
Abstract
Background:
Dementia prevalence and related caregiving burden are increasing, particularly among Hispanics. We studied the characteristics and mental health of Hispanic caregivers in New York City.
Methods:
We recruited 139 Hispanic family caregivers. We collected data on sociodemographic characteristics and predictors of caregiver burden, measured with the Zarit Caregiver Burden Scale, and depressive symptoms, measured with the Geriatric Depression Scale.
Results:
The mean age was 59.3 ± 10.4 years. The majority of caregivers were daughters and earned less than US$30 000 a year. In multivariate analyses with linear regression, lower satisfaction with social networks was associated with higher caregiver burden and a greater number of depressive symptoms. Higher dementia severity was associated with higher caregiver burden, while higher caregiver comorbidities were associated with higher depressive symptoms.
Conclusions:
Caregiver comorbidities and satisfaction with social support may be targets for intervention that could improve caregiver burden and depressive symptoms among Hispanic caregivers.
Introduction
Dementia is a syndrome characterized by impairment of memory and other cognitive abilities as well as behavior disorder, severe enough to impair the ability to live independently. 1 The most common cause of late-onset dementia is Alzheimer’s disease, 2 comprising between 60% and 80% of cases. Vascular dementia is the second most common cause, comprising about 10% of cases, but approximately 50% of cases of dementia have a vascular component. 2 According to the 2014 Alzheimer’s disease facts and figures report from the Alzheimer’s association, 2 11% of people aged 65 years and older, and a third of people aged 85 years and older have late-onset Alzheimer’s dementia (LOAD). Given the longer life expectancy of the population, the cases of LOAD in persons 65 years and older is expected to increase by 40% by 2025 from current numbers. 2 The Alzheimer’s association also reported that in 2013, unpaid caregivers provided an estimated 17.7 billion hours of informal care valued at over US$220.2 billion. 2 The value of informal care is estimated to be equal to the value of medical and long-term care costs of dementia. 3 Despite increased understanding of dementia, no preventive or curative measure exists, 4 and trials of new agents are discouraging. 5 Consequently, the numbers of caregivers burdened by dementia is increasing. Hispanics, the fastest growing ethnic group in the United States, 6 is also the group with the fastest growing number of cases with dementia. 7 Prevalence of dementia in Hispanics is several times higher than in non-Hispanic Whites (NHWs) nationally (27.9% vs 10.9% in persons aged 75-84 years; 62.9% vs 30.2% in persons 85 years and older) 7 and in New York City. 8
The care of persons with dementia is challenging, 9 –11 requiring intense supervision and often physical support, leading to adverse effects on caregivers’ psychological, physical, 12 –14 and financial health. 7 The burden of caregiving for a person with dementia may be higher in Hispanics compared to NHWs. 15 There is a paucity of research in the characteristics of urban Hispanic caregivers in New York City, who have a high burden of psychosocial and medical stressors 16 that may compound the burden of caregiving. Thus, we recruited 139 Hispanic dementia caregivers for a clinical trial comparing counseling interventions, including a family based intervention, 17 and collected detailed data in-person on their demographics and mental health including caregiver burden and depressive symptoms. Here, we report the demographic characteristics of the sample and the cross-sectional correlates of caregiver burden and depressive symptoms.
Methods
This is the report of a cross-sectional analysis of baseline data from the 139 participants in the Northern Manhattan Caregiver Intervention Project (NOCIP; clinicaltrials.gov NCT01306695). The methods of NOCIP have been described elsewhere. 17 Briefly, NOCIP was a randomized 1:1 pragmatic trial comparing the effectiveness of two 6-month interventions in Hispanic caregivers of persons with dementia, that is, (a) community based case management (CM) conducted by community health workers, and CM in addition to the New York University Caregiver Intervention (NYUCI). 18 For this report, data from the baseline visit prior to randomization were analyzed. The sample in this analysis was recruited between January 01, 2011 and February 28, 2013. The NOCIP was approved by the Institutional Review Board of Columbia University Medical Center.
Study Variables
Demographic variables included age, sex, family position in relation to the person with dementia, whether the caregiver lived with the person with dementia, Hispanic subgroup following methods from the 2010 census, household income, language, and country of origin. We also collected data on the severity of the dementia using the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE; Cronbach α [α] = 0.93). 19,20 The 16-item IQCODE scores range from 16 to 80, with higher scores indicating greater impairment. Caregiver comorbidity was measured using the Charlson Comorbidity Index, 21 which has a potential score range of 0 to 25, and the items were weighted and summed. There were 14 items used. The scores of satisfaction with social support network range from 1 to 6, with 6 indicating greater satisfaction with social support. A number of members in the social network were collected as part of the Stokes Social Network List, 22 and type of dementia was also collected. For each person with whom the respondent has contact in a month, the relationship and whether the respondent feels close to the person are recorded. General satisfaction with the social network, satisfaction with assistance received from the social network in daily activities (eg, help with chores and patient care), and satisfaction with emotional support are evaluated on a 6-point Likert scale; responses range from “very satisfied” to “very dissatisfied”. Higher score indicates less satisfaction with the social support received. 22 Acculturation was measured with the Marin bidimensional acculturation scale (BAS; α = 0.92). 23 The BAS contains 24 items that cover 2 domains (Hispanic and non-Hispanic). The possible total scores range from 1 to 4 for each domain. Scores above 2.5 in both domains indicate biculturalism. Our 2 main outcomes were depressive symptoms measured with the Geriatric Depression Scale (GDS; α = 0.85) 24 and caregiver burden using the Zarit Caregiver Burden Scale (ZCBS; α = 0.85). 25 The GDS contains 30 somatic yes/no items. Total scores range from 0 to 30 with a higher score indicating more severe depression. The ZCBS contains 22 questions about the impact of the care recipient’s disabilities on the caregiver’s life. Items include “Do you feel that your relative asks for more help than he/she needs?” Each item is rated never, rarely, sometimes, quite frequently, or nearly always. Scores range from 0 to 88 with higher scores indicative of more severe burden. Self-reported depression was evaluated with the GDS. All medications currently taken by the participants were recorded during the baseline and follow-up interviews. These medications were later categorized by type.
Statistical Analyses
Linear regression models were used to examine the multivariate correlates of the baseline ZCBS and GDS variables. Both the ZCBS and GDS were normally distributed. Covariates were chosen for inclusion in the regression analyses if the P value was ≤.10 in zero-order bivariate analyses of either the ZCBS or GDS. The covariates that met this criterion and were thus selected for inclusion in the regression models were age, the satisfaction with social support network index, the IQCODE, and the Charlson Comorbidity Index. Missing values for the covariates were imputed using the EM algorithm. Colinearity diagnostics among the covariates were examined and violations were not observed. All analyses were performed using IBM SPSS Statistics version 19.
Results
Table 1 shows the general characteristics of the sample of Hispanic family caregivers from New York City. The mean age was 59.3 ± 10.4 years. The great majority of caregivers were women, and among them, daughters were the majority, followed by spouses. Following the US census format, the majority of participants identified themselves as “other Hispanic or Latino”, as compared with Puerto Rican, South American, and Central American. The most frequent region of origin was the Dominican Republic (41.7%), followed by Puerto Rico (12.9%), South America (12.2%), and Central America (5.8%). Only 16.3% of participants were born in the United States. The majority had a household income less than US $30000 a year (mean monthly household income was US $2094.5 ± 1704.6) and 77% were interviewed in Spanish. The majority of the sample met criteria for biculturalism. The majority of the dementias were reported to be due to Alzheimer’s disease. Depression was reported by 16.8% of the sample and 10.2% reported taking a medication for depression; 34.8% of the sample met GDS criteria for mild depression and 16.7% for severe depression.
Characteristics of the 139 Hispanic Participants in the Northern Manhattan Caregiver Intervention Project (NOCIP).a
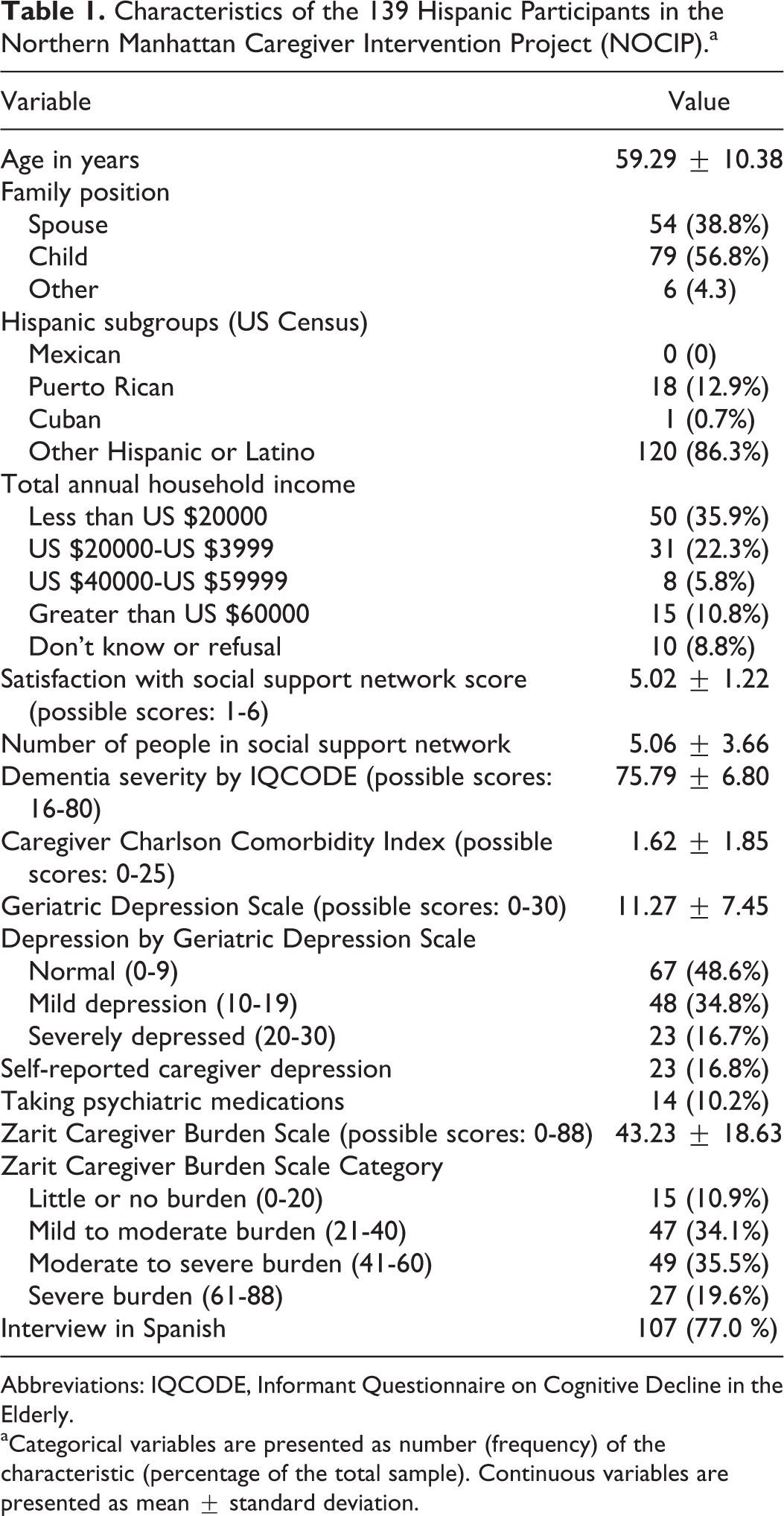
Abbreviations: IQCODE, Informant Questionnaire on Cognitive Decline in the Elderly.
a Categorical variables are presented as number (frequency) of the characteristic (percentage of the total sample). Continuous variables are presented as mean ± standard deviation.
The majority of primary family caregivers were adult children (56.8%) with a mean age of 54.1 ± 7.5 years, followed by spouses (38.8%) with a mean age of 65.9 ± 9.6 years. The proportion of women among spouses (85.2%) and children (86.1%) was similar. National origin did not vary by whether the caregiver was a spouse or adult child (P = .88); 87% of spouses and 86.1% of adult children identified as “other” Hispanic subgroup (not Mexican, Puerto Rican, or Cuban). The country of origin also did not vary (P = .90). The most frequent country of origin identified for both spouses and adult children was the Dominican Republic (40.7% in spouses and 41.8% in adult children). The monthly income was higher for adult children (US $2313.9 ± US $1821.7 vs US $1773.4 ± US $1377.7) but it was not statistically significantly different (P = .10). Satisfaction with social support did not vary by family position (5.1 in spouses ± 1.2 vs 4.8 ± 1.2 in adult children; P = .19), but the number of people in the social support network was modestly lower for adult child caregivers (5.6 ± 3.6 vs 4.4 ± 3.5; P = .06). There were no differences between spouses and adult child caregivers in dementia severity (IQCODE = 76.9 ± 5.3 vs 75.1 ± 7.4; P = .13), caregiver comorbidities (Charlson = 1.8 ± 2.0 vs 1.4 ± 1.5; P = .22), depressive symptoms (GDS = 11.3 ± 7.3 vs 11.2 ± 7.4; P = .91), or report of caregiver burden (ZCBS = 43.4 ± 18.9 vs 42.8 ± 18.7; P = .84). A higher proportion of adult child caregivers compared to spouse caregivers met criteria for biculturalism (62.7% vs 52.0%) but this difference was not statistically significant (P = .37).
We examined zero-order correlates of caregiver burden (ZCBS) and depressive symptoms (GDS). Pearson coefficients (r) were estimated for continuous variables and Phi r for categorical variables. Higher satisfaction with social support network was correlated with less caregiver burden (r = −.316; P = <.001), while dementia severity was related to higher caregiver burden (r = .18; P = .03). Higher satisfaction with social support was also related to less depressive symptoms (r = −.38; P < .001), while dementia severity was not related to depressive symptoms (r = .13; P = .12). Caregiver comorbidity was related to higher depressive symptoms (r = .24; P = .003), while the relation with higher caregiver burden was almost statistically significant (r = .15; P = .08). Older age was correlated with lower caregiver burden (r = −.15; P = .07) and depressive symptoms (r = −.16; P = .05), and these correlations were close to statistical significance. Sex, family position, country of origin, income, number in social support network, type of dementia, language, and biculturalism were not related to either outcome.
Table 2 shows the results of multivariate analyses from a model including independent variables with p ≤ .10 in the bivariate analyses. Satisfaction with social network was significantly related to lower caregiver burden as measured by the ZCBS. Caregiver-reported dementia severity was associated with higher levels of caregiver burden. Caregiver comorbidity was related to higher caregiver burden and this result was close to statistical significance (p = .08). Higher satisfaction with social network was related to fewer depressive symptoms, while caregiver comorbidity was significantly related to more depressive symptoms.
Linear Regression Results Predicting Zarit Caregiver Burden Scale and Geriatric Depression Scale.a
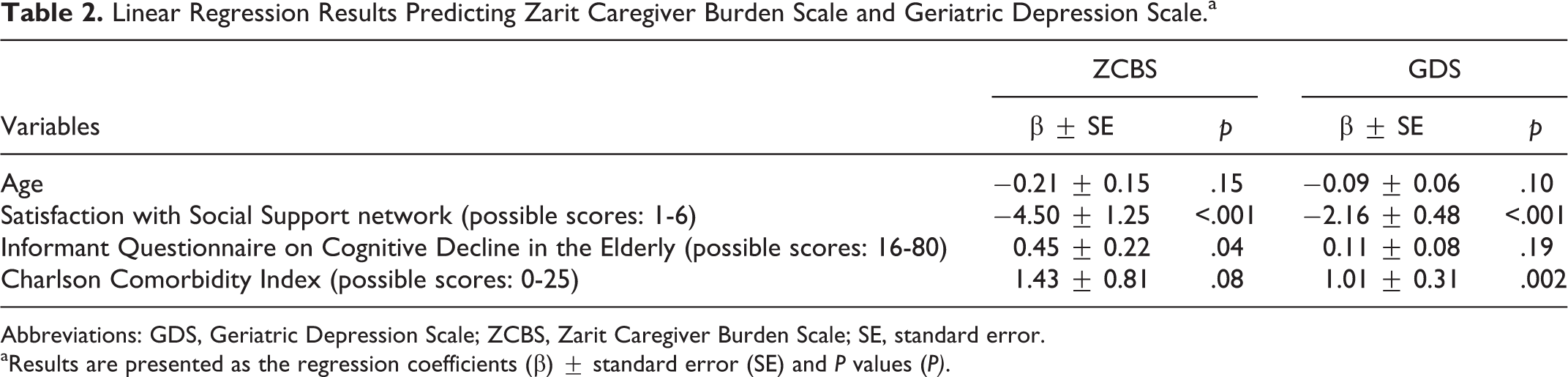
Abbreviations: GDS, Geriatric Depression Scale; ZCBS, Zarit Caregiver Burden Scale; SE, standard error.
a Results are presented as the regression coefficients (β) ± standard error (SE) and P values (P).
Discussion
In this unique cohort of Hispanic dementia caregivers from New York City, we found that the main correlates of depressive symptoms and caregiver burden were satisfaction with social networks, dementia severity, and caregiver comorbidity. We also found that the majority of Hispanic caregivers in New York City are daughters with low socioeconomic resources. Our study is one of the few 26 –28 to describe the characteristics of Hispanic dementia caregivers. As far as we know, this study is the first to report the characteristics of Hispanic dementia caregivers with a majority Caribbean-Hispanic origin in New York City.
The study of Hispanic dementia caregivers is important because Hispanics are the fastest growing demographic group in the United States, 6 have the fastest growing elderly population, 29 have the most accelerated increase in cases with dementia, 29 have a prevalence of dementia that is higher than NHWs, 8 have fewer socioeconomic resources, and have particular attitudes toward caring for relatives. 30,31 Caregiver burden may be higher in Hispanics 15 because caregiving of adult relatives is an expectation of their culture, 32,33 because not accepting the caregiving responsibility could bring shame, 33 and because care of loved ones with dementia puts particular emphasis on family centered care, 34,35 consistent with the concept of familism often identified with Hispanic caregivers. 36 –38 Although most caregivers report no guilt after nursing home placement of persons with dementia, 7 this is less common in Hispanics, 7,39 who delegate less care. 39
In the context of increasing prevalence of dementia without cure or preventive measures 40 with potentially shrinking health care resources, Hispanic families will inevitably face a disproportionate burden of the dementia epidemic. Hispanic caregivers are more depressed than other racial/ethnic groups, 41 but the causes for this disparity are not understood. A 2011 nationwide telephone survey conducted by the Alzheimer’s Association highlighted Hispanic caregivers’ unique socioeconomic characteristics. 7 Compared to NHW caregivers, Hispanic caregivers are younger, are less likely to be married, are more likely to have minor children or grandchildren, are more likely to be a primary caregiver, are more likely to earnless than US $50000 annually, and are more likely to need help balancing work and family and finding personal time. Small studies show Hispanics experience more strain and less social support than other racial/ethnic groups, 42,43 despite extensive social networks, 44 and less acculturated Hispanic caregivers experience more depression. 45 Mixed results from small studies have not clarified the association between social support and caregiver depression in Hispanics. 43,44 Higher acculturation to the United States among Hispanics has been found to be related to both healthy and unhealthy behaviors that may vary by gender. 46 We can only speculate on how acculturation could play a role in dementia caregiving. Acculturation was not associated with caregiver burden or depression, which may be explained by evidence suggesting that a high level of perceived family support is invariable despite changes in acculturation. 47
Not surprisingly, we found that increased dementia severity was related to increased caregiver burden. We also found that higher satisfaction with social networks, but not number of persons in the social network, was related to lower caregiver burden and depressive symptoms. One previous study of rural African American and White dementia caregivers reported on levels of social support, 48 but did not report on how it correlates with depressive symptoms and caregiver burden. Our finding suggests that interventions that improve the quality of social networks may be particularly useful in Hispanics. Family based interventions such as the NYUCI have been shown to reduce stress appraisal 49 and depression 50 in spouse caregivers, and thereby to enable these caregivers to keep their relatives with dementia at home significantly longer than a usual care control group. 51 These outcomes were achieved largely through improving satisfaction with social support from family and friends, and the number of persons in the caregiver’s social network to whom he or she feels close. 52 We observed at baseline that there was a relationship of depression and satisfaction with social support among the Hispanic caregivers. This suggests that the main immediate target of the intervention should continue to be to improve social support. In order to do so, the NYUCI counselor tries to help the caregiver and family to learn to interact in a more productive and positive fashion. This might be achieved by helping the primary caregiver to express his or her needs and the other family members to express their ability to provide help and support. Because the intervention is tailored to the individual situation of each caregiver, person with dementia and family, based on a comprehensive baseline assessment and the counseling sessions, if other problems, such as unmet treatment needs of either the caregiver or the person with dementia become apparent, they can be discussed, and options addressed. There is a paucity of data on the efficacy of the NYUCI in nonspouse and Hispanic caregivers. Our data indirectly suggest that strengthening social support in these 2 demographic groups through interventions such as the NYUCI might improve caregiver burden and depressive symptoms.
Importantly, we found that caregiver comorbidity was an important correlate of depressive symptoms. Given the cross-sectional design of our analysis, we do not know the direction of the association between comorbidities and depressive symptoms, but it seems reasonable to postulate that persons with more comorbidities have more difficulty coping with the stress of caregiving and have more depressive symptoms. It is also possible that the caregivers with more depressive symptoms have higher comorbidities because of neglect of their health or the physical consequences of depressive symptoms of stress. It is unclear if this association is particularly important in Hispanics, perhaps because of neglecting personal health in favor of the care of a loved one. A plausible mechanism that could explain the coexistence of depressive symptoms and physical comorbidities is physiologic stress. 53 It is not clear whether physiologic stress can be modulated in interventions to improve caregivers’ physical and mental health, but our results suggest that more research is needed in this area. It is also important to point out that there is anecdotal evidence that caregivers derive satisfaction from the caregiving experience, but much less is known about the positive aspects compared to the negative aspects of dementia caregiving. 54 It is possible that some or most Hispanic caregivers derive satisfaction from fulfilling their perceived caregiver responsibilities and not see it as a burden. The satisfaction with caregiving needs to be studied in our cohort. It is possible that this aspect could be a resilience factor that decreased the sense of burden and depressive symptoms, the main outcomes explored in this study.
Our study has several limitations. First, this is a cross-sectional analysis, and the directionality of the associations is not clear. It is possible that caregivers with higher depressive symptoms and perceived caregiver burden perceive the dementia in their relatives as more severe, decreased their engagement with social networks, and perceived their health and reported it worse than it really is. Another important limitation is the lack of objective measures of physical health such as vital signs, anthropometric measures, and biomarkers. Given our finding that comorbidities are an important correlate of depressive symptoms in particular, it is important to further characterize physical health with objective measures. Another limitation is that our study focused on the adverse consequences of caregiving. We did not collect qualitative data that might have revealed the gratifying aspects of caregiving in the unique context of caregiving among Hispanics of Caribbean origin. Finally, our sample is a group of caregivers recruited from the community in New York City who volunteered to participate in a clinical trial, and our findings may not be representative of the Hispanic caregivers in the community at large. However, our study has important strengths. It is one of the few studies with detailed data collected in person (rather than through telephone surveys) that focused on Hispanic caregivers. The cohort in our study is being followed longitudinally, and we will be able to report on longitudinal analyses in the future.
In conclusion, the great majority of Hispanic dementia caregivers in our sample from New York City are daughters with limited socioeconomic resources. The main correlates of caregiver burden and depressive symptoms in this sample were dementia severity, lower satisfaction with social networks, and increased comorbidities. Although dementia severity depends on the natural history of the disease and is difficult to treat, 55 it is possible that culturally appropriate interventions that increase satisfaction with social networks and ameliorate comorbidities could improve caregiver health, and more research is needed in this area.
Footnotes
Acknowledgments
First, we are grateful to the participants in our study who agreed to participate despite their caregiving burden. Second, we would like to give special thanks to the New York City Chapter of the Alzheimer’s Association, which provided assistance with outreach. None of the authors have any conflicts related to this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This report was supported by grants P60 MD000206 and P60 MD000206-08S1 from the National Institute on Minority Health and Health Disparities and by grant R01 NR014430 from the National Institute of Nursing Research.