
Abstract
Background: Some authors suggest that besides the fundamental components, cognitive reserve (CR) also reflects the influence of a combination of factors that improve mental health. Method: After obtaining the sociodemographic profile of each participant and evaluating their neurologic and neuropsychologic abilities, first, homogeneity analysis was used as a technique to select variables and reduce the number of categories with similar behavior; then CR construct was identified through a latent class analysis model. It was then possible to categorize participants according to their level in this construct and compare the neuropsychological performance of the subgroups that emerged, using a t test of differences of means for independent samples. Results: Participants with Alzheimer’s disease with low CR scores exhibited significantly greater deficits in measures of memory, attention, and language than patients with high CR. Conclusions: Our results ratify the effect of higher education, higher professional performance, and ludic activities on CR.
Introduction
At present, the study of cognitive reserve (CR) is moving toward a more integral approach in which a set of different factors is thought to contribute to an individual’s final reserve, each factor making an individual contribution. These factors include innate capabilities, the socioeconomic circumstances surrounding childhood, education, occupation, and the leisure activities engaged in at a more advanced age. It is important that CR be understood not as a stable situation but rather as something dynamic that changes over the course of one’s life.
It has been suggested that CR is a mechanism that links low educational levels with a greater risk of suffering a neurodegenerative process. Cognitive reserve, or the ability of the brain to better tolerate the effects of a pathology associated with dementia, may be the result of an innate ability or the effect of life experience, such as level of education or occupation. 1,2 In this vein, CR is considered an active mechanism based on the application of resources learned as a result of a good education, profession, or premorbid intelligence. 3 –6
Alzheimer’s disease (AD) is a good model for demonstrating the CR hypothesis and is also a pathological process affected by numerous causes; on one hand, there are genetic factors, and on the other, there are nonhereditary factors that are the result of environment and lifestyle. The cause of this process can perhaps be found in the interaction among genetic, environmental, and behavioral factors, which modulate and modify each other. Each of these factors can protect from, facilitate, or even accelerate the course of the disease. 7 –10
A low level of intelligence may act as a risk factor, since diverse epidemiological studies have shown that populations having an IQ below the average (100 ± 15) are more likely to suffer from AD. 11 –13 The hypothesis that a higher educational level can protect against dementia has been studied by many authors. 7,14,15
Low educational level is not the only variable intervening in the appearance of dementia. Studies have been carried out, which associate dementia with another type of socioenvironmental factor such as place of residence 16 or the degree of social relationships, both as regards quantity and level of satisfaction. 17 –19 These social relationships would increase CR by demanding the participants a greater and more efficient communicative capacity as well as participation in complex tasks that demand the implementation of cognitive resources and capacities. 20
According to authors such as Moceri et al, 21 Feinstein, 22 and Gatz et al, 15 coming from a large family or having unskilled parents, together with the social class to which they pertain, poses a risk of AD, most likely because these circumstances are associated with less favorable conditions (health, nutrition, etc).
A person’s degree of activity and social relations, as well as life interests, have also been studied in relation to both risk and protective factors. 23 For this author, a low level of physical activity can be considered a risk factor.
Numerous factors affect the development and trajectory of cognition in the long run. Besides genetic determinants and prenatal exposure, early influences include birth order, 24 material domestic conditions, 25 the encouragement or support of parents, 26 physical growth, 27 and physical health. 28
The factors associated with cognitive benefits during maturity include physical activity, 29 –33 nutrition, 34 –38 social and intellectual commitment, 39 –43 reading, 44 or any other type of cognitively stimulating activity. 45 ,46 Taking into account all the above factors, Katzman 24 considers that they follow a specific order in time, in which genetic conditions intervene first, then early exposure, and finally factors related to adulthood that can delay the clinical expression of the disease.
To conclude, some authors 4,5,47 suggest that besides the fundamental components of parental environment, intelligence, and educational achievements, CR also reflects the influence of a combination of factors that improve mental and physical health, and that in turn increase and maintain neural integrity. Thus, instead of being a phenomenon that remains stable during development, CR represents a dynamic process that evolves with age and has crucial implications for cognitive function in the later stages of life. 8,48
The main objective of this research is to contribute to a more in-depth knowledge of the CR construct. With this goal in mind, we study the different fundamental components described above in an attempt to find whether combinations of them can intervene as underlying factors of CR, assessing the explanatory power of each of these elements on a sample of Spanish individuals with Sporadic Late Onset Alzheimer Disease (SLOAD).
Participants and Methods
Participants
The sample used in this study comprised 112 participants who were divided into 2 groups; one group of 74 participants were diagnosed with SLOAD and another group of 38 participants who at the time of examination were carefully screened to exclude those with dementia or any other medical conditions that would affect their neuropsychological performance. The following exclusion criteria were considered: (a) a history of neurological disorders, (b) visual and auditory noncorrected deficits, (c) a history of abuse or dependence on alcohol or other drugs, and (d) a score lower than 28 on mental status: Mini-Mental State Examination (Folstein); adaptation by Lobo et al. 49 Information about the relatives was obtained through a semistructured interview.
The participants with SLOAD were selected in the Neurology Service of the University Clinical Hospital of Salamanca. The participants in the control group were selected from among the individuals accompanying the patients on their visits to this service who fulfilled the necessary inclusion criteria. All the participants signed and informed consent form.
To be included in the clinical group, the participants had to satisfy the following criteria: (a) neurological and neuropsychological diagnosis of AD according to Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition [DSM-IV]) criteria (American Psychiatric Association, 50 (b) cutoff age of 60 in order to differentiate between early and late onset according to parameters established by the researchers and based on the observations of early and late presentation in the population studied by the group, and (c) the criteria of the National Institute of Neurological and Communicative Disorders Association–Alzheirner's Disease and Related Disorders Association (NINCDS-ADRDA) group for the diagnosis of probable or possible AD. 51
We decided to consider both the groups of criteria for the diagnosis (DSM-IV) and classification (NINCDS-ADRDA) of AD, since besides being the ones most used internationally for clinical diagnosis of dementia, they show a high sensitivity (81%) and an acceptable level of specificity (70%) for AD. 52
From the methodological point of view, the study was carried out in several stages. In the first stage, patients who presented in the Neurology Service and expressed subjective complaints about memory were evaluated by neurological examination and neuropsychological assessment. After 6 months, the patients were again evaluated, enabling us to include patients in the category of probable AD. However, only the data obtained in the first evaluation were used in this research study.
For the participants with SLOAD, diagnostic tests were used in order to exclude those individuals with possible secondary dementia. Included in these tests were: thyroid function, luetic serology, levels of vitamin B12, and folic acid.
All the participants with SLOAD were examined neuroradiologically by computed tomographic scans. According to the neuroradiological reports, all the participants included in the clinical sample showed structural lesions consisting of the presence of different degrees of cerebral atrophy, mainly cortical.
Procedure
The evaluation of each participant in the clinical group consisted of a full neurological examination performed at the Neurology Service of the Clinical Hospital of Salamanca, a semistructured interview on sociodemographic and clinical aspects, a neuropsychological evaluation with a battery of tests designed for this study and an assessment of mood with the Beck Depression Inventory. 53 Interviews and neuropsychological testing were conducted in Spanish.
Sociodemographic and Clinical Evaluation
Each patient and each participant in the control group was interviewed in a semistructured way in order to obtain enough information to draw up a sociodemographic profile of each. The interviews were then transcribed and their content was analyzed in order to obtain the data of interest. Based on this data, each participant was then classified within a previously designed category system according to whether they fulfilled the preset requirements or not.
Likewise, information was also gathered in the interview regarding medical, neurological, and psychiatric variables, which was then contrasted and expanded by consulting the hospital clinical record where the participant had been selected. The main purpose of this register was to establish a control over these variables and at the same time guarantee a thorough description of the sample. Nevertheless, certain variables showed a high rate of nonresponse, a possible explanation for which is the following: some of the factors considered refer to information outside the participant’s own life cycle (eg, the educational level of the participant’s father) and it is possible that the participant did not know or remember such information. There were also other variables, related to the participant’s involvement in leisure activities (social or intellectual activities and reading), for which the categorization of information required a certain level of operationalization that some participants were not able to attain. This situation occurred most strikingly in patients with a certain degree of cognitive deterioration whose capability for analyzing and organizing information was diminished. An evaluation of manual dominance was also included, using the Edinburgh Laterality Inventory. 54
Factor Scores: Cognitive Reserve
Table 1 shows the variables studied for the classification of the participants into high or low reserve. The variables parents’ health, quality living accommodations during the participant’s childhood and youth, and parents’ support were eliminated from the analyses owing to a high level of nonresponse (80%). The variable “linguistic environment” was also eliminated since all the patients gave the same response.
Parental, Family, and Patient Influence Variables and Their Categorizations a
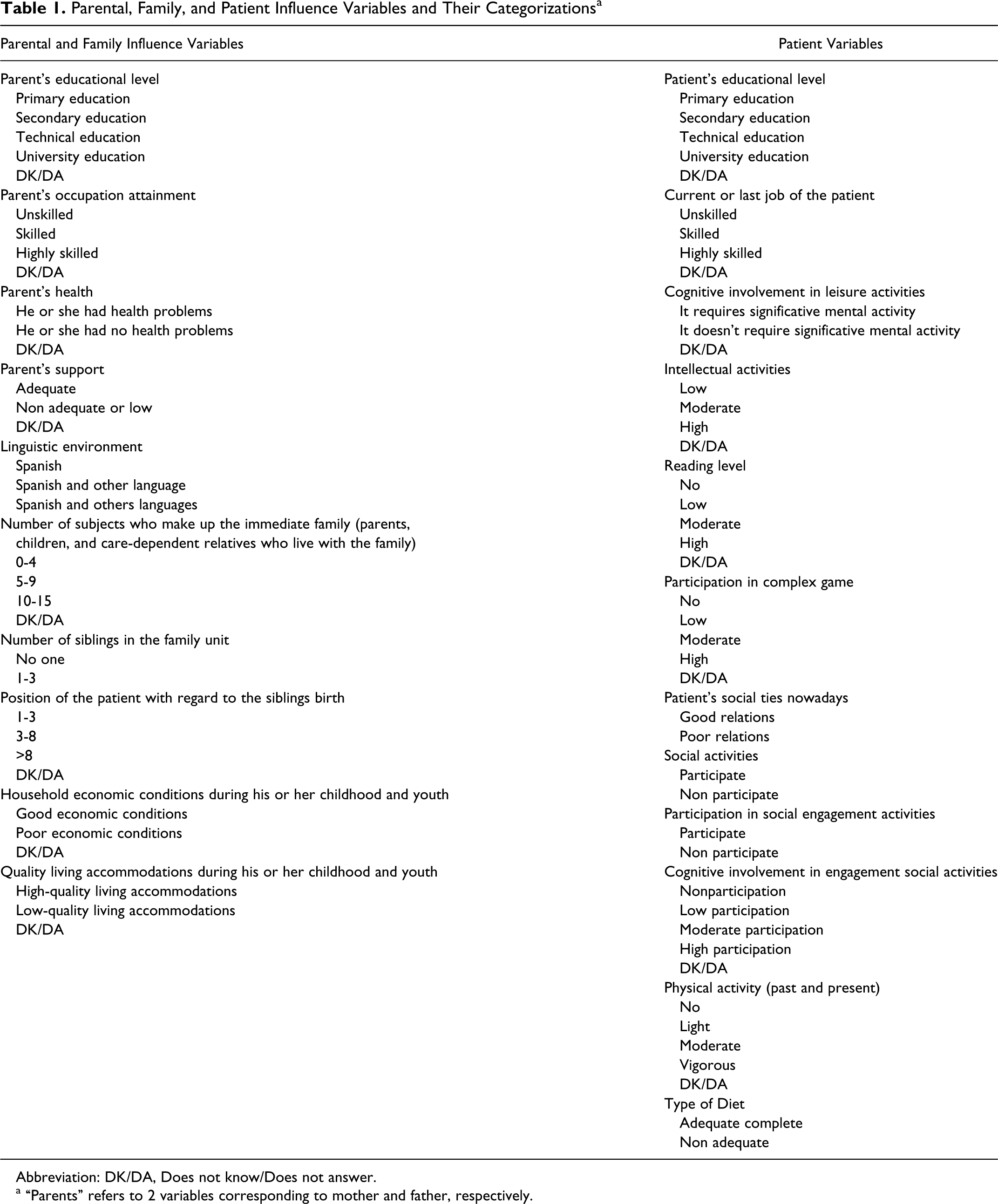
Abbreviation: DK/DA, Does not know/Does not answer.
a “Parents” refers to 2 variables corresponding to mother and father, respectively.
Neuropsychological Evaluation
The tests comprising the neuropsychological examination battery designed for this study were selected for their validity and because they had been shown to be sensitive to neuropsychological deterioration in patients with AD.
Neuropsychological Testing
Mental Status: Mini-Mental State Examination (Folstein). Adaptation by Lobo et al 49
Intelligence: Wechsler Adult Intelligence Scale (Third Edition; WAIS-III). 55
Memory: Wechsler Memory Scale (WMS-III), 56 WAIS-III: Digit Span, 55 and Remote Memory.
Attention: WAIS-III: Digit Span, 55 Stroop Color–Word Test, 57 Trail Making Part A and Part B, 58 and Letter Cancellation Test.
Language: Boston Naming Test, 59 Controlled Word Association Test, 60 Semantic Verbal Fluency Test (Animals), and Phonemic Verbal Fluency Test (P/M/R).
Visuospatial, Visuoconstructional, and Visuoperceptual Abilities: WAIS-III: Block Design, 55 WAIS-III: Object Assembly, 55 and Facial Recognition. 61
Executive Functions: Wisconsin Card Sorting Test, 62 Trail Making Part A and Part B, 58 and Stroop Color–Word Test. 57
Emotional Status: Beck Depression Inventory. 53
Statistical Analyses
Given the high number of social-type categorical variables and the number of categories in each variable, it was impossible to use a model to identify the CR construct owing to the high number of parameters to be estimated in relation to the number of patients included in the study. Therefore, Homogeneity analysis (HOMALS), 63 also known as multiple correspondence analysis, was used as a technique to select variables. The objective of this analysis was to identify a space of a few dimensions or factors that will allow us to summarize and represent the structure of associations in a determined group of categorical variables. Thus, with this analysis, we sought the set of homogeneous variables to classify (or for classifying) patients. Once HOMALS was applied, we obtained the representation of the individuals and the categories of different variables in a single space. In this way, the proximities or distances of the points allow us to see the similarities among the individuals and the associations among the variables; when the points of the categories of the same variable are close together, it indicates that their behavior is similar in relation to the individuals. This feature also enabled us to reduce the number of categories when their behavior was similar. The variables to be included in the latent class analysis were chosen by means of discrimination measures, which provided us with a measure of the contribution of each variable to the shaping of the dimensions that best discriminate the individuals. We chose the variables that contributed most to the first dimension, which is the one that explains the most variability.
In the homogeneity analysis, the category “Does not know/Does not answer (DK/DA)” was eliminated because the variables could be grouped by the lack of response, which was not of interest for the objective of this analysis.
Latent class analysis 64 was used to identify the CR construct. The latent class model is a technique that enables us to study the existence of one or several latent variables based on a set of observer (manifest) response variables. This technique is considered more suitable given the categorical nature of the manifest variables considered important in the definition of CR.
The first step in this analysis is to choose the number of classes or categories comprising the latent variable. We assessed the number of classes in the model by means of a likelihood test. The fitted model is the one that shows the greatest decrease in the likelihood test. Several tests exist to identify the number of classes in a latent variable. The method used in our study was the Bayes Information Criterion (BIC). 65 The CR status of each class was obtained from the probabilities that an individual is in a specified level of manifest variable given a latent class.
The t test was used to compare the high and low CR groups, taking into account whether the population variances were equal or not. These statistical tests were carried out in both the experimental and the control groups to compare the differences between means in healthy and unhealthy patients. No adjustment was made for multiple comparisons. Although there is an increase in the Type I risk, subjecting the tests to corrections according to the number of comparisons leads to an important decrease in the power of these tests given the sample sizes. 66 Since the disadvantage of the increase in Type I risk occurs in controls and the group with AD, the results are compared according to the P value and the effect size considered as the difference of means.
Given that the results of some of the tests used in the battery for neuropsychological exploration could not be converted into scalar scores that would eliminate the age effect, analysis of covariance was run to eliminate the effect of this sociodemographic variable.
To assess the impact of multiple comparisons, multivariate analysis of variance ([MANOVA] or multivariate analysis of covariance depending on whether the group of variables are adjusted for age) analysis was carried out for each cognitive domain constituted by several variables such as: ATTENTION, WMS-III, logical memory, WMS word list, WMS-III, Visual reproduction, Language, Intelligence, and Executive Functions. Data were analyzed with LATENTGOLD (version 4.0) and SPSS (version 18).
Results
The inertia absorbed by the first 2 dimensions of the homogeneity analysis is 38.5%, and the degree of homogeneity of the variables is high (Cronbrach’s alpha = 0.77).
The variables chosen to identify the classes of CR are those that have a discrimination value higher than 0.3 (Figure 1 ). This cut-off was chosen because it is where the largest decreases in discrimination values occurred.
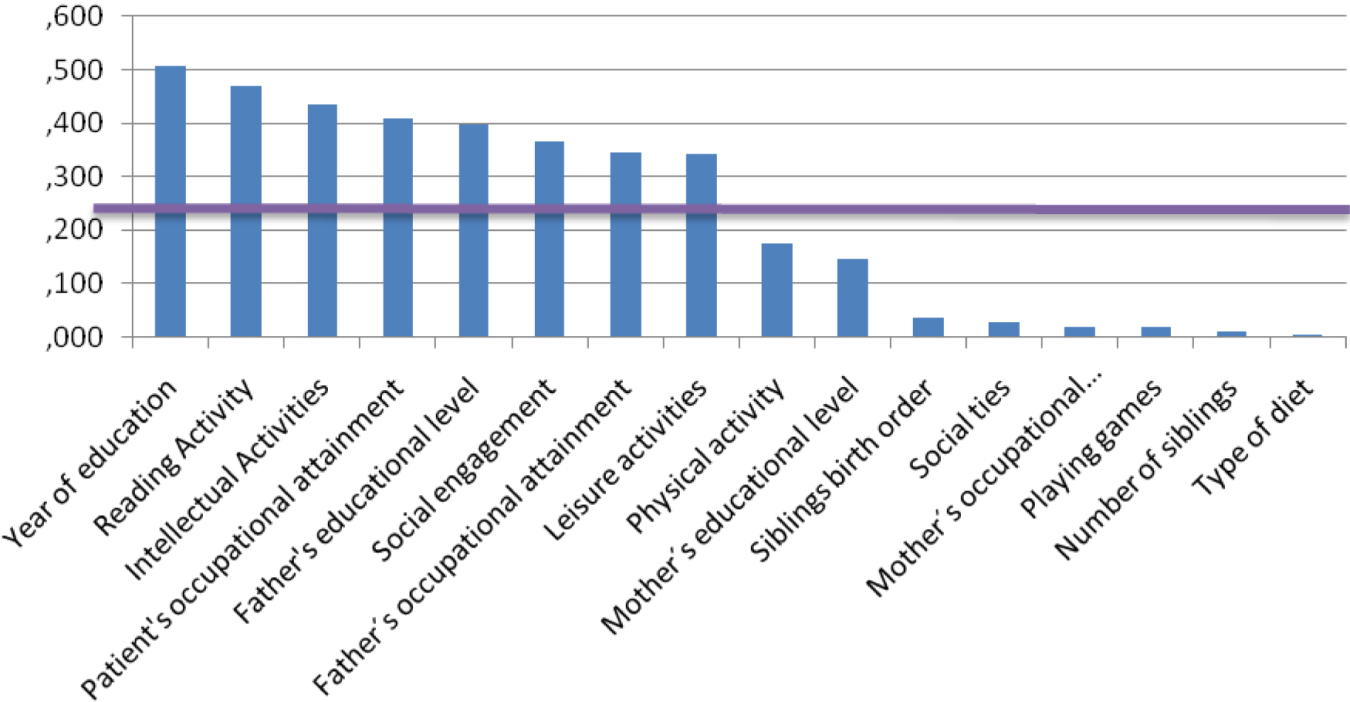
Discrimination values of the homogeneity analysis variables for the first factor.
In a second step, we analyzed the possibility of reducing the number of categories in each of the variables chosen. The grouping was based on the proximity of the points representing the levels of the categorical values in the HOMALS plot (Figure 2 ).
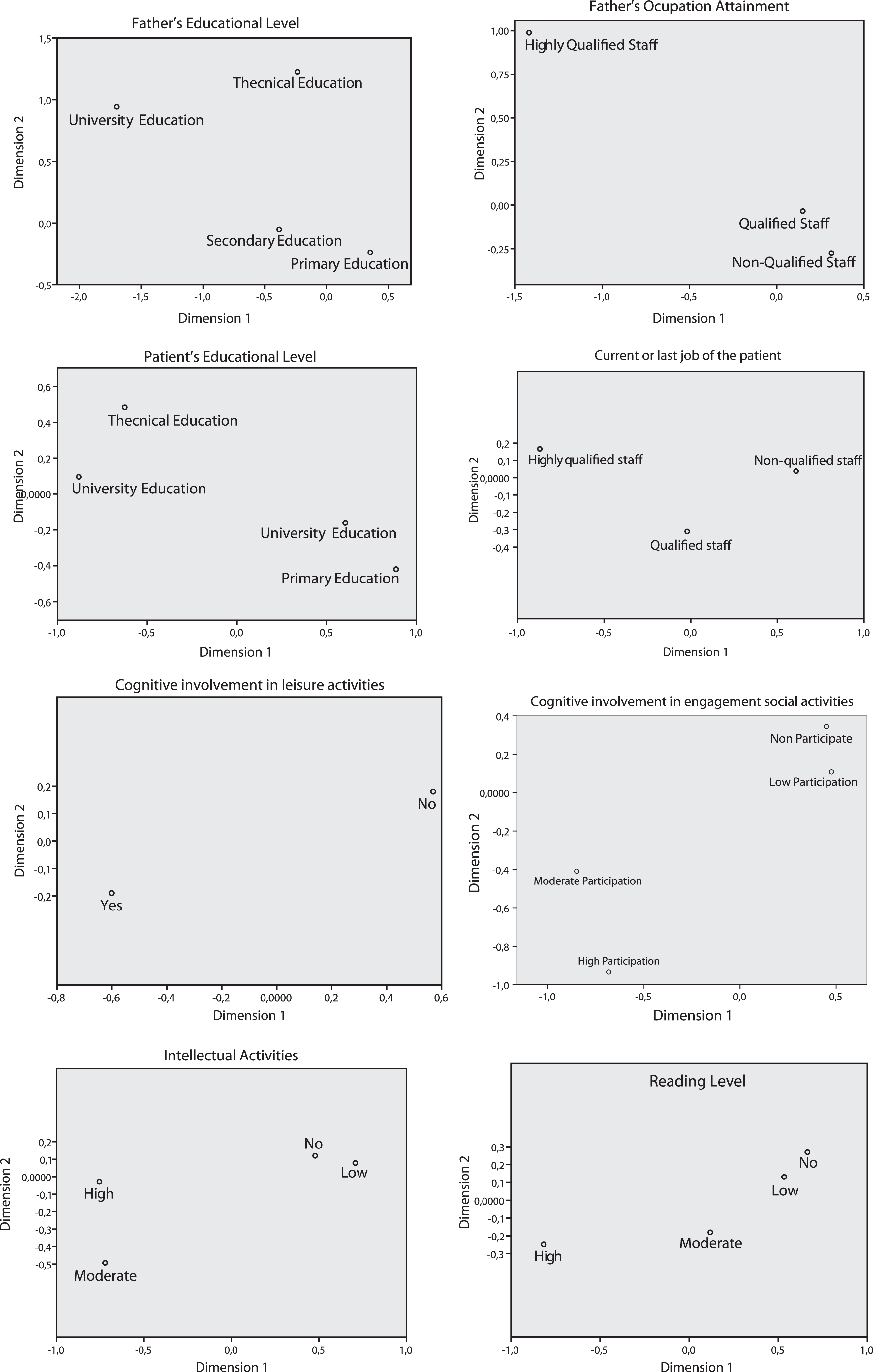
Configurations obtained in the homogeneity analysis for the levels of the variables with the highest discrimination index.
The variables to be used in the latent class analysis are the following: Father’s educational level (DK/DA, Basic Education, Higher Education), Patient’s occupational attainment (DK/DA, Unskilled, Highly Skilled), Patient’s educational level (Basic Education, Higher Education), Patient’s current or last job (Unskilled, Highly Skilled), Cognitive involvement in leisure activities (DK/DA, No, Yes), Social activities (DK/DA, No, low, moderate-high), Intellectual activities (DK/DA, No, Low, moderate-high), and Reading level (DK/DA, No, Low, moderate-high). The control participants and the patients were entered jointly in the latent class model for their subsequent classification according to their CR.
To choose the number of latent classes, we estimated a first model with a latent class as the base model. Starting with this model, the latent classes were gradually increased. We chose the model with 2 classes, since it had the lowest BIC value (Table 2 ). Subsequently, we analyzed the supposition of local independence based on the residuals of paired variables. It was observed that there was local dependence between the following pairs of variables: Years of education and Father’s occupational attainment, Years of education and Patient’s occupational attainment, and Intellectual activities and Leisure activities and Social engagement. Model 5 is the one obtained after adjusting for these local dependencies. The P value of this model is still significant, which means that there is unexplained variability.
Latent Class Models
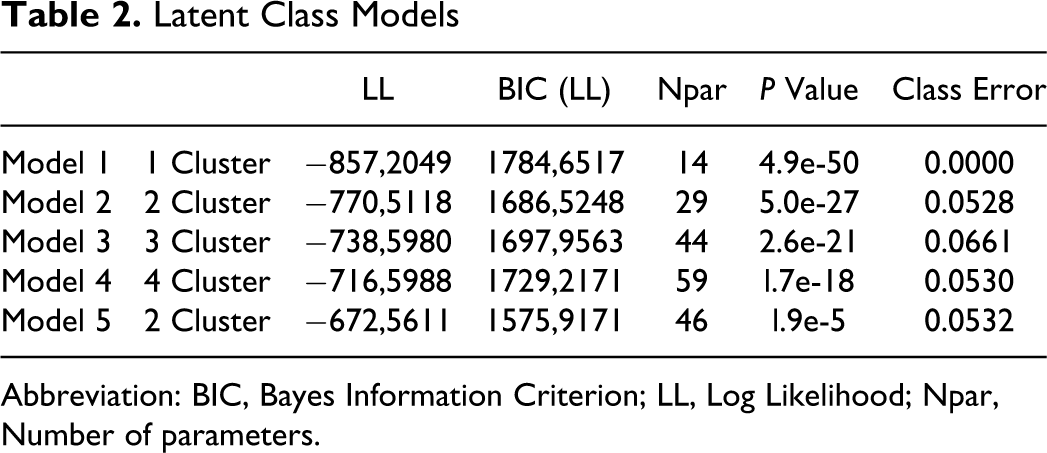
Abbreviation: BIC, Bayes Information Criterion; LL, Log Likelihood; Npar, Number of parameters.
The probabilities of the levels of the manifest variables, conditional on the latent classes, are presented in Table 3 . Based on this information, we can identify the levels of the manifest variables that characterize the 2 latent classes. The first class would be identified by no higher education and low qualifications both on the part of the father and the patient, absent or scarce cognitive implications of ludic and social activities, absent or low intellectual activities and reading. Given the characteristics of this class, we shall call it the low CR class. The second class would be defined mainly by highly cognitive implications, such as high ludic and social activities, high intellectual and reading activities, and higher education, whereas the father’s and the patient’s qualifications and the father’s education would define it to a lesser extent. However, if we compare the probabilities in this class for the high levels of these last 3 variables, it is observed that it is 3 times greater in the case of the father’s education and the patient’s occupation and 6 times greater in the case of the father’s occupation.
Levels of Probability for Observed Variables
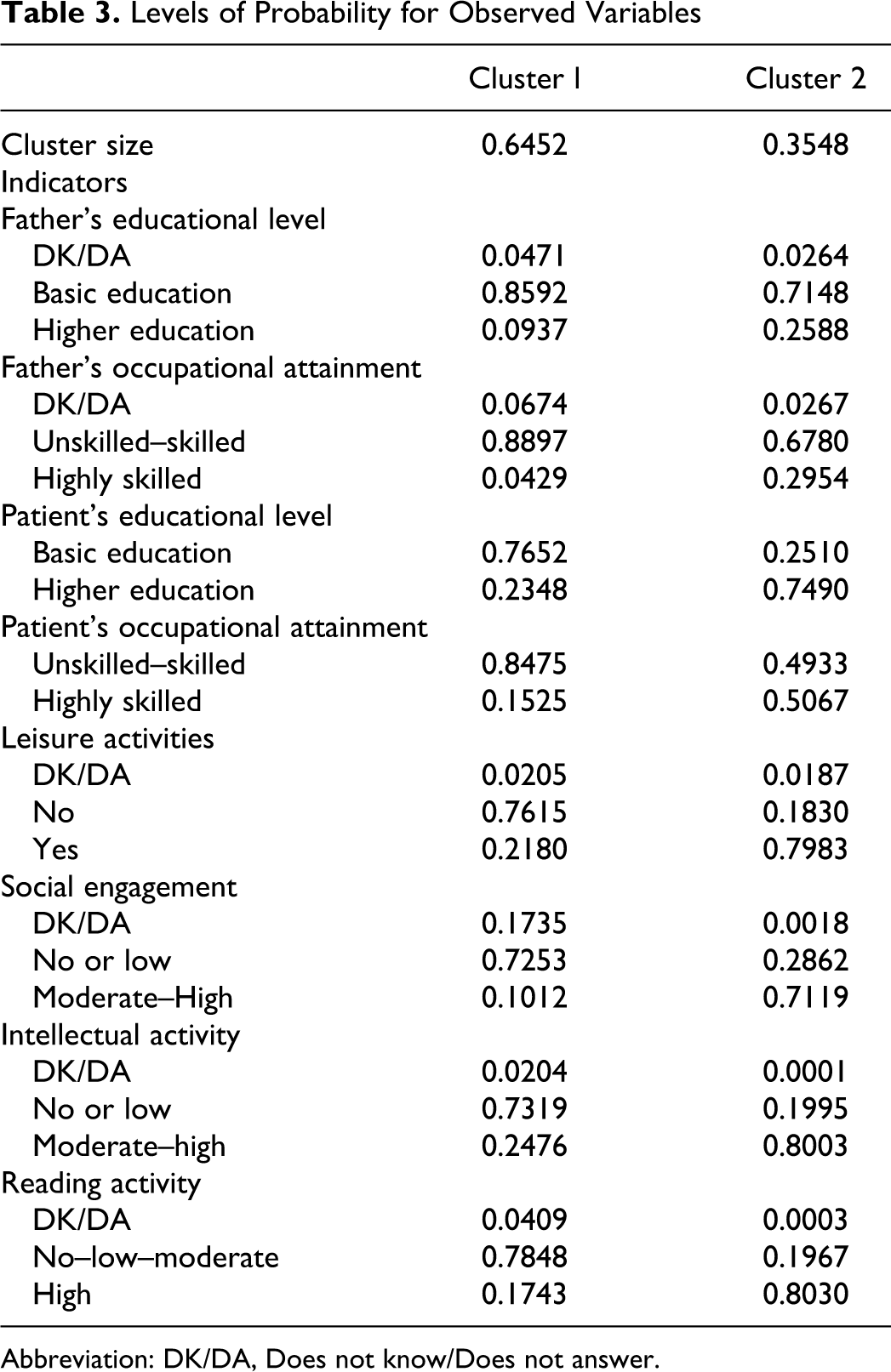
Abbreviation: DK/DA, Does not know/Does not answer.
In Table 4 , we present the results of the t test of differences in means for independent samples between the participants in the control group and the participants with AD, in the different cognitive areas studied. This test was run in order to be able to determine the different cognitive profiles of the 2 groups and the possible existence of significant differences between them. As expected, there were statistical differences between the two groups in the majority of the tests applied, except in resistance to interference in the Stroop Color–Word Test and in the percentage of perseverative responses and nonperseverative errors in the Wisconsin Card Sorting Test.
Independent Samples t Test on Neuropsychology Battery Between Subjects in the Control Group and the Clinical Groupa
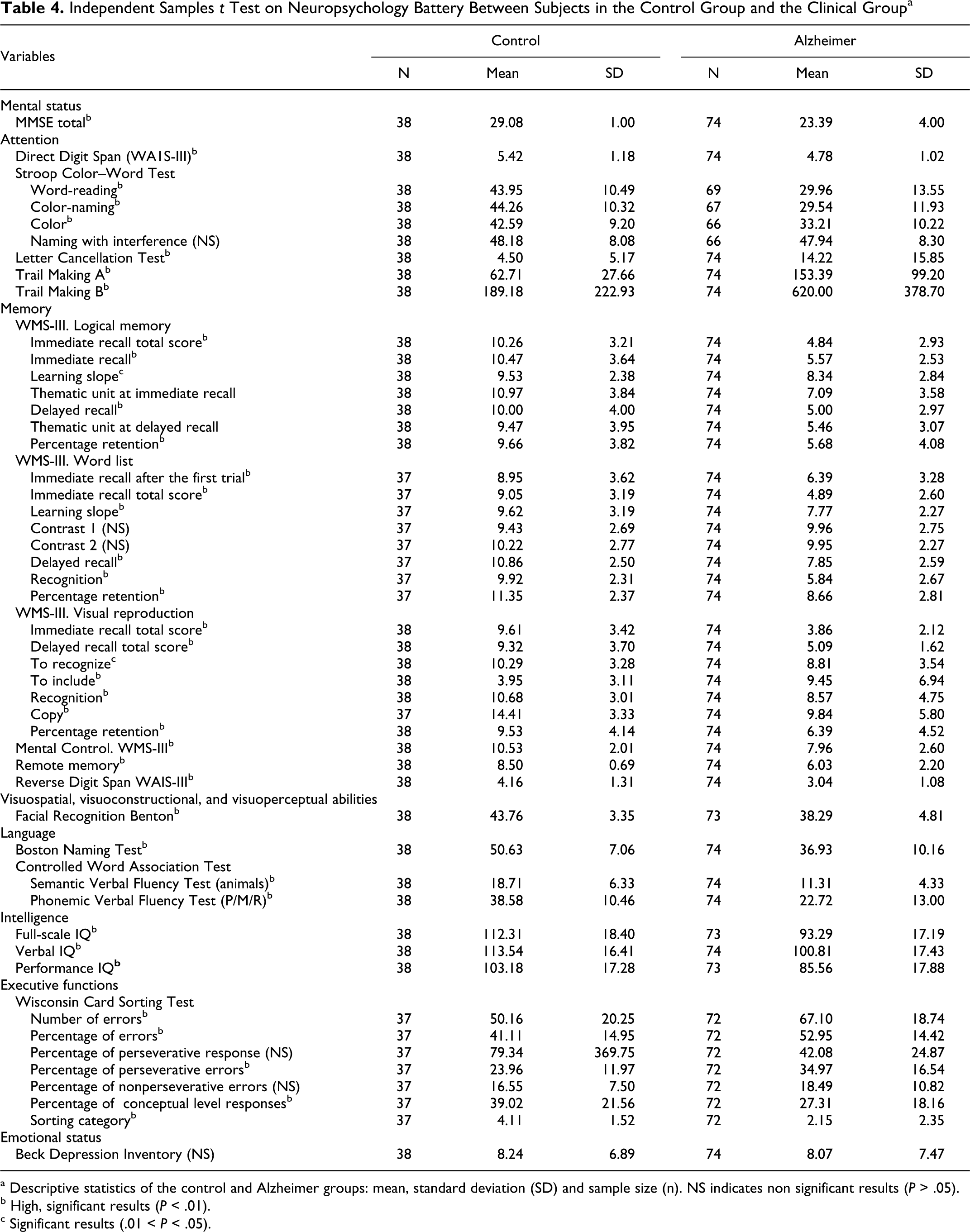
a Descriptive statistics of the control and Alzheimer groups: mean, standard deviation (SD) and sample size (n). NS indicates non significant results (P > .05).
b High, significant results (P < .01).
c Significant results (.01 < P < .05).
We now turn to examining the role of CR. MANOVA results did not detect statistically significant differences in the control group for any cognitive domain. In contrast, in the patient group, differences were detected in the ATTENTION (P = .045) and WMS-III word list (P = .041) groups. In the case of the language domain, the P value was close to significance (P = .08).
Table 5 shows the results of the t test of differences in means for independent samples that was used to determine the possible influence of CR on the neuropsychological performance of the participants in both groups.
Independent Samples t Test for the Groups of High and Low Cognitive Reserve on Neuropsychological Performance of Different Cognitive Functions Assessed in the Clinical and the Control Groups
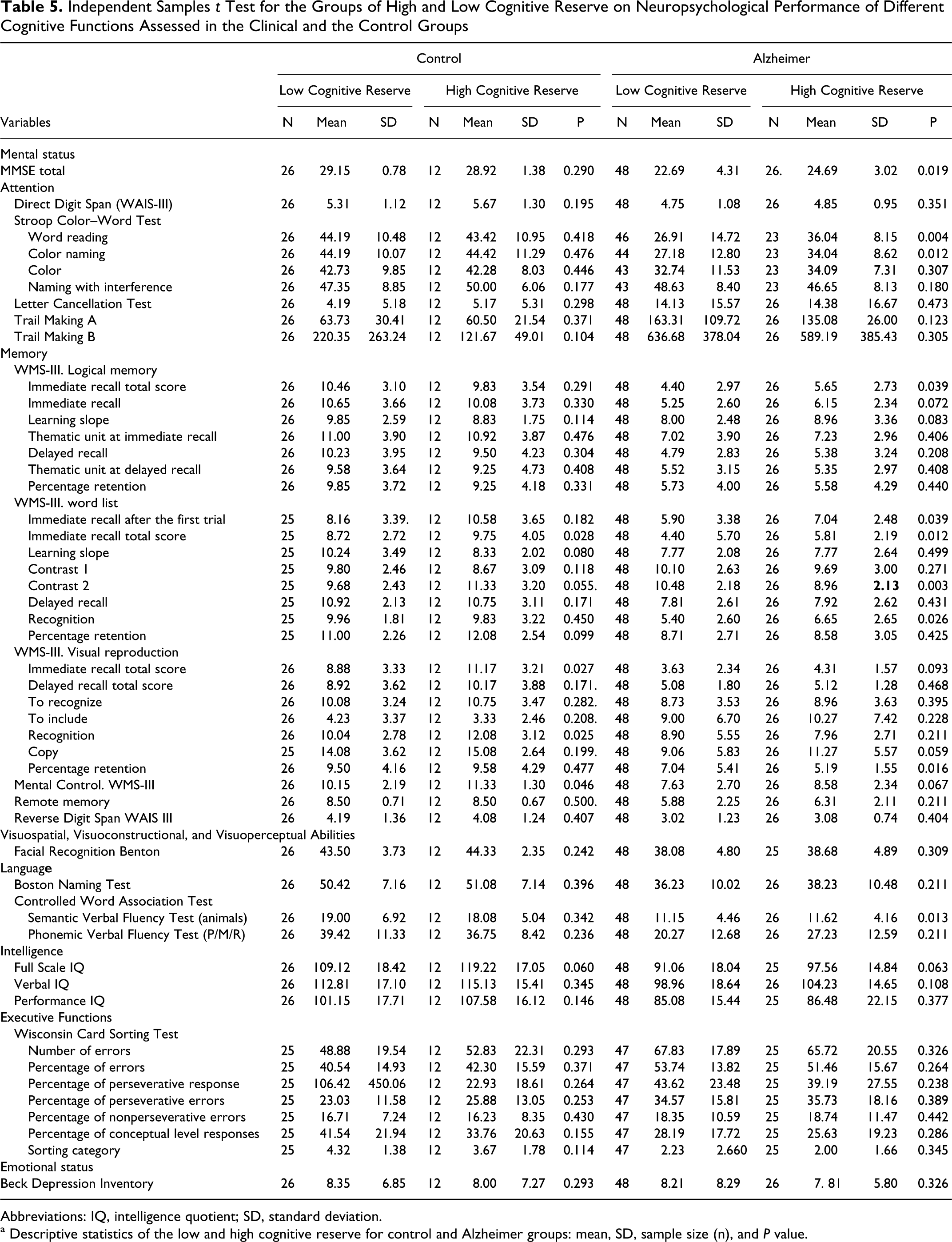
Abbreviations: IQ, intelligence quotient; SD, standard deviation.
a Descriptive statistics of the low and high cognitive reserve for control and Alzheimer groups: mean, SD, sample size (n), and P value.
In the group with AD, the results show the existence of significant differences between the participants with high and low reserve in general cognitive functioning, the group with low reserve showing a slight cognitive deterioration in relation to the group with high reserve.
The results show a greater mnesic alteration in the participants with low CR that mainly affects the immediate recall of verbal material. Moreover, although both groups perform similarly in the coding and recovery of visual material, retention is significantly better in the high reserve group. On the other hand, the neuropsychological tasks that require the linguistic component of verbal fluency reflect significant differences between the low and high CR groups, the participants with low reserve showing a poorer performance.
When attention was assessed, we found significant differences between the low and high CR participants in the results of the tests used, with the low reserve participants performing more poorly in these functions, the same as in the former cases.
Finally, no significant differences were found between the participants with low and high reserve as regards mood assessment.
In the control group (Table 5), there were only significant differences between the scores of the high and low reserve groups in the tests evaluating mnesic functions. We observed a greater alteration in the immediate recall of verbal and nonverbal material in the participants with low reserve, a situation which limits their ability to learn new information. Moreover, the participants with low CR showed a greater alteration in the evocation of automatic sequences.
Discussion
Our results reveal that patients diagnosed with AD who have a high CR attain a higher neuropsychological performance than those with a low reserve. These results show that the considerable intellectual activity delays the onset of AD symptoms in persons with brain damage secondary to the disease. Many authors whom we shall cite below consider that the so-called “cognitive reserve” theory can be applied, which in short means that the stimulation of intellectual activities prepares the brain (like physical activities do for the rest of the organism) to confront the problems that appear when a person is faced with illness, because it “increases” the “adaptive flexibility” of the organ in the face of the possible damage to which it is exposed. Thus, the participants with high CR have gradually developed throughout their lives a large range of cognitive strategies for solving complex problems, and because of this, they have developed a higher number of neuronal pathways for performing these same cognitive processes, making it more likely for them to preserve their cognitive functions despite the deterioration. 4
Manly et al, 1 using a sample of elderly participants without dementia, found that an increase in literacy (probably related to higher quality and access to education) was associated with less deterioration of memory, executive function and language skills.
In the present study, the variables that best discriminate between participants with high and low reserve, in the initial stages of AD, are the participant’s cognitive level, memory, attention and language, and results that are in line with those obtained by authors such as Fritsch et al. 8 They report that leisure activities and educational level are significant predictors of cognitive function in the elderly, finding that the participation in intellectual activities is associated with performance in verbal fluency and that a high educational level can be considered a good predictor of overall cognitive functioning, episodic memory, and processing speed.
In the same vein, Le Carret et al 67 observed in their studies a different pattern in the deterioration of cognitive functions as a function of the participants’ educational level. Patients with a low level of education showed greater deterioration of the episodic memory and attentional processes. This suggests that in slight or moderate stages of AD, both these functions can benefit from CR, whereas the rest of the functions have lost their compensatory potential.
Our results have allowed us to determine, on one hand, an important relation among the different highly cognitive factors, such as complex leisure activities, good social relations, elevated intellectual activity, reading habits, years of schooling, and professional achievements on the part of patients, and, on the other hand, we find important relations in the type of occupation a patient’s father had as well as his years of schooling as possible factors underlying CR. This suggests that each of these variables contributes independently to the formation of this theory. Our findings are similar to those obtained by many authors who have considered different variables as representative of high CR: a high educational level, 3,10,68 –70 high professional performance, 3,71 and high reading activity. 44
Authors such as Kliegel et al, 48 Richards et al, 32 Richards and Saker, 47 Wilson et al, 43 and Fritsch et al 8 maintain that CR has a dynamic nature, that is, although the initial level of reserve may be determined by innate differences or childhood cognitive activity, there are also processes in youth, adulthood, and old age that can act to increase or decrease that reserve, and authors such as De la Barrera et al 2 show that CR is not stable throughout our lives but is rather a dynamic process that evolves with age and has crucial implications for cognitive functioning in the later stages of life.
Our hypothesis is confirmed by the data published by Valenzuela and Sachdev, 9 who after a meta-analysis of 22 studies that included 29 000 participants reached the conclusion that there is a 46% reduction in the risk of dementia, when there have been high levels of mental activity as compared to low levels. Furthermore, when each of the 3 factors was studied separately (education, occupation, and day-to-day cognitive activities), it was found that they were all similar in magnitude.
Recent studies 46 support this hypothesis, showing that cognitively enriching activities in the second and third stages of life increase CR. According to these authors, beyond the demands of work, those leisure activities that incorporate voluntary and social behaviors that allow participants to engage in different skills and enriched social networks during adulthood have a protective effect. Thus, activities in adulthood seem to influence the later stages of cognitive health in men and women through an increase in CR.
This idea has been supported by numerous epidemiological studies, 45 ,72,73 which suggest that exposure to enriched environments can have observable effects on cognition and the risk of suffering from neurodegenerative diseases associated with age, such as AD.
One of the leisure activities most studied has been physical exercise. Several studies have shown a positive association between physical activity and cognitive function in older persons. 74 Authors such as Dik et al 75 found an important relationship between physical activity in the first stages of life, regardless of current physical activity, and information processing speed. This suggests that individuals who are physically active in the first stages of life may benefit from it in terms of higher information processing speed in old age.
Notwithstanding, other authors 45 ,76 –78 did not find a protective effect of physical activity in relation to cognitive deterioration and AD. Our findings agree with those of the latter authors. We did not find this type of activity to be a possible underlying factor of CR.
One explanation for the lack of an association between participation in physical activities and cognitive deterioration in our study could be that the assessment of this type of activity is not as uniform as the assessment of cognitive activities. Thus, the lack of association may be due to an error in registering information and a lack of standardization.
Given that the studies reporting a significant improvement in cognitive capability as a result of physical activity are mainly the ones that have employed broad systematized procedures for assessment, 79 it would be of interest to posit a future line of research in which by means of a more detailed and structured assessment protocol in relation to this area, it would be possible to confirm whether physical exercise or the elements associated with it are able to delay the cognitive deficiencies that come with age. Furthermore, we have also observed that many of the studies that have found this relationship between physical exercise and a delay in the deterioration of cognitive faculties are those that studied the effects of physical training and intervention with different aerobic, anaerobic, and strengthening activities in older participants with and without dementia. 80,81 This was not the goal of our study, which was limited analyzing retrospective information on physical activity which furthermore was obtained from a sample in which the majority had never been involved in programmed physical activity of a certain duration. It is possible that the procedure used and the characteristics of the sample could explain in part the variance found in the present study in relation to this aspect.
Authors such as Mackinnon et al, 82 studying healthy older participants, found that participants’ performing mental, physical, and social activities in their spare time was associated with better memory; changes having been noted in this function, when the levels of activity are altered. Our results show significant differences between the scores of the high and low reserve participants in the control group in tests that assess mnesic functions, in which we observed a greater alteration in immediate recall of verbal and nonverbal material in the participants with low reserve.
To end, let us consider the principal strong points of our study. First of all, a large variety of variables related to CR were taken into account, increasing the sensitivity of the research and contributing a larger amount of information, thus reducing the possibilities that the differences found in the study may be due to other factors not included in the model. Second, in this research, the sample consisted of patients with incipient AD, which is important given that it is in the early stages of the clinical manifestation of the disease when the effect of CR is most notable. Finally, we should highlight the quality of the neuropsychological evaluation, carried out by means of a rigorous procedure employing a complete battery of tests.
Nonetheless, we must also point out some of the limitations of the research. First, the participants of the control group were selected through nonprobabilistic sampling, which restricts the possibilities for generalization. Furthermore, when assessing the participants’ leisure activities, we did not take into account their frequency, duration or intensity, which could lead to a loss of sensitivity in the assessment of this aspect. Finally, a large part of the sociodemographic information was obtained through interviews, and therefore, some of the data obtained could be participant to biases in interpretation or due to inaccessibility on the part of the participants (especially in those with greater deterioration), and contrasting this information with their family members turned out to be highly complicated.
Taking into account the results obtained, we can conclude that the variables that best discriminate between participants with low and high CR in the initial stage of AD are the participant’s mental state, memory, attention, and language. In contrast, in participants without the pathology, only the mnesic functions discriminate between the low and high reserve participants as regards cognitive function.
To conclude, it can be said that CR is not stable throughout life, but rather is a dynamic process that evolves with age and has crucial implications for cognitive functioning in the later stages of life. Our study supports the effect of higher education, higher professional performance, and ludic activities on CR. This suggests that each of these variables contributes independently to that theory.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.