
Abstract
Purpose:
This study examined whether seniors’ exposure to direct-to-consumer advertising (DTCA) for Alzheimer’s disease (AD) medicine contributes to his or her subjective and objective knowledge of AD.
Methods:
A self-administered survey was conducted with a sample of 626 US seniors who were registered for an online consumer research panel.
Results:
The study found that (1) exposure to DTCA for AD medicine was positively related to seniors’ subjective knowledge of AD, (2) DTCA exposure had no significant relationship with overall objective knowledge of AD, and (3) DTCA exposure might influence knowledge of specific features of AD.
Implications:
Although DTCA for AD medicine may induce people to “feel” knowledgeable about AD, it may not result in an equivalent increase in actual knowledge. Therefore, to enhance doctor–patient interactions, both patients and doctors should be aware that although DTCA delivers important and potentially useful health information, it does not necessarily enhance actual knowledge.
Keywords
Introduction
Since the Food and Drug Administration relaxed its restrictions on direct-to-consumer prescription medicine advertising (DTCA) on television in 1997, DTCA expenditures have rapidly increased. 1 Opinions regarding the merits of such advertising are largely polarized into 2 camps. On one side, critics note that DTCA fails to provide fair and balanced information regarding health issues, touts medication while ignoring alternative and equally efficacious treatment options, induces people to seek unnecessary medications, and interferes with the doctor–patient relationship. 2 On the other side, its advocates claim that DTCA informs individuals about health conditions and treatment options, raises the public’s awareness of stigmatized diseases, leads individuals to seek more information and professional help, and empowers patients to engage more actively in doctor–patient interactions. 3
The rise in DTCA mirrors a transition in the United States toward consumers assuming an increasingly active role in seeking health information and making health care decisions. 4 According to a national survey by the Kaiser Family Foundation, more than 90% of US consumers are aware of DTCA. 5 The average television viewer in the United States encounters approximately 15 hours of DTCA per year. 6 Given this high level of exposure and awareness, DTCA has been reported to influence the public’s beliefs and coping actions related to various diseases, including depression and erectile dysfunction. 7 -9 However, no such research has been reported in the context of DTCA for Alzheimer’s disease (AD) medicine in the United States, although Hall and Jones 10 examined how Australian consumers respond to message appeals in such advertising. In fact, having concluded that DTCA for AD medicine typically presents multilayered messages combining persuasive techniques with facts about the disease and medications, Gooblar and Carpenter 11 encouraged future researchers to examine what consumers in the United States could learn from such advertisements. Given the growing prevalence of AD in the United States and the potentially impaired cognitive capacity of at-risk individuals, it is critical to examine how DTCA may influence the potential patients’ knowledge of this disease.
To address this need, this study investigated whether exposure to DTCA for AD medicine contributes to seniors’ knowledge of AD. In pursuing this inquiry, it is important to note that knowledge has the following 2 underlying conceptual dimensions: subjective and objective. The former refers to a person’s own judgment of the extent to which he or she is knowledgeable about a particular area, whereas the latter refers to what he or she actually knows. 12 Given that the subjective and objective dimensions are conceptually distinct, 12,13 this study first examined how exposure to DTCA for AD medicine independently relates to the two dimensions of knowledge of AD among US seniors. Then, the study explored whether DTCA exposure could shape one’s knowledge of various specific features of AD.
Exploring the following question seems to be critical in informing the social debate regarding the educational potential of DTCA: does exposure to DTCA enhance the public’s knowledge of diseases? 14,15 However, the question remains unanswered. Based on this notion, this study focused on the role of DTCA in constructing consumer knowledge of AD. In the DTCA literature, there is much research on consumer awareness and attitudes toward DTCA and consumer perception of its value as a source of health information. 10,16,17 Although knowledge of a disease is an important construct that is capable of shaping health behaviors, 18 the question of how DTCA can shape consumer knowledge of a disease remains largely unexamined in the literature, particularly in the context of AD medicine. It is also noteworthy that for effective patient education and counseling, it is important to consider how much individuals know about AD and what may have contributed to their knowledge or the lack thereof. In this regard, the current study has implications for doctor–patient communications.
Methods
Sample and Recruitment
The institutional review board for human participants at a southern state university in the United States approved the protocol. All respondents provided informed consent for their participation in the study. A sample of US seniors at least 65 years of age was obtained for data collection. The seniors were registered members of the Survey Monkey Contribute online research panel. A total of 3991 recruiting announcements were distributed to the panel members; 626 seniors returned usable surveys, yielding a response rate of 16.7%. Members of the panel first received an e-mail presenting a brief description of the study. The invitation contained the URL of the survey Web site. Members who clicked the URL were able to directly log on to the site. After confirming that they were 65 or older, reading the informed consent and providing their consent to participate, the respondents proceeded to take the survey.
Measures
The survey instrument was designed to measure independent and dependent variables (self-reported exposure to DTCA for AD medicine and subjective and objective knowledge of AD), correlates related to life experiences involving AD (interpersonal experiences with AD, experience of caring for someone with AD, self-reported overall health status, and exposure to general, nonadvertising media coverage of AD), and general demographic background (gender, age, education, and household income). The survey first measured the respondents’ subjective knowledge of AD, and then interpersonal experiences, caretaking experience, and overall health status were measured. The survey then assessed the respondents’ objective knowledge of AD, exposure to DTCA for AD medicine, and exposure to general, nonadvertising media coverage of AD. At the end of the study, general demographic variables were measured. The survey required approximately 15 minutes to complete.
To report their subjective knowledge of AD, the respondents answered the following question on an 11-point scale (0 = not at all knowledgeable and 10 = extremely knowledgeable): “How knowledgeable would you say you are about Alzheimer’s disease?” 19 Interpersonal experiences were measured by having respondents check “yes,” “no,” or “don’t know” to report whether they knew of someone among their family members, relatives, friends, and neighbors with a history of AD. For each respondent, the number of “yes” responses across the 4 referents was obtained to create a single index of interpersonal experiences. Caretaking experience was reported with “yes” and “no known experience” options in response to the following question: “Have you ever taken care of someone with Alzheimer’s disease?” On a 4-point scale (1 = poor and 4 = excellent), the respondents self-reported their overall health status. 20
Next, 10 items were used to assess the respondents’ objective knowledge of AD. 21 The respondents checked “true,” “false,” or “don’t know” regarding 10 true or false statements pertaining to various features of AD, including “Alzheimer’s disease can be diagnosed with a blood test” (a sample false statement) and “Alzheimer’s disease is generally fatal” (a sample true statement). For each individual, the number of correct responses was obtained to create a single index of objective knowledge ranging from 0 (no item answered correctly) to 10 (all items answered correctly).
Exposure to DTCA for AD medicine was measured by instructing the respondents to use a 6-item, 7-point scale (1 = never and 7 = very often) to indicate how often they had seen, read, or heard advertisements for AD medicine from the radio, newspapers, magazines, television, the Internet, or other media (eg, flyers, brochures, outdoor, etc.) in the past 6 months. 22 Responses across the 6 media types were averaged to produce a single index of DTCA exposure.
Exposure to general media coverage of AD was measured by asking the respondents to use a 4-item, 7-point scale (1 = never and 7 = very often) to indicate how often they had seen, read, or heard instances other than advertisements where AD or prescription medicine for AD was depicted or discussed in the following 4 media categories: (1) television news, documentaries, and current affairs; (2) television entertainment programs (eg, soap operas, sitcoms, drama, and movies); (3) articles in newspapers and magazines; and (4) the Internet. 23 Responses for the 4 types were averaged to obtain a single index of exposure to general media coverage of AD.
A variety of demographic questions (ie, gender, age, education, and household income) were included at the end of the survey. Analyses were conducted using IBM SPSS 24 version 21 to examine the research objectives. These analyses included basic descriptive statistics, multiple regressions, and logistic regressions.
Results
Sample Characteristics
Table 1 summarizes the sample characteristics in terms of demographic background. The sample members ranged in age from 65 to 92 years (mean [M] = 74.23, standard deviation [SD] = 6.15). The respondents primarily consisted of whites (95.8%), followed by African Americans (1.9%), Asians (.5%), and Hispanics (.5%). The majority (70.8%) had an annual household income of US$25 000 to US$99 999, with 15.5% reporting less than US$25 000 and 13.7% reporting US$100 000 or more. The majority of the respondents were currently married (n = 384, 61.3%) and were not employed (n = 524, 83.7%). Self-reported personal history of AD was reported with “yes” and “no” options. Because only 4 (.6%) respondents reported that they had been diagnosed with AD, these individuals were excluded from further analysis.
Demographic Profile of Respondents.a
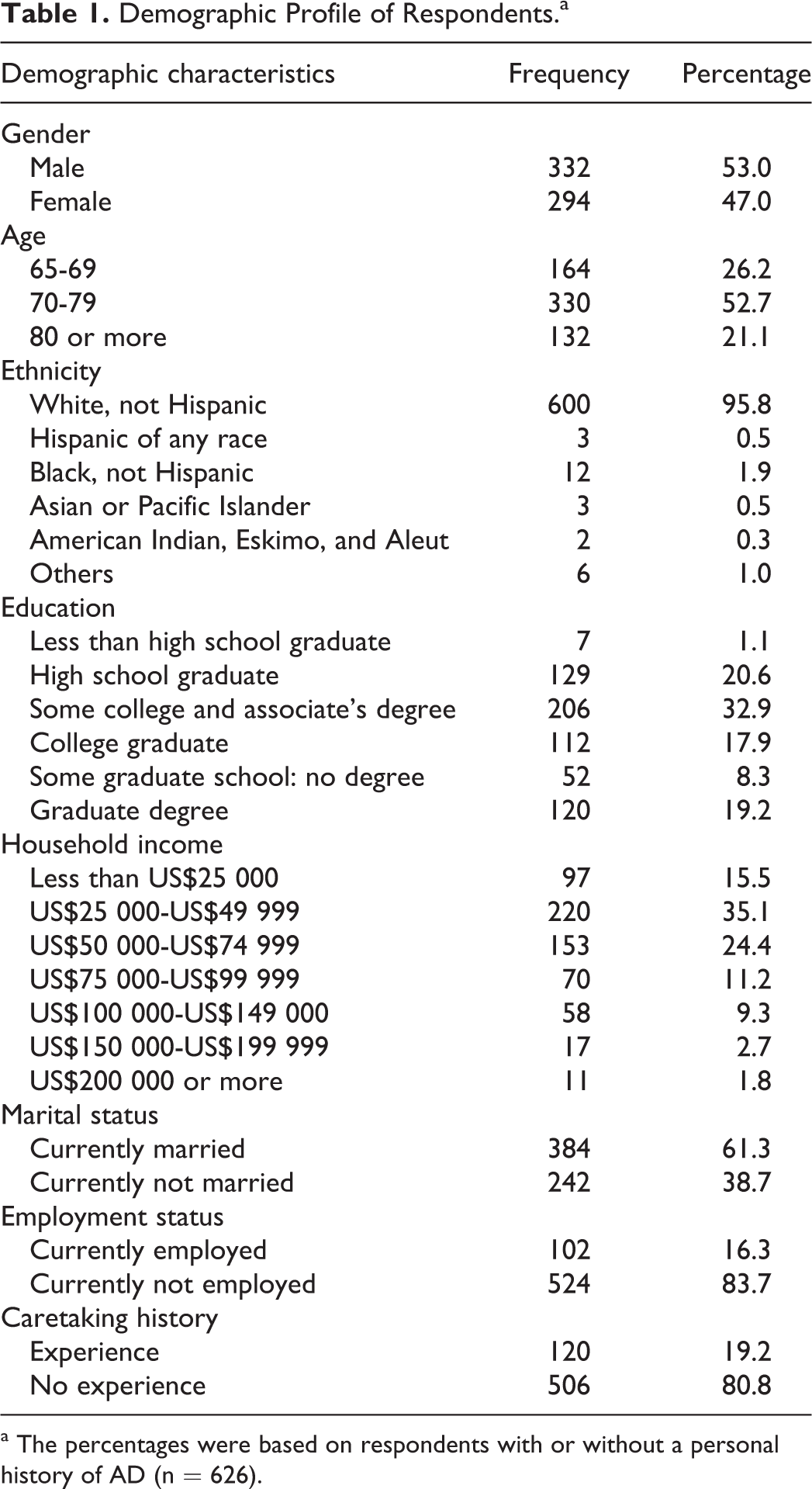
a The percentages were based on respondents with or without a personal history of AD (n = 626).
Descriptive Statistics
Among respondents without a self-reported personal history of AD (n = 622), a considerable number of respondents were aware of family members (n = 109, 17.5%), relatives (n = 155, 24.9%), friends (n = 228, 36.7%), and neighbors (n = 137, 22.0%) who had experienced AD, whereas 259 (41.6%) indicated that they did not know anyone with AD among their close others. The sample’s mean rating for the sum of interpersonal experiences was 1.01 (SD = 1.07). A total of 120 (19.3%) respondents reported having personal experience in caring for patients with AD. The respondents generally reported that their health status was good (M = 2.93, SD = .66).
The mean rating for self-reported exposure to DTCA for AD medicine was 2.40 (SD = 1.20). Of the 6 media types that were measured, television (M = 3.30, SD = 1.93) and magazine (M = 2.59, SD = 1.63) appeared to be the media through which the respondents most frequently encountered DTCA for AD medicine. The mean rating for exposure to general, nonadvertising media coverage of AD was 2.11 (SD = 1.16). Television news, documentaries and current affairs programs (M = 2.44, SD = 1.52), and articles in newspapers and magazines (M = 2.31, SD = 1.47) had higher mean ratings compared with the other 2 categories. The mean rating for subjective knowledge was 5.65 (SD = 2.06), and the mean rating for objective knowledge was 6.54 (SD = 1.71).
Direct-to-Consumer Advertising and Subjective Knowledge
To examine whether exposure to DTCA for AD medicine is associated with seniors’ subjective knowledge of the disease, a hierarchical multiple regression model was constructed. In the first block, gender, age, education, and household income were entered as general demographic control variables. The second block included potential correlates pertaining to various life experiences regarding AD, including self-reported overall health status, interpersonal experience, caretaking experience, and exposure to general media coverage of AD. Exposure to DTCA for AD medicine formed the third block.
Table 2 summarizes the results. All statistics represent the full regression model. The results indicated that DTCA exposure was positively associated with subjective knowledge (β = .11, P < .05). The positive coefficient indicated that the more frequently seniors were exposed to DTCA for AD medicine, the more knowledgeable about AD they considered themselves to be. It was notable that this relationship was statistically significant after controlling for correlates representing sources or occasions other than advertising from which the respondents might have received information about AD, such as interpersonal experiences involving AD, caretaking experience, and exposure to general media coverage of AD.
Hierarchical Regression for Subjective Knowledge.a
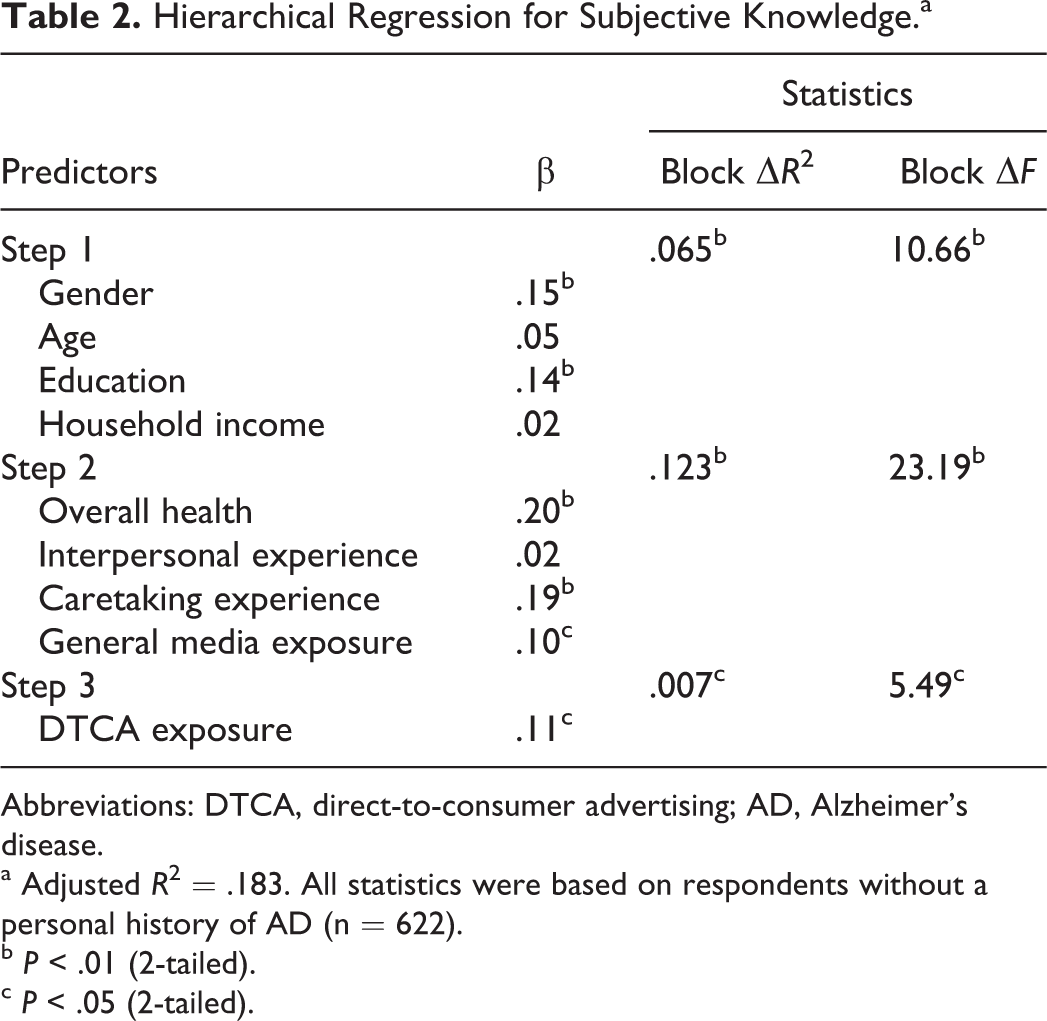
Abbreviations: DTCA, direct-to-consumer advertising; AD, Alzheimer's disease.
a Adjusted R2 = .183. All statistics were based on respondents without a personal history of AD (n = 622).
b P < .01 (2-tailed).
c P < .05 (2-tailed).
Table 2 also reveals a number of correlates that were significantly related to subjective knowledge of AD. First, females reported higher levels of subjective knowledge than males did (β = .15, P < .01). Educational level (β = .14, P < .01), overall health status (β = .20, P < .01), and caretaking experience (β = .19, P < .01) were also positively related to subjective knowledge. Exposure to general media coverage of AD, which was another source of mediated information about the disease, was also positively associated with subjective knowledge (β = .10, P < .05). Overall, the results suggested that in addition to exposure to DTCA for AD medicine, a wide range of demographic, life experience, and media exposure factors potentially influence the extent to which seniors feel knowledgeable about AD.
Level of Objective Knowledge
Objective knowledge was measured by asking the respondents about the truth or falsity of 10 statements related to various features of AD, such as its symptoms, prevalence, and lifetime risk. For each respondent, the total number of correct responses represented the level of overall objective knowledge. It was notable that the correlation between subjective and objective knowledge was statistically significant but low (r = .26, P < .01), confirming previous research showing that the 2 knowledge dimensions often have a low level of correspondence. 12
Table 3 shows the distribution of responses for each statement. The percentage of respondents correctly identifying the truth or falsity of a statement varied widely across questions. For example, with respect to the false statement “Alzheimer’s disease could be contagious,” the overwhelming majority (n = 585, 94.1%) provided the correct response (ie, they checked “false”). Regarding the false statement “Alzheimer’s disease can be diagnosed with a blood test,” approximately half of the respondents (n = 259, 41.6%) provided the correct response (ie, they checked “false”). Regarding the true statement “Symptoms of depression are similar to those of Alzheimer’s disease,” approximately one-third (n = 201, 32.3%) checked “true.” Only 2.4% (n = 15) answered all questions correctly, and 2 (.3%) respondents did not provide any correct answers.
Responses to Objective Knowledge Items.a
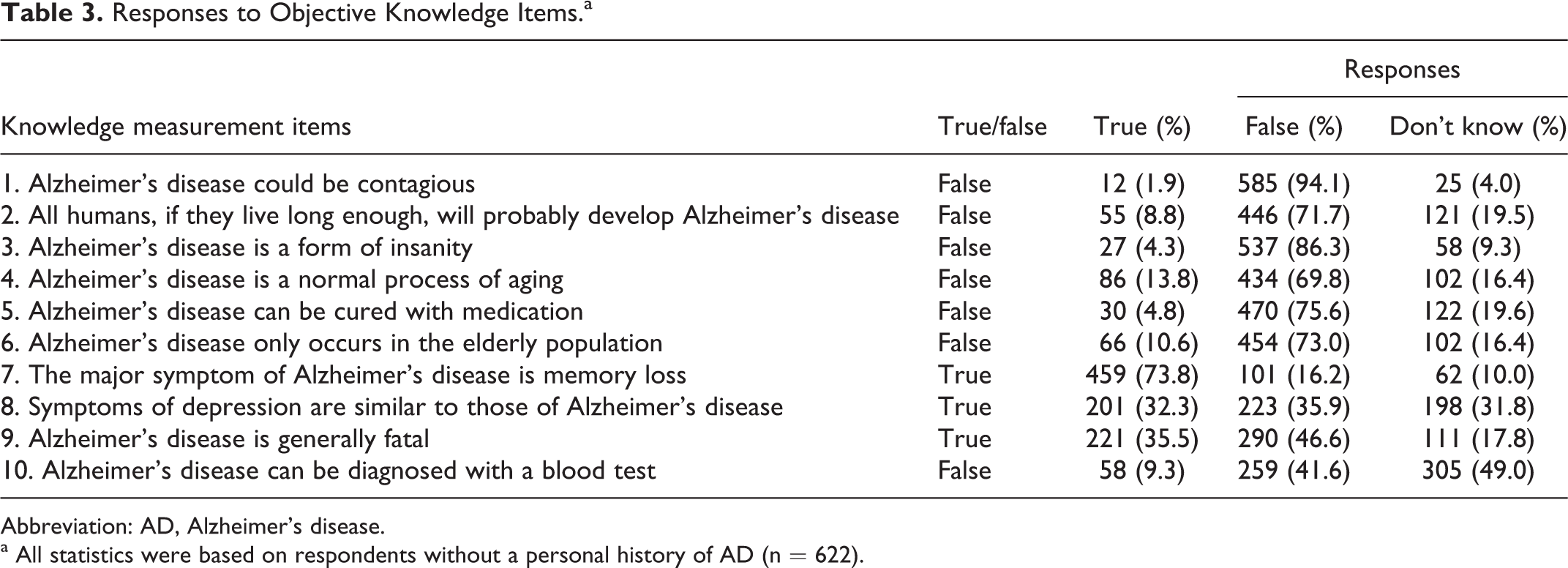
Abbreviation: AD, Alzheimer's disease.
a All statistics were based on respondents without a personal history of AD (n = 622).
Direct-to-Consumer Advertising and Objective Knowledge
Another research objective was to examine the relationship between DTCA exposure and seniors’ objective knowledge of AD. This question was first addressed by regressing the objective knowledge rating on the same set of independent and control variables that were used in Table 2. The results indicated that DTCA exposure did not significantly contribute to seniors’ overall objective knowledge of AD. In fact, the relationship was close to zero (β = −.004, P > .95). Three correlates were significant predictors of overall objective knowledge. Educational level (β = .09, P < .05), household income (β = .10, P < .05), and caretaking experience (β = .11, P < .05) were all positively associated with overall objective knowledge. Noticeably, although subjective knowledge had a wide range of significant predictors, only 3 correlates were significantly related to objective knowledge.
Direct-to-Consumer Advertising and Knowledge of Specific Features of AD
The measurement items of objective knowledge pertained to various features of AD. Therefore, one could argue that although DTCA exposure was not associated with seniors’ overall objective knowledge of AD, it could still influence their knowledge of specific features of AD. To examine this question, a logistic regression model was constructed for each knowledge measurement item with the same independent and control variables. For each statement, responses were recoded as “correct” (ie, recognizing a true statement as true or a false statement as false) and “not correct” (ie, not recognizing a true statement as true or a false statement as false). Next, a logistic regression model was used to examine whether DTCA exposure significantly predicted the likelihood that seniors would correctly recognize a statement’s truth or falsity. This process was repeated for all 10 items.
Of all 10 statements about various features of AD, exposure to DTCA significantly predicted the likelihood that seniors would recognize the truth or falsity of the following 2 statements: “All humans, if they live long enough, will probably develop Alzheimer’s disease” and “Symptoms of depression are similar to those of Alzheimer’s disease.” Table 4 summarizes the results of the logistic regression for the false statement “All humans, if they live long enough, will probably develop Alzheimer’s disease,” with all statistics representing the final model. As shown in Table 4, exposure to DTCA significantly predicted the likelihood that seniors would correctly identify the falsity of the statement (B = −.22, standard error [SE] = .099, P < .05). It was important to note that the coefficient was negative, indicating that seniors who were more frequently exposed to DTCA for AD medicine were less likely to recognize the falsity of the statement. Neither general media exposure nor life experience-related correlates significantly predicted the likelihood of recognizing the falsity of the statement.
Logistic Regression for Knowledge Measurement Item 2.a,b
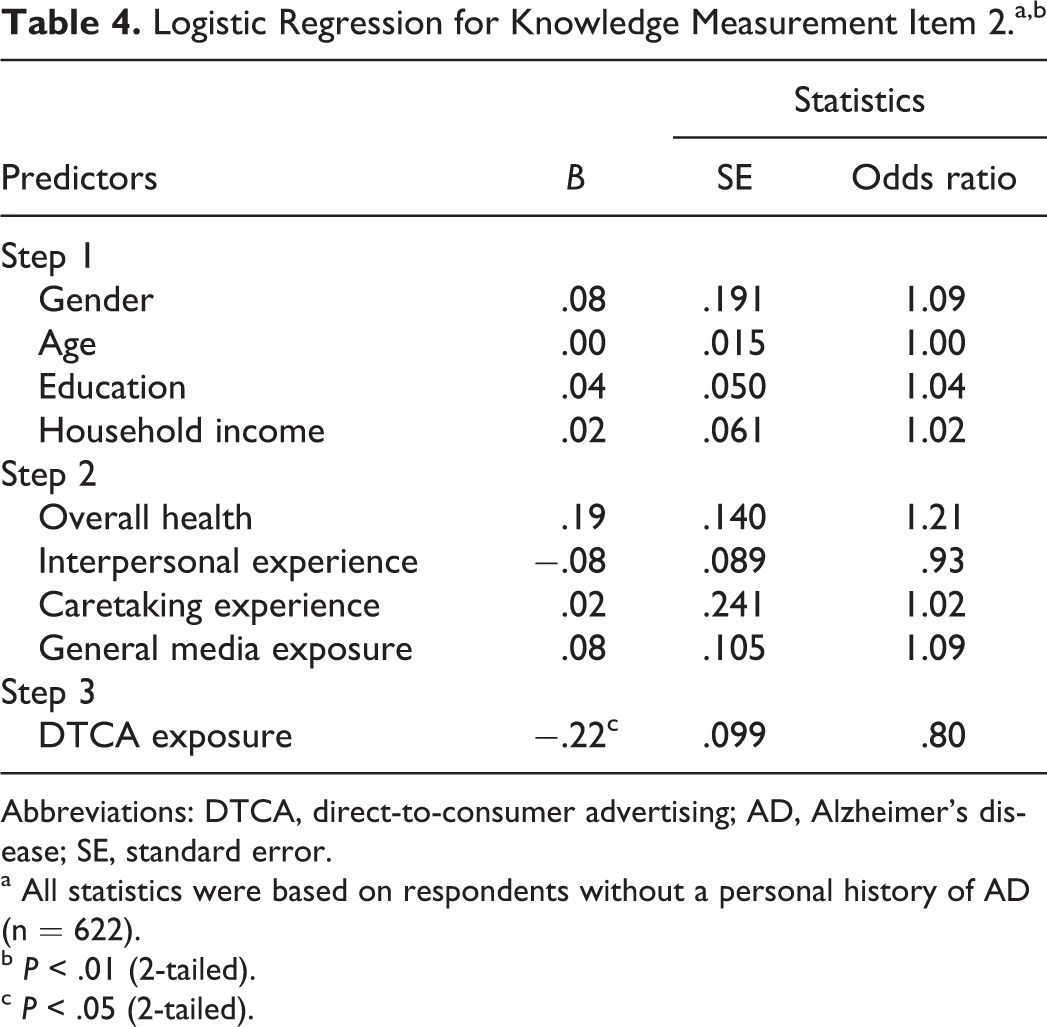
Abbreviations: DTCA, direct-to-consumer advertising; AD, Alzheimer's disease; SE, standard error.
a All statistics were based on respondents without a personal history of AD (n = 622).
b P < .01 (2-tailed).
c P < .05 (2-tailed).
As shown in Table 5, DTCA exposure positively predicted the likelihood of recognizing the true statement “Symptoms of depression are similar to those of Alzheimer’s disease” to be true (B = .19, SE = .095, P < .05). The positive coefficient indicated that seniors who were more frequently exposed to DTCA for AD medicine were more likely to recognize that the statement was true. Again, no other variables were significantly associated with the likelihood of providing the correct response. The results for the 2 statements not only confirmed that objective knowledge is minimally affected by demographic, life experience, and general media exposure factors but also verified that DTCA has the potential to facilitate or inhibit seniors’ knowledge of specific features of AD.
Logistic Regression for Knowledge Measurement Item 8.a,b
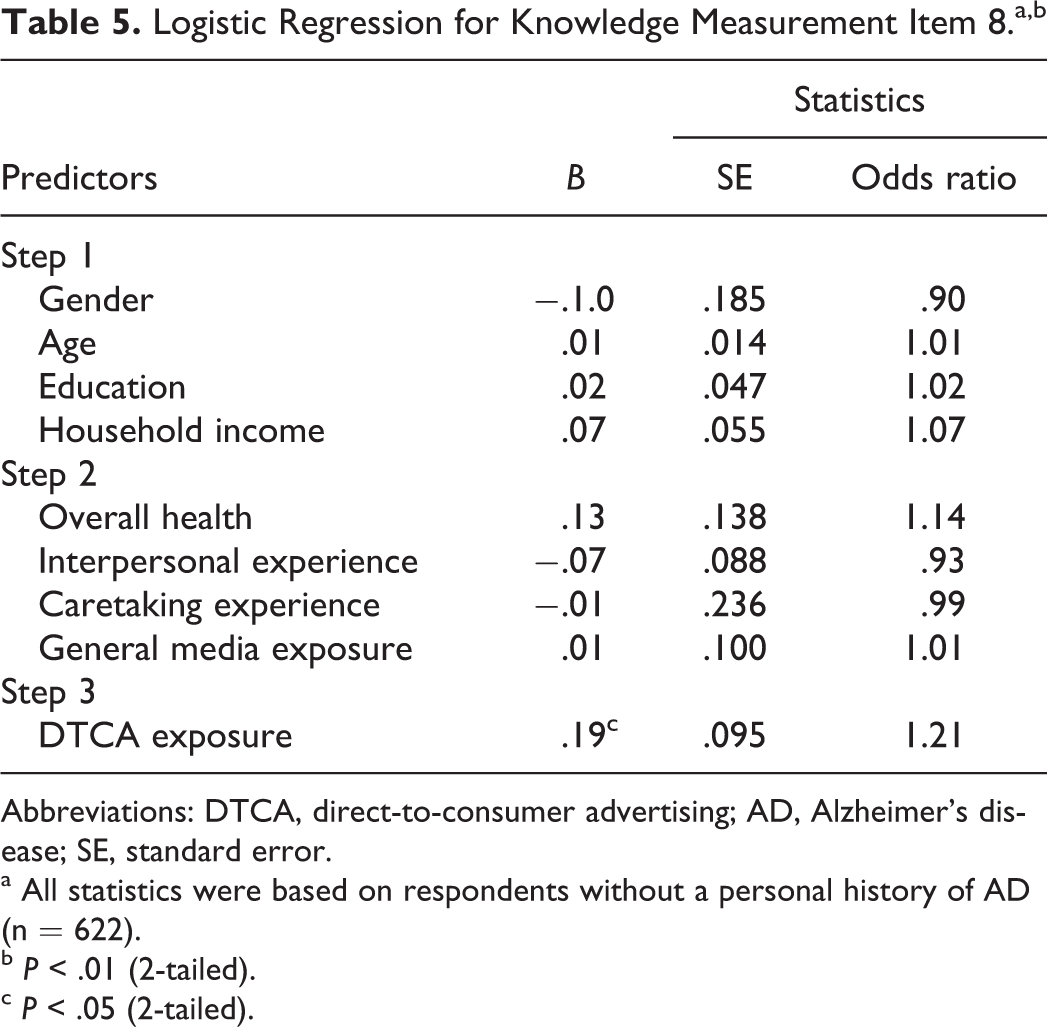
Abbreviations: DTCA, direct-to-consumer advertising; AD, Alzheimer's disease; SE, standard error.
a All statistics were based on respondents without a personal history of AD (n = 622).
b P < .01 (2-tailed).
c P < .05 (2-tailed).
Discussion
Although early detection and professional intervention are critical in managing AD, a substantial lag often exists between the onset of the disease’s early symptoms and the time of professional intervention. 25 What prevents at-risk individuals from seeking professional help? Research suggests that inadequate knowledge is one of the barriers that inhibit individuals from seeking help to address their health problems. 18 Lack of knowledge may be an especially serious impediment for diseases such as depression and AD, whose early symptoms are often difficult to discern because they may not be acute or physically manifested. For example, people may confuse early symptoms of AD with the mild impairments in cognitive functioning that are a normal part of aging. Therefore, one may be aware of deteriorating memory and reasoning but choose not to discuss the problem with a doctor. 26
Direct-to-consumer advertising expenditures for AD medicine have increased rapidly in the United States over the past several years, with US$77.8 million spent in 2012, representing an increase of approximately 150% from 2007 expenditures. 27 This change signals that seniors in the United States are being increasingly exposed to advertising messages for AD medicine. Direct-to-consumer advertising for AD medicine presents both information for consumer education and emotional appeals to persuade current and prospective patients to seek professional help. 11 What would be the net effects of such content in terms of educating individuals about AD?
According to national surveys, people typically believe that DTCA improves their understanding of health problems and treatments. 5,28 However, the current study found that although DTCA may increase seniors’ subjective knowledge of AD, its relationship with their overall objective knowledge is minimal. That is, although DTCA can induce seniors to “feel” knowledgeable about AD, such advertising may not result in an equivalent increase in actual knowledge of the disease. This outcome may be cause for concern, given that an optimum correspondence between perceived and actual knowledge is desirable. 29,30
Another important finding is that although DTCA exposure may enhance seniors’ knowledge of a certain feature of AD (eg, similarities between the symptoms of depression and those of AD), it can also fuel misperceptions (eg, the idea that all people will develop AD if they live long enough). Such misperceptions may support critics’ opinion that DTCA has limited educational value. The finding has implications for improving doctor–patient interactions. For example, a doctor may encounter a patient who believes that all humans will develop AD if they live long enough. If the doctor finds that such misperceptions preclude an effective interaction with the patient, then he or she may consider that exposure to DTCA may have contributed to the patient’s erroneous belief. Accordingly, it may be necessary to remind patients that although DTCA delivers important and potentially useful health information, it does not necessarily increase their knowledge.
Given the importance of knowledge in the management of health issues, it is crucial to explore the factors that contribute to public knowledge of diseases and treatment options. Research suggests that health beliefs are shaped by a range of factors, such as personal history with the disease, 31 general health status, 32 and interpersonal experiences with the disease. 8 Because DTCA has emerged as a major source of health information in the United States, 33 the current study aimed to provide insight into its role in forming individual health knowledge of AD. Although the literature abounds with research on the public’s awareness, attitudes, and perceptions of the value and social consequences of DTCA, 16,17,34,35 this study represents the first scholarly inquiry into DTCA’s potential effects on the subjective and objective knowledge of a disease.
It is also important to note that the current study focused specifically on seniors and their knowledge of AD, a disease that seriously affects their quality of life. A body of existing research has investigated seniors’ views of DTCA’s informational value 17 and social consequences. 35,36 Hall and Jones 10 investigated the effects of advertising message strategies in DTCA for AD medicine on how consumers in Australia evaluate various features of such advertisements, such as the adequacy of the information provided and the ease of processing that information. To the best of the author’s knowledge, this study is the first scholarly inquiry into the potential role of DTCA in shaping US seniors’ knowledge related to AD. Thus, the current study represents a much-needed advance in research.
Despite its contribution, this study has several limitations that should be addressed in future research. First, although this study offered a possible causal interpretation of the observed association between exposure to DTCA for AD medicine and seniors’ knowledge of the disease, a survey study cannot establish causality. To enhance the validity of the causal interpretation, the current study controlled for a wide range of potential correlates (such as interpersonal experiences with AD and exposure to general, nonadvertising media coverage of AD). However, an experimental design allowing for a causal interpretation is recommended for future research to further validate the findings of the current study.
Another limitation to be noted is that only 2 of 10 statements measuring objective knowledge of AD yielded significant results. The other 8 items provided no significant results. Therefore, one should not overlook the possibility that the statistically significant results were merely coincidental, rather than providing solid evidence for the supposed effects. A related issue is that objective knowledge of AD could have been measured in several different ways. The current study employed the scale developed by Jang, Kim, and Chiriboga 21 based on the notion that its measurement items are appropriate for nonprofessional samples. Future researchers may explore if the results might vary if knowledge is measured with more comprehensive and thoroughly validated scales 37,38 that include measurement items designed for health professionals as well as the general public.
The recent growth in DTCA expenditures for AD medicine signals that seniors in the United States will be increasingly exposed to the stories that pharmaceutical companies tell about AD. However, it was beyond the scope of the current study to specify the full range of content elements provided by DTCA for AD medicine. Research suggests that although DTCA typically provides information on the symptoms of a disease, such advertisements rarely communicate other important features, such as the cause, risk factors, and prevalence of the disease. 39 This lack of information may explain why DTCA exposure had a minimal effect on seniors’ overall objective knowledge of AD in the current study although the effect for one of the measurement items pertaining to the symptoms of AD was statistically significant. To further explore this line of thinking, future research may employ a design that can attribute the knowledge-enhancing (or inhibiting) effects of DTCA to specific content elements that are strategically placed in DTCA.
Finally, response rates varied across the demographic subsegments of the consumer panel; therefore, the demographic characteristics of the sample diverged from the population of US seniors. For this reason, one should be cautious in interpreting the findings of this study. Future researchers are encouraged to address this limitation with a nationally representative sample, as knowledge of AD is known to vary across ethnic groups. 31,40
Conclusion
In the United States, patients are assuming an increasingly active role in managing their health problems. 4 Direct-to-consumer advertising encourages individuals to visit a doctor to discuss their medical conditions and to ask for specific types of prescription medicine. 2,3 Thus, to communicate with potential patients of AD more effectively, health professionals may need to consider patients’ level of subjective and objective knowledge of the disease and explore what may have contributed to that knowledge. For both doctors and patients, the findings of the current study imply that although people may feel more knowledgeable about AD as a result of their cumulative exposure to DTCA for AD medicine, the influence of DTCA on what people actually know about the disease may not be as strong.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.