
Abstract
This study was conducted to compare the caregiver burden with regard to Alzheimer’s disease (AD) and frontotemporal dementia (FTD) and to determine the factors affecting the caregiver burden of patients with AD and FTD. A comparative descriptive study design was used. The sample consisted of 90 patients with AD and 44 patients with FTD and their caregivers. Sociodemographic questionnaire, Mini-Mental State Examination (MMSE), the Caregiver Burden Inventory (CBI), Neuropsychiatric Inventory (NPI), and Functional Activities Questionnaire (FAQ) were used. Descriptive statistics, t tests, χ2 test, and multinominal regression were used for analysis. No difference was found with subscales and the total score of the CBI, except time dependency scale. The total NPI and FAQ scores correlated significantly, and the MMSE score did not show a significant correlation with the AD and FTD caregiver burden. The presence and frequency of neuropsychological symptoms differ among patients with FTD and AD, and different symptoms affect the caregiver burdens in both groups.
Introduction
The prevalence of dementia is increasing rapidly in Turkey, as it is worldwide. A study reported that the rate of prevalence of dementia in Turkey is 8.4% and that this rate increases with age. Although the prevalence of dementia in the 55 to 59 year-old age-group is 2.2%, it is 30.4% among individuals aged 75 and older. 1 As the disease advances, restrictions in daily life activities and cognitive and behavioral disorders become more evident, and patients become dependent on other people in order to meet their physical, emotional, economic, and social needs. 2,3
There are many studies in the literature which examine the effects on family members of providing care to patients with dementia. These studies have shown that caregivers experience a care burden through the course of the caregiving process. 4 -6 Dementia is a syndrome of varying types, and different symptoms are observed in patients depending on the type of dementia.
Alzheimer’s disease (AD) is the most common neurodegenerative cause of dementia characterized by cognitive deficits such as amnesia, aphasia, agnosia, and apraxia, emerging as a result of damage in the brain to the hippocampus and cortical areas, as well as behavioral changes. Although behavioral changes are not common in the first stage of AD, apathy and lack of motivation in particular can be observed with the progression of the disease. 6 -9
Frontotemporal dementia (FTD) is the third common cause of neurodegenerative dementia. It is characterized by pathological changes in the frontal and temporal lobes, which are responsible for causal thinking, personality, social behaviors, and control of speech. In individuals with FTD, impulsive and compulsive behaviors, inappropriate sexual behaviors, disinhibition, and dangerous actions due to lack of forethought/insight can all be observed. 8,10 -12
The neuroanatomical pathologies and predilection for affected cortical regions and thus the symptoms and indicators of these 2 types of dementia are different. Therefore, it is essential to determine the dimension of the burden and the factors affecting it among different caregivers who may well experience different levels of burden.
Although the studies in the literature have mainly been conducted with caregivers of patients with AD, it has also been emphasized that caregivers providing care to individuals with FTD have a care burden. In addition, there are studies reporting that the caregivers of patients with FTD have a greater level of burden than the caregivers of patients with AD. 7,13 -15 It is a prime necessity to increase the number of studies concerning caregivers of FTD in order to set up and deliver effective interventions for them.
Most of the studies of the care burden in FTD have been conducted in Western countries. 11,13,16 -20 However, as the cultural diversity of the world continues to increases, so studies about the care burden associated with different types of dementia in different cultures are needed. It is thought that the findings of the present study will facilitate cross-cultural comparisons and culture-oriented care planning for AD and FTD caregivers.
It is thus of paramount importance to determine the differences in the burden among caregivers and the factors affecting the caregiving burden with regard to patients having these 2 different types of dementia in order to shed light on the planning, implementation, and assessment of interventions made by health-care professionals to aid the caregivers. This study was designed to (1) compare the caregiver burdens in relation to FTD and AD and (2) to determine the factors affecting the burdens felt by the caregivers of patients with FTD and AD.
Materials and Methods
Design and Sample
A comparative descriptive study design was used. The sample selection was carried out using nonprobability convenience sampling. A total of 134 participants were recruited into the study. Forty-four had been diagnosed with FTD and 90 with AD. Three types of FTD—behavioral variant FTD (bvFTD; n = 25), nonfluent variants of primary progressive aphasia (n = 13), and semantic variant primary progressive aphasia (n = 6)—were included in the sample. Patients were diagnosed as having FTD or AD by a neurologist (one of the researchers), who based the diagnosis on clinical and cognitive assessments, laboratory tests, and neuroimaging. Dementia was diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition) criteria. 21 For the diagnosis of probable bvFTD, criteria by Rascovsky et al were used, 12 while AD diagnosis followed the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders’ Association (NINCDS-ADRDA) criteria for probable AD. 22 Patients with FTD and AD had equivalent independent variables, and both types of patients with dementia had the same severity of dementia (Clinical Dementia Rating = 1; Table 1).
Demographic Characteristics of Patients.
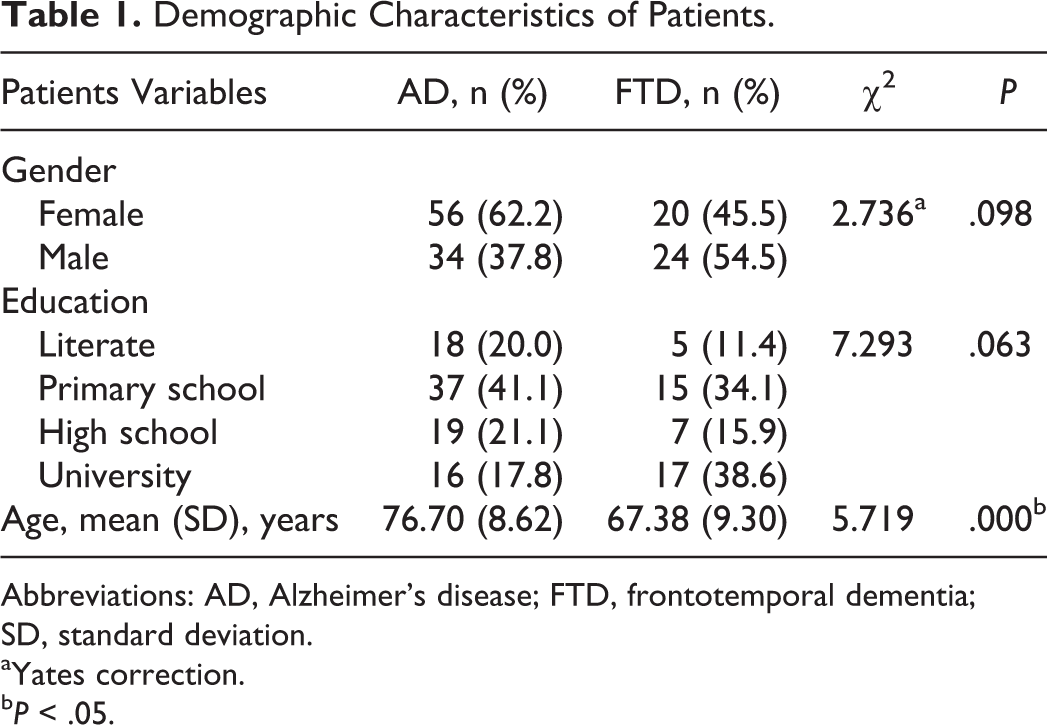
Abbreviations: AD, Alzheimer’s disease; FTD, frontotemporal dementia; SD, standard deviation.
aYates correction.
b P < .05.
The inclusion criteria for the caregivers were as follows: a family member of the patient (spouse, daughter, son, sister, etc), the primary person responsible for caregiving, and providing care for at least 3 hours in a day. The exclusion criteria for the caregivers were having visual, hearing, or speech impairments, and for the patients, the exclusion criteria were as follows: psychiatric disorders such as severe depression, schizophrenia, and bipolar disorder; other neurological diseases; and being diagnosed with another type of dementia (vascular dementia, multi-infarct dementia, or Lewy body dementia).
The factors affecting the burden were similar in both groups (AD and FTD groups): caregivers’ age (P = .07), total duration of caregiving (P =.49), education (P = .84), income (P = .08), employment status (P = .39), relationship to care recipient (P =.11), and Mini-Mental State Examination (MMSE) scores of patients (P = .12; Table 2). The age of the patients (P = .00), the patients’ Functional Activities Questionnaire (FAQ) score (P = .02), and the gender of caregivers (P = .02) were not similar (Table 3). The mean age of patients with AD was 76.70 years (standard deviation [SD] = 8.63) and of patients with FTD was 67.38 years (SD = 9.30). However, age was an anticipated difference between the 2 groups. Patients with AD had a mean FAQ score of 19.22 ± 10.34, while the patients with FTD had a mean FAQ score of 23.86 ± 9.75. The caregivers of patients with AD were mainly the daughter or son (n = 42, 46.7%) and the caregivers of patients with FTD were mainly spouses (n = 21, 47.7%). More than half of the AD (n = 60, 66.7%) and FTD (n = 38, 86.4%) caregivers were female. The mean age of the AD caregivers was 57.41 years (SD = 11.61) and of the FTD caregivers was 52.68 years (SD = 14.86; Table 2).
Demographic Characteristics of Caregivers.
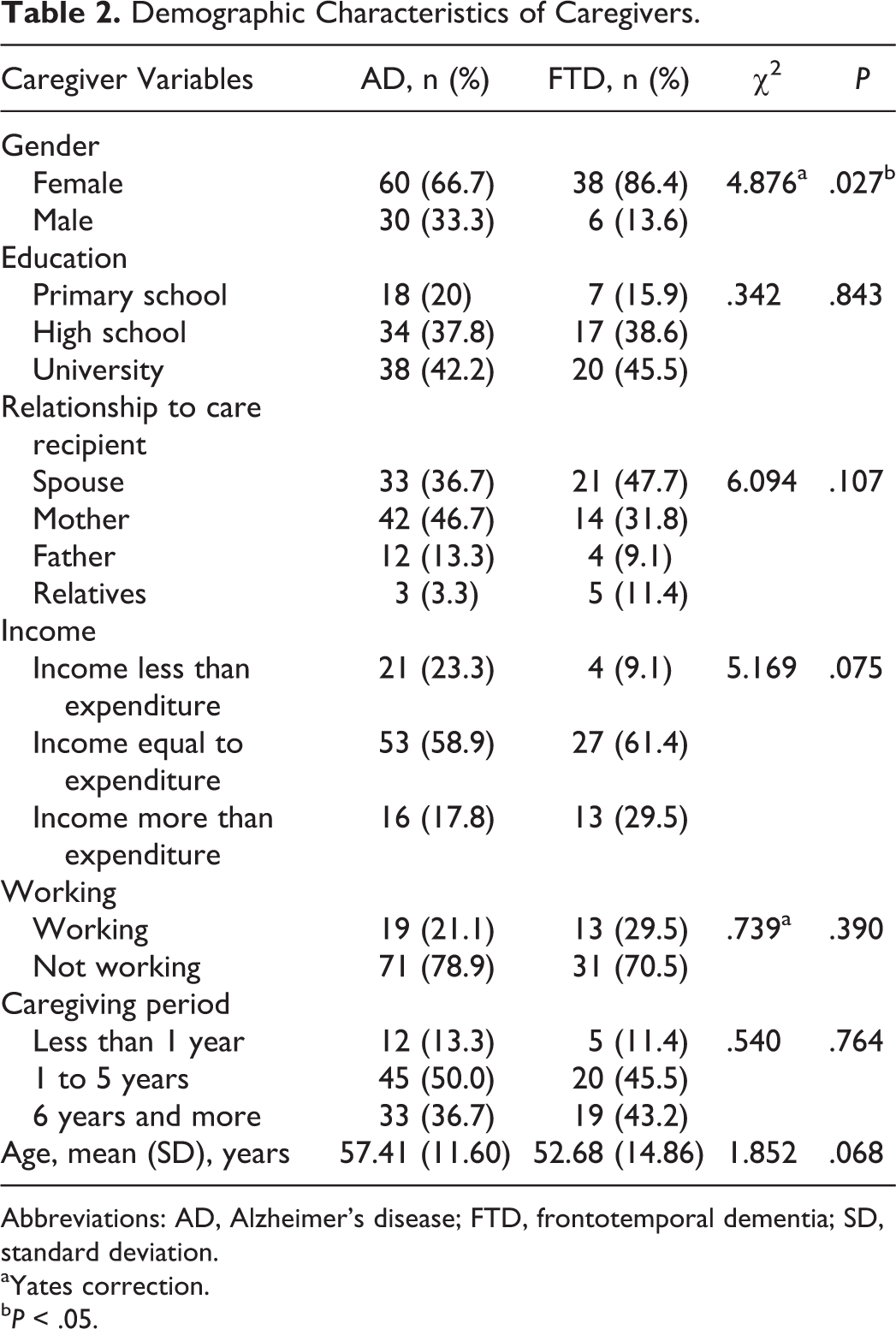
Abbreviations: AD, Alzheimer’s disease; FTD, frontotemporal dementia; SD, standard deviation.
aYates correction.
b P < .05.
MMSE, FAQ, and NPI Scores of Patients and Caregiver Burden of Caregivers.
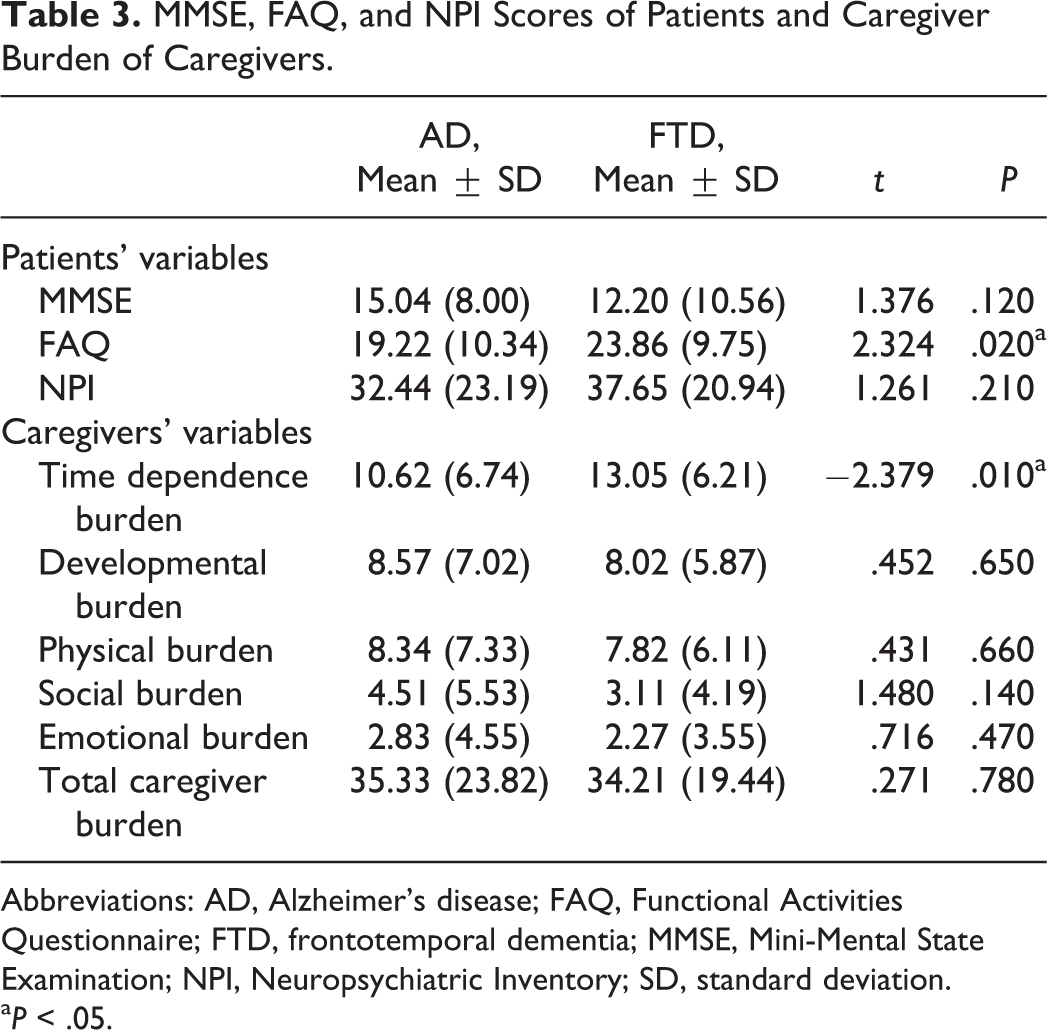
Abbreviations: AD, Alzheimer’s disease; FAQ, Functional Activities Questionnaire; FTD, frontotemporal dementia; MMSE, Mini-Mental State Examination; NPI, Neuropsychiatric Inventory; SD, standard deviation.
a P < .05.
Data Collection
The study was conducted between September 2015 and May 2016 in the dementia outpatient clinic of 1 university hospital in Turkey. The administration of the questionnaire took about 25 minutes. Approval to conduct the study was obtained from the ethical committee of the Dokuz Eylül University, Noninvasive Research Ethics Board. If the participants agreed to participate in the study (after written permission had been obtained), they were asked to complete the questionnaires.
Instruments
A sociodemographic characteristics questionnaire, the Neuropsychiatric Inventory (NPI), 23 and the Caregiver Burden Inventory (CBI) 24 were applied. The NPI was used to assess neuropsychiatric symptoms, and the CBI was used to examine the caregiver burden. The FAQ 25 was used to determine performance based on 10 complex activities in everyday life. Mini-Mental State Examination 26 was used to assess the cognitive function of patients.
Statistical Analysis
The caregiver burden and differences in subscale scores between FTD and AD caregivers were evaluated with independent t tests. 27 A value of P < .05 (95% confidence interval) was considered statistically significant. The mean age of the caregivers, mean duration of daily caregiving, mean age of the patients, and MMSE and NPI mean scores by groups were analyzed using t tests. Level of education, monthly income, employment status, and caregiving duration in the groups were analyzed by a χ2 test. 27 In general, there was no statistically significant difference among the caregivers in terms of these features (P > .05). Logistic regression analysis was used to assess which factors predict caregiver burden.
Results
Caregiver Burden of AD and FTD Caregivers
The CBI scores of the AD and FTD caregivers were 35.33 ± 23.82 and 34.21 ± 19.44, respectively. In both groups, caregivers reported more burden for the time dependence subscale and less burden for the emotional subscale. The CBI scores and many of the subscales in the CBI were statistically equivalent (Table 3). The time dependency burden among all subscales (P = .01) of the FTD caregivers was significantly higher than that of the AD caregivers.
Common Factors Affecting the Caregiver Burden in AD and FTD Groups
The total FAQ and NPI scores correlated significantly with the AD and FTD caregiver burden, whereas the MMSE score did not significantly correlate with the AD and FTD caregiver burden. The total NPI and FAQ scores of those with FTD were higher than those with AD. The MMSE scores of those with FTD were less than those with AD.
The factors affecting the caregiver burden in patients with AD
The FAQ score was 19.22 (SD = 10.34), the mean NPI score was 32.44 (SD = 23.19), and the MMSE score was 15.04 (SD = 8.00) for people with AD. The total FAQ and NPI scores correlated significantly with the AD caregiver burden (Table 4).
Logistic Regression Analysis Using CBI Scores From Patients With FTD and AD as the Dependent Variable.a
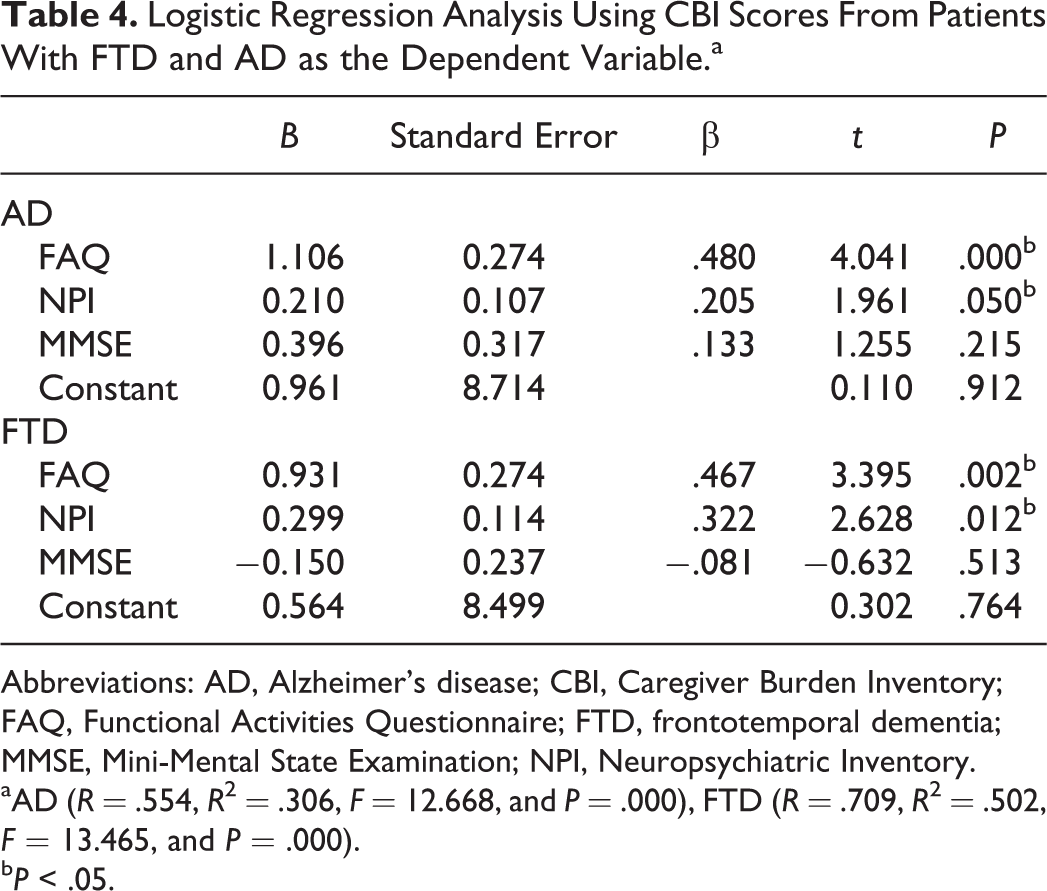
Abbreviations: AD, Alzheimer’s disease; CBI, Caregiver Burden Inventory; FAQ, Functional Activities Questionnaire; FTD, frontotemporal dementia; MMSE, Mini-Mental State Examination; NPI, Neuropsychiatric Inventory.
aAD (R = .554, R 2 = .306, F = 12.668, and P = .000), FTD (R = .709, R 2 = .502, F = 13.465, and P = .000).
b P < .05.
The most frequently reported symptom for patients with AD was delusion; however, delusion as a symptom did not manifest the strongest correlation with the caregiver burden in AD. In AD group analysis, aberrant motor behavior (P = .043) was the only symptom that correlated significantly with the AD caregiver burden. The total FAQ and NPI scores correlated significantly with the AD caregiver burden.
The factors affecting the caregiver burden in patients with FTD
For individual with FTD, the FAQ score was 23.86 (SD = 9.75), the mean NPI score was 37.65 (SD = 20.94) and the MMSE score was 12.20 (SD = 10.56). The total FAQ and NPI scores correlated significantly with the FTD caregiver burden (Table 4).
The most frequently reported symptom for patients with FTD was apathy. However, the symptom of apathy did not manifest the strongest correlation with the caregiver burden in FTD. For FTD group analysis, 3 subscales of NPI correlated: hallucinations (P = .010), euphoria (P = .005), and sleep disturbances (P = .046).
Discussion
Many of the studies conducted have been about AD caregivers, and this study therefore examined and compared findings with regard to the caregiver burden associated not only with AD but also with FTD.
Caregiver Burden of AD and FTD Caregivers
The burden experienced by the caregivers of individuals having AD is a well-known topic in the literature. It is necessary to better illuminate questions such as what dimension of burden is experienced by the caregivers of individuals with different types of dementia. Most of the studies examining the burden of FTD caregivers have used different measurement tools and, in general, have not examined burden subscales. In the current study, the CBI, which allows for assessing different dimensions of burden, was used to compare caregivers’ burdens. It was found that the caregivers of patients with FTD had a higher burden in terms of time dependency. The higher burden of time dependency subscale in the FTD group can be explained on the basis of the lower functionality scores in this group. The functional state of the patient is one of the major factors affecting the caregiver burden. 17,22 Caregivers need to spend more time providing care when there is a loss of autonomy, especially financially, and when it is necessary to help the patient take medicines, eat, and use the telephone. In the present study, it was concluded that patients with FTD are more dependent in terms of functionality and thus require more care. In general, the functional state of patients with FTD is better than that of patients with AD, 28 but the functionality average score of patients with FTD was found to be lower in the present study, and this result might be attributed to the characteristics of the sample.
Factors Affecting the Caregiver Burden
This study found that total NPI scores correlated with the AD and FTD caregiver burden. Previous studies have stated that NPI scores and behavioral changes appear to correlate with caregiver burden in AD 11,29,30 and in FTD. 26 Behavioral symptoms are one of the most significant factors affecting the burden on caregivers. It is known that deterioration in behavioral symptoms affects caregiver burden more than deterioration in cognitive states. 13,31,32
In the present study, the neuropsychiatric symptoms observed in each group had differing degrees of presence, frequency, and intensity of symptoms, although NPI scores were found to be similar in patients with FTD and AD. In addition, the neuropsychiatric symptoms affecting the caregiver burden in each patient group were different. The current study is consistent with previous studies in that it shows increased agitation, depression, apathy, disinhibition, irritability, and eating abnormalities for FTD, but not so much for sleep disturbance and aberrant motor behaviors. 20 In the present study, the most frequently reported symptom for patients with FTD was apathy (Figure 1). However, apathy did not show the strongest correlation with the caregiver burden in FTD. For FTD group analysis, 3 symptoms correlated: hallucinations, euphoria, and sleep disturbances.
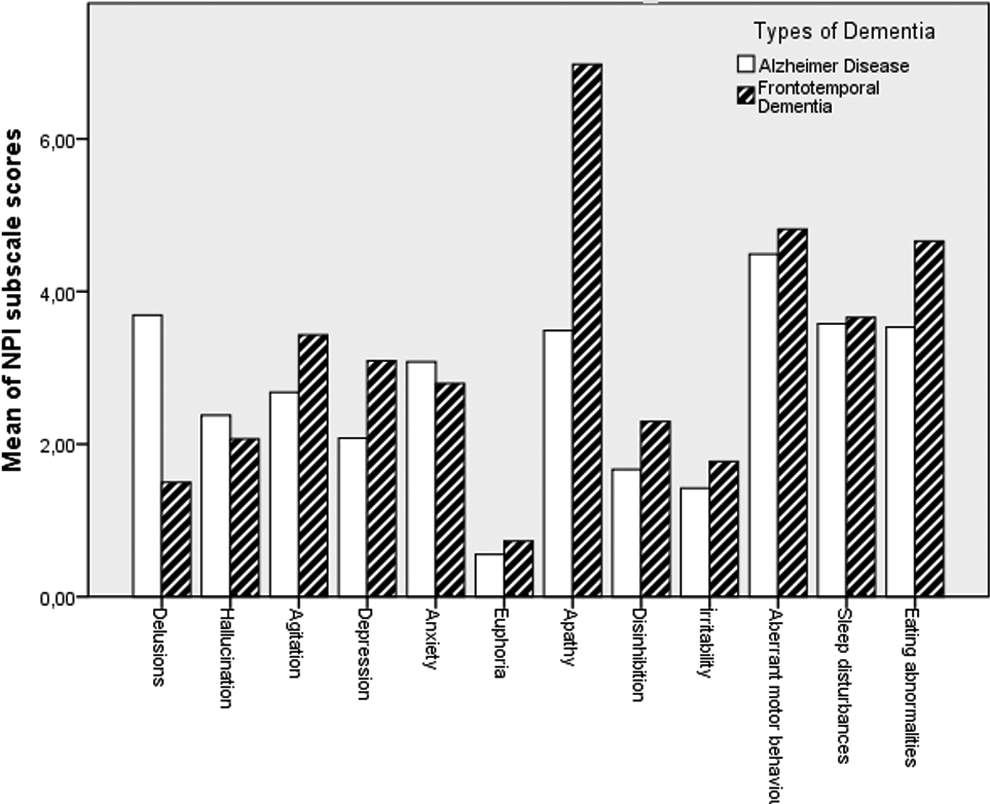
Mean NPI subscale scores in AD and FTD. AD indicates Alzheimer’s disease; FTD, frontotemporal dementia; NPI, Neuropsychiatric Inventory.
Similar to other studies, 33,34 this study reported that apathy is a common symptom in patients with FTD. Despite being among one of the most frequent negative neuropsychiatric symptom, apathy did not correlate with CBI. In the other studies, apathy was observed to be a symptom increasing the caregiver burden and distress. 35,36 It was emphasized in these studies that apathy usually accompanies depression and thus affects the caregiver burden. 35 Individuals with apathy need more support in order to initiate and maintain their activities and this increases the caregiver burden. 37 In contrast to these studies, generally caregivers do not consider apathy as a problem, and apathy is an indispensable component of the disease. 38 In Turkey, families are generally responsible for the care of patients with dementia, and care is perceived as a responsibility toward the patient, so caregivers do not expect patients to carry out activities independently. On the contrary, it is thought that patients with apathy cause less burden on the caregivers when compared to an aggressive patient. Patients with apathy are perceived as quiet and calm patients and the care provided to them causes less burden on their families. 11,39
Hallucinations are common psychotic symptoms and are reported by caregivers to be among the symptoms most difficult to manage. 11 Hallucination is defined as perceiving something which is not present, or the belief in such a perception, and individuals with dementia usually experience visual hallucinations, unlike, for instance, patients with schizophrenia. 18 It is thought that caregivers have difficulty, feel despair, and may also feel afraid when patients talk about nonexistent things or insist on the reality of what they perceive. Thus, a greater caregiver burden may be associated with the presence, intensity, and content of a patient’s hallucinations. It is to be expected as a result that the burden of a caregiver whose patient has disturbing hallucinations will be greater. Even though the frequency of hallucination in the FTD group is rather low and generally confined to a subgroup of genetically hereditary c9orf72 mutation, 40 the burden related to this symptom is greater.
The relationship between sleep disorders and caregiver burden is also supported by another study. 39,41 Merrilees et al reported that sleep disorders observed in patients had a strong correlation with the distress felt by the caregiver and that the quality of sleep of caregivers also deteriorated significantly. Merrilees et al also reported that 92% of caregivers had sleep problems and that 41% of them needed to take sleeping aids more than 3 times a week. When patients do not get enough sleep, the intensity and frequency of their behavioral symptoms may increase and this might make them more challenging for the caregivers. Due to sleep disorders, caregivers themselves may be unable to sleep, and since their own strength may decrease as a result of lack of sleep, it may become even more difficult for them to deal with deteriorating symptoms.
A striking finding of this study is that euphoria can be correlated with caregiver burden. Euphoria is a nonconcealable positive symptom. When patients act in a manner inconsistent with the social environment/situation, caregivers may be obliged to explain the patient’s disease to those in the vicinity. It is thought that caregivers may experience embarrassment due to this situation. An abnormal state of happiness displayed by the patients in social environments leaves caregivers in a difficult situation, and this becomes even more challenging when communicating with other individuals who may be more subdued. Respect for sorrow is one of the most important features of Turkish culture. It is thought that the impact of euphoria on the caregiver burden, which is not found commonly in the literature, might be attributed to the specific features of culture.
For patients with AD, the most frequently reported symptoms were aberrant motor behaviors, delusion, and sleep disturbances. In AD group analysis, aberrant motor behavior was the only symptom that correlated significantly with the AD caregiver burden. Liu et al reported that aberrant motor behavior and hallucinations were the symptoms that correlated most significantly with caregiver burden in different types of dementia. In the current study, aberrant motor behavior correlated with the CBI in patients with AD. In the literature, there are studies reporting that aberrant motor behaviors lead to caregiver burden. 29,42 Aberrant motor behaviors are directly observable and may result in a decrease or increase in motor activities. Such behaviors create the risk of continuous idle activity/loafing or, alternatively, leaving the domestic setting and becoming lost and may result in behaviors such as disinhibition which are not compatible with sociocultural norms. Caregivers have difficulty managing the inappropriate and aberrant motor behaviors of the patients as well as their outcomes.
Cognitive function and daily activity function showed conflicting results in the literature. 43,44 Some studies have reported that lower cognitive function is correlated with caregiver burden, 45,46 whereas others have found that cognitive function itself does not affect caregiver burden. 25,29,30,33,47 In the present study, the cognitive assessment scores were not related to caregiver burden. On the other hand, the functionality scores correlated with AD and FTD caregiver burden in this study. This finding is similar to those in the literature. 30,48 It is thought that caregivers may have a higher degree of burden as the need for care increases when functionality decreases and when adequate support for home care in order to meet these needs cannot be provided.
Health professionals need to be aware that family caregivers experience a significant caregiver burden and require tailored education and support. When planning interventions to assist the caregivers of patients with dementia, not only the families of patients with AD but also the relatives of patients with FTD should be taken into consideration. Family members caring for patients with FTD experience as great a burden as family members caring for patients with AD.
Conclusion
The time dependency burden of caregivers of patients with FTD is greater than that of caregivers of patients with AD. However, it was determined that both family member groups had similar burden levels in terms of the other subscales and total caregiver burden score averages. The factors most affecting the caregiver burdens in both groups are the daily activity functions and patients’ neuropsychiatric symptoms. No statistically significant relationship was detected between the cognitive states of patients and caregiver burdens. The caregiver burdens are similar in both types of dementia, despite the average behavioral score of patients with FTD is higher than that of patients with AD. This is because of the fact that neuropsychiatric symptoms with varying frequencies and intensities are observed in patients with each type of dementia. Every neuropsychiatric symptom also has a different impact on the caregiver burden. Thus, health-care professionals and family members caring for patients having different types of dementia need to learn how to manage different neuropsychiatric symptoms. In this respect, it is of paramount importance to structure training for caregivers in accordance with the type and characteristics of the dementia from which their patients are suffering. With respect to those caring for patients with dementia, the standard training should be refined and appropriate interventions should be planned and adapted for the type of dementia as well as for the level of functionality and neuropsychiatric symptoms observed in patients. Only in this way can interventions that aim to reduce the caregiver burden be undertaken. We believe that the data from the present study will provide a guide for preparing training in this field.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.