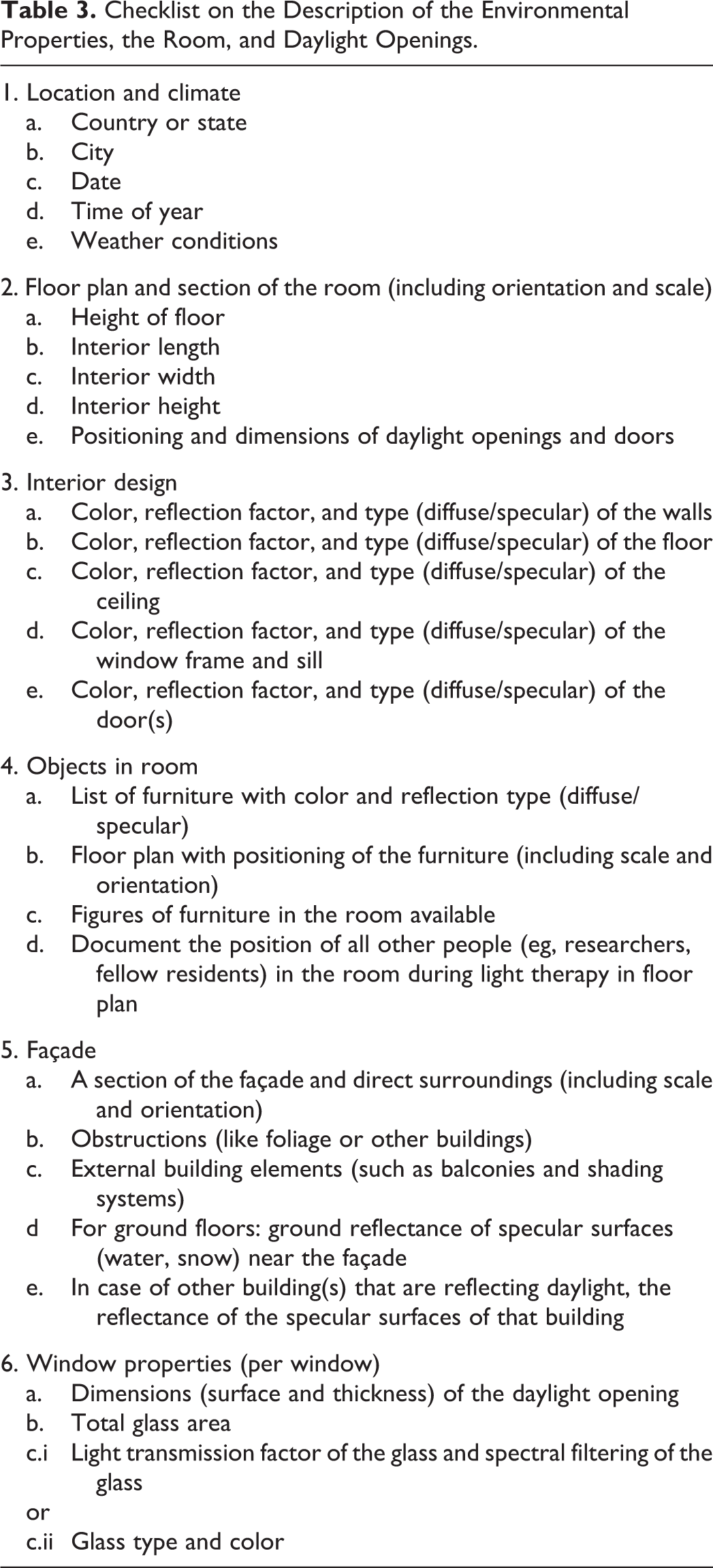
The first step in the review process was to check for a relevant description of the active substance, the light or irradiance characteristics, and whether these were monitored on the eye level and on a continuous basis. If these descriptions were not of a sufficient quality, a second analysis was made of aspects, which might be an indicator of the above-mentioned aspects. These indicators included a description of the used lighting system, the influence of the effective exposure of the therapeutic room or environment, and finally the influence of light/irradiance exposure other than coming from the therapeutic light source. The most likely and the most influential light source for expected side effects is daylight. In general, when going outdoors, the light values exceed the indoor values by at least 10 times.
The process of evaluation was the following: first, the papers were read by the 4 authors (MPJA, MBCA, AD, and JvH.) in their entirety and thereafter read again and analyzed by scoring the appraisal protocol described in Tables 1 to 3. In the second stage of the analysis, the scoring lists of the authors were compared and consensus had to be reached on every entry in the appraisal protocol for each article. This was done on April 2, 2015, and articles were discussed in a random order.
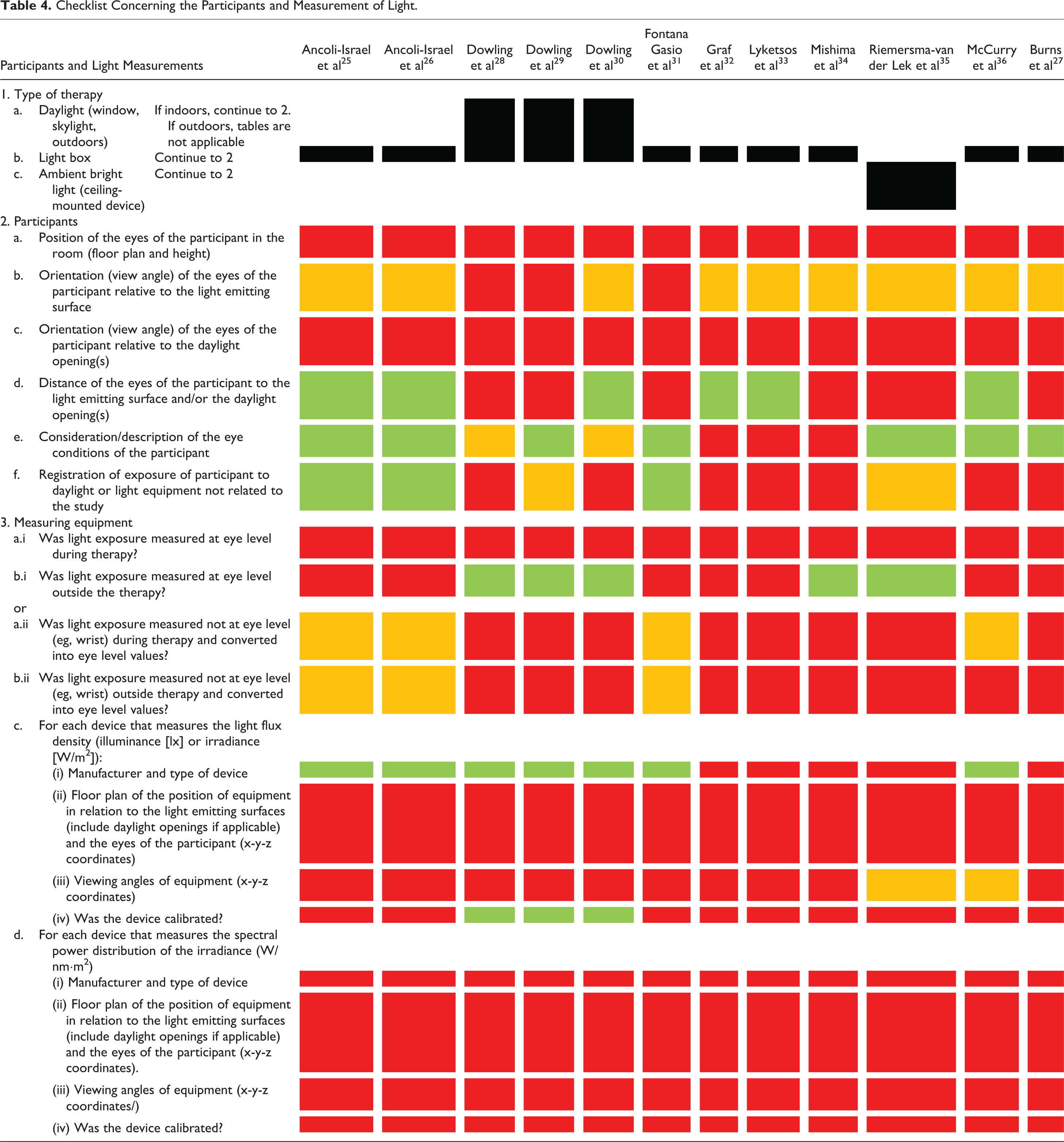
The tables were filled out for each study as following: green field: description is correct and complete; orange field: description given but incomplete; red field: not mentioned in the paper; and yellow field: not applicable.
The studies receive a total score for each element. A green score counts for 1 point, orange fields for 0.5 points, and red as 0 points. The yellow fields are counted as 0 and deducted from the maximum possible score. This way, the topics that are not applicable are not included in the total score. In some categories, 2 elements/methods are possible and indicated by “or.” Therefore, it can score for only 1 point maximum. Finally, all scores are rated and added, resulting in a maximum reachable score per paper of 1.
Results
Tables 4 to 6 show the results of the analyses of the participants and light measurements, lighting system, and the environment.
Checklist Concerning the Participants and Measurement of Light.
Checklist on the Lighting System.
Checklist on the Description of the Environmental Properties, the Room, and Daylight Openings.
The checklist concerning the measurement of light (Table 4) shows that the majority of studies were conducted using light boxes, in particular, table-mounted devices. The best scores were obtained for the description of the distance to the light source and the description of the health condition of the eyes. In 6 of the 12 studies, the distance of the participant to the light box is mentioned. In the studies of Dowling et al, 28 -30 daylight was also considered to be therapeutic. In the study of Riemersma-van der Lek et al, 35 ambient bright light is used, not a bright light box therapy. Since the illuminance was measured on the eyes, the distance to the light source is less relevant. However, due to the fact that it was not measured continuously, it still scored negatively. In none of the studies, the height of the participants’ eyes is mentioned.
Unfortunately, the exposure to light sources other than the therapeutic one is only described in both studies by Ancoli-Israel et al 25,26 and the study by Fontana Gasio et al, 31 since they monitored the light exposure continuously. It would have scored positively if it was monitored on a position close to the eye and not via a wrist-worn actigraph. Daylight is a major contributor to light exposure, and failing to describe this exposure is a major flaw in any study. In analogy, it is like being administered a specific active substance, a specific drug during a test, but allowing to take an unlimited and unregistered number of these pills.
The description of the measuring equipment is poor. In some studies, only the brand of the measuring device is given. Even the best quality of measuring equipment can have an error of 5%. In only 3 studies, calibration is mentioned, which is an essential step in the use of measuring equipment. It is not mentioned whether these instruments were actually used in a proper way, for instance, if sensors were blocked by the researchers or not. In the study by Ancoli-Israel et al, 26(p197) it is written that “Research staff, using hand-held photometers, confirmed that light levels at the eye were >2,500 lux each time patients changed position or activity.” It is not described whether these researchers actually shielded off the ambient light or light being emitted from the light box. Almost all studies included in this review mentioned the presence of other people but did not discuss whether these people prevented light from entering sensors.
The spectral distribution of the light is not measured or described at all, although it may be deduced from the type of luminaire/light source used, such as in the study by Riemersma-van der Lek et al 35 who described the tubes. Ancoli-Israel et al 25(pp25-26) described the use of “cool-white fluorescent, non-UV full spectrum light bulbs,” which does not adequately describe the system, as the readers are left puzzled about the actual spectrum. Fontana Gasio et al 31(p209) failed to describe the wavelength of the red light nor the type of light source used in the study and mentioned no more than “red light.” Dowling et al 28(p740) go one step further when the authors compared “morning bright light exposure to usual room light exposure” and used the words “usual light conditions” without adequately describing these usual conditions. The study by Mishima et al 34(p694) described the times that lights were turned on and off and was one of the few studies that described the overall lighting system used in the experiment.
In several studies, participants were allowed to engage in activities during therapy. For example, Ancoli-Israel et al 25(p26),25(p197) defined in their studies: “Patients could eat, converse, play cards, watch television, and so on during treatment sessions as long as they remained facing the light box.” In about half of the studies, the care professionals involved or the researchers made sure that the participants remained facing the light box. In the studies by Fontana Gasio et al, 31 Mishima et al, 34 and Riemersma-van der Lek et al, 35 this type of fixation was not applicable, since the light boxes were mounted onto the ceiling or onto a standard. The studies of Dowling et al 28 -30 and Riemersma-van der Lek et al 35 used ambient light as therapy. Dowling et al 28 -30 described the ambient light levels by the control group as “usual” indoor light. The other studies did not mention the ambient light levels of the room.
Overall, luminaires and the duration of the bright light therapy are addressed by the majority of studies (Table 5). The light sources are hardly described, even though a detailed description is, as already mentioned previously, as essential as mentioning the substance in pharmaceutical research. Burns et al 27(p712) described a “randomized controlled trial of full spectrum BLT < bright light therapy > versus normal light for agitation in dementia.” The authors failed to describe the full-spectrum lighting system and the “normal” light conditions.
Table 6 shows that researchers pay no attention to the environmental conditions in which their participants stay and undergo the light therapy. The daylight opening design and its access, reflective properties of the built environment, and furniture present are totally not addressed, even though all influence the light exposure.
Generally, there is an overall lack of understanding of nomenclature used for light characteristics. Lyketsos et al 33(p521) speak of “[b]right light therapy [that] was administered for 1 hour every morning using a 10,000 lux full spectrum lamp at 3 feet.” Apart from the minor flaw of using feet as a unit of distance, a lighting system emits a luminous flux, expressed in lumens, and the intensity of the light source is expressed in candelas. Moreover, Dowling et al 30(p242) speak of a median light exposure for the treatment groups of “6204 ± 2668 lux.” This is much too specific to have any practical significance, especially when a deviation of 5% on the measured values is acceptable for the highest quality of light-measuring equipment. It is highly recommended to journal editors to have someone with a (light)technical background on the reviewing panel when light therapy studies are submitted to prevent papers from being accepted that contain such major errors.
Table 7 shows the scores of each study on the 3 different appraisal score forms for methodological quality. If all issues were addressed correctly, an indicative total score of 1.0 could be obtained. Unfortunately, the overall scores are very low, ranging from 0.1 for the study by Graf et al, 32 Lyketsos et al, 33 and Burns et al 27 to 0.2 for the other studies.
Indicative Results of the Studies Reappraised for Their Methodological Quality From an Engineering Perspective.

Discussion, Conclusions, and Further Actions
The methodological quality of light therapy studies not only require attention from a research method point of view but even more from an engineering perspective. This pleads for a multidisciplinary approach.
Strengths and Limitations
This study is the first to systematically score the methodological quality of light therapy studies that passed the internationally accepted inclusion criteria for quality set by Cochrane Database of Systematic Literature from the perspective of engineering. The list of criteria used for this study is very extensive, and not all parameters are of equal importance. Yet, we believe that future studies should try to be more considerate of these engineering perspectives and not only include quality standards that are used in medical sciences. In this study, the checklists were filled out solely using the available data documented in the reviewed papers. The scores, therefore, do not give an absolute value on the methodological quality of the studies, as researchers may have all the needed data available upon request. At this point in time, questions about exposure intensity, exposure duration, and exposure timing are still unanswered.
The Need for Multidisciplinary Studies
Results from studies focusing on the effects of light therapy will be used for the improvement and further development of products and building design. This requires a proper coordination and translation of input and output data.
We know that light for nonimage-forming effects follows a different pathway and procedure in the human brain than for the formation of images (visual). The rods and cones, related to image-forming effects, are connected to the visual cortex in the brain. They have a direct response and are most sensitive to 507 respectively 555 nm. The nonimage-forming intrinsically photosensitive retinal ganglion cells (ipRGCs) are connected to other parts in our brain. 38 The ipRGCs are connected to the biological clock, which regulates our daily rhythm and therefore “builds up exposure effects” as well as depends on the timing of exposure and seems more sensitive to the more bluish part of the spectrum. Taking all of this into consideration, further research has to unveil multiple unknown effects light can have on humans, other the vision-related effects. A well-described protocol for “light” exposure on the eye level may enhance this process. This should be a combined and multidisciplinary effort of a medical/biological researcher and a light engineer.
General consensus on the description of irradiance is necessary not only for all research on the fundamentals of nonimage-forming effects but also to enable the development of light sources that enhance these effects. Without a multidisciplinary approach combining knowledge from the medical and engineering domains, essential data are not reported in the studies, which decrease the value of the results and leave many open questions to those professionals developing new lighting solutions for application in the medical field. It is also uncertain whether studies and their study outcome can be compared.
Light engineers, electrical engineers, and physicists require an adequate description of obtained results in order to design and develop high-quality lighting solutions that cater to the needs for light therapy. If research results are not correctly understood or documented, they may not be practically implemented.
Quality of the Studies
The quality scores resulting from this study range from 0.1 and 0.2. These numbers are unsatisfactorily low, as the results cannot be used by the lighting engineering, building services engineering, and/or construction communities for implementation in practice. For instance, architects cannot design a nursing home with adequate ambient light systems as the studies currently available do not reveal which lighting systems have been used. There are simply too many basic flaws in the methodologies, which could have been prevented if a lighting engineer had been consulted or if details of all the equipment used had been stated in the papers. Both the additional contributions of electric light systems and daylight exposures have been largely ignored. Concerning the light measurements, although several aspects of the related eye exposure of the participants were taken into consideration, this was still insufficient. None of the studies report on daylight exposure or certain restrictions of going outdoors or residing outside the day lit area. Daylight levels can easily exceed the values participants have been exposed to under (electric) light therapy conditions. Even when staying indoors, a position close to the window can reach similar or even higher values than some of the lighting systems used in the studies. None of the studies measured light levels continuously at the eye level. This is important to be able to get the effective exposure, so taking the duration into account as well. None of the studies measure the spectral power distribution of the irradiance. There are strong indications that, next to illuminance levels, also directionality and spectral composition of light play a role in the effectiveness of light therapy. 3
Future Actions
Proper light provides great new opportunities to be used as a nonobtrusive therapeutic treatment. The quality of the photometric, radiometric, and colorimetric light description in measurements regarding light therapy research is, seen from a light engineering point of view, not sufficient and not complete. International experts gathered in Technical Committees of the Commission Internationale d’Eclairage identified the urgent need for an international consensus on defining the right nomenclature and effective quantities for eye-mediated nonimage-forming effects of optical radiation. 39 The next step is the development of a protocol providing instructions on the correct and complete documentation of measurement execution and description of effective light dose for light therapy studies. It should be noted that there are multiple inherent difficulties that accompany doing research in nursing facilities populated by residents with dementia. Some of the parameters cited in this study that are deemed necessary for methodological rigor would be quite difficult to obtain within these settings and populations, even with the added expertise of a lighting engineer. Collaboration between biological, medical, and technical researchers provides input for a protocol including study design, participant selection, light delivery modalities, outcome measures, and all technical aspects of light and lighting, which will be fully accepted and understood by several research worlds.
Footnotes
Acknowledgments
The authors thank Mr. Lennart Schmitz of the Unit of Building Physics and Services of the Department of the Built Environment of Eindhoven University of Technology for designing the preliminary version of the protocol and checklist.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Part of this study was financially supported by the Province of Noord-Brabant (Algemene Subsidieverordening Noord-Brabant, Grant “Samen Slim in Zorg”, as part of the Activiteitenplan Brabant Medical School [BMS] 2013) and Stichting Promotie Installatietechniek (PIT), through the VETO programme (Nursing Home of the Future) of Fontys University of Applied Sciences.