
Abstract
This study assessed the utility of party horns for quick, simple respiratory function testing in 66 inpatients with dementia to maintain safe eating activity. Relationships of forced vital capacity (FVC) to Mini-Mental State Examination (MMSE) score and complete extension when blowing 40- and 80-cm party horns were examined. The FVC differed significantly by both MMSE score (P = .000) and party horn score (P = .000). Significant differences in FVC were found between groups categorized by MMSE score and in groups categorized by the ability to extend both party horns. Multiple regression analyses performed on possible FVC indicators identified a significant correlation for the party horn examination (regression coefficient: .562). Breathing is always coordinated with swallowing. Party horns seem highly effective as a simple tool for testing respiratory function in patients with early-stage dementia, and the ability to offer breathing rehabilitation for patients in need is likely to result in safer eating activity.
Keywords
Introduction
Aging of the global population is considered to be accelerating. 1 The incidence of dementia is likewise increasing around the world and is predicted to double by 2030. In addition, chronic respiratory diseases are on the rise globally. In fact, respiratory diseases are expected to represent the third to fifth most common causes of death by 2020, according to the World Health Organization. 2
Among patients with dementia, respiratory diseases were the cause of death in 55.5% of patients with Alzheimer’s disease and 33.1% of patients with cerebrovascular dementia. 3 In addition, among nursing home residents with dementia, the probability of at least 1 episode of respiratory disease (such as pneumonia or bronchitis) was nearly 50%, while that of a swallowing problem was 85.8%. 4 Moreover, examination of 412 inpatients in dementia wards found that 73.2% had experienced at least 1 episode of problems affecting the 4 stages of swallowing. 5 With regard to healthy aged individuals, while elastic recoil of the lungs tends to deteriorate with age, the swallowing reflex and cough reflex do not decrease. As for dementia, however, the risk of aspiration pneumonitis gradually increases with decreasing cerebral function. 6,7 Maintenance of expiratory flow and forced vital capacity (FVC) is necessary to avoid aspiration pneumonitis. However, acquisition of reliable data using spirometry requires sufficient training and experience and can be difficult even in healthy older individuals. 8 Because the pulmonary function test is an examination that depends greatly on the understanding and effort of the patient, measurement of lung function itself is difficult in patients with dementia due to the reduced ability to understand and follow instructions. 9 For patients with dementia to maintain safe eating as long as possible, quick and simple respiratory function tests are required to allow a determination of whether respiratory function is sufficient, and a tool enabling such testing as an alternative to the spirometer is indispensable. In this regard, the party horn may prove useful as an evaluation tool. Party horns are already known to be effective for distracting pediatric patients during painful procedures. 10,11 The purpose of this study was to evaluate the party horn as a tool for evaluating respiratory function similar to the spirometer in patients with dementia.
Methods
Patients
This study was approved by the institutional ethics committee of Nagasaki University. Potential participants in this study were 75 inpatients in the dementia ward of a mental institution. Informed consent was obtained from the family prior to participation and 9 patients who were unable to adequately communicate or who could not sufficiently perform the pretest (putting the mouthpiece of the party horn in the mouth and blowing) were excluded. As a result, 66 inpatients (23 men, 43 women; mean age, 80.2 ± 9.43 years) with dementia participated in this research. The type of dementia was Alzheimer’s disease in 28 patients, vascular dementia in 30 patients, and other dementia in 8 patients.
Preparations for Examination
Party horns of 2 different lengths (40 and 80 cm; Party Horn Entertainment Village, Hyogo, Japan) and a spirometer (Mr. Spirometer; Chest M.I., Tokyo, Japan; Figure 1) were used in this study. First, an examiner completely unrolled each new party horn 5 times in order to minimize resistance. Furthermore, we marked each party horn to allow confirmation of whether the tip had completely unrolled. Each party horn had a disposable mouthpiece (Tsutsumi, Tokyo, Japan). To ensure mouthpieces of party horns and the spirometer were exactly the same diameter, we used customized bullhorn-shaped rubber adaptors (Kanae Prosthesis Manufacture, Nagasaki, Japan). The smaller end was joined to the spirometer and the larger end to the disposable mouthpiece (Figure 1).

Spirometer (black rubber adaptor with disposable mouthpiece).
Procedure for Examination
For the recruitment of patients, ward nursing staff selected candidates with stable body functions and informed an examiner who visited the ward on a regular basis to provide therapeutic advice. First, the Mini-Mental State Examination (MMSE) 12 was administered to the patient. Second, the patient was instructed in how to use the party horns and the spirometer. Third, each patient blew the 40- and 80-cm party horns once each (Figure 2). Finally, the patient was obtained the 2 values in the same session of spirometer examination for FVC. Patients were given a 3-min recess after each step. Private information including name, age, and type of dementia was obtained after this examination.

A patient blowing into an 80-cm party horn with disposable mouthpiece.
Data Analysis
Before analysis, MMSE and party horn results were used to define 3 groups each. Criteria for MMSE were group 1, MMSE score 0 to 5; group 2, MMSE score 6 to 10; and group 3, MMSE score 11 to 30. The criteria for party horns were group 1, unable to completely extend either the 40- or 80-cm party horns; group 2, able to completely extend only the 40-cm party horn; and group 3, able to completely extend both the 40- and 80-cm party horns. Furthermore, 2 times of vital capacity data used the one which had high value for analysis.
The data obtained were analyzed using SPSS for Windows version 22. OJ statistical software (SPSS Japan Company, Tokyo, Japan). The Kruskal-Wallis test was used to assess differences between the FVC examinations and the results of examinations including the MMSE and party horns. Next, Bonferroni’s multiple comparison tests were used to compare differences between 3 groups using FVC and the results of examinations. Finally, multiple regression analyses were performed to test items affecting FVC.
Furthermore, patients were divided into 2 groups: a group that could blow the 80-cm party horn to its full length and a group that could not. The chi-square (χ 2 ) test or Fisher’s exact test was used to compare the groups with respect to various factors and categorical variables. Age and height were compared between the groups using the unpaired t test. All results were interpreted using a 5% significance level.
Results
The FVC differed significantly by MMSE score (P = .000). Furthermore, in the 3 groups categorized by MMSE, significant differences in FVC were identified between groups 1 and 2 (P = .000) and between groups 1 and 3 (P = .000; Table 1).
Relationship Between FVC and MMSE.

Abbreviations: FVC, forced vital capacity; G1, group 1; G2, group 2; G3, group 3; MMSE, Mini-Mental State Examination.
a P < .001
The FVC also differed significantly by party horn score (P = .000). Similarly, in the 3 groups categorized by party horn score, significant differences in FVC were evident between groups 1 and 2 (P = .008), groups 1 and 3 (P = .000), and groups 2 and 3 (P = .000; Table 2).
Relationship Between FVC and Party Horn.

Abbreviations: FVC, forced vital capacity; G1, group 1; G2, group 2; G3, group 3.
a P < .001.
b P < .01.
Multiple regression analyses performed on possible indicators of FVC identified a significant correlation for the party horn examination (Table 3). There was a significant difference between the 2 groups in the use of thickening fluids (P = .002) and texture-modifying foods (P = .000) but not in age, height, respiratory diseases, or motor paralysis (Table 4).
Results of Multiple Regression Analysis.
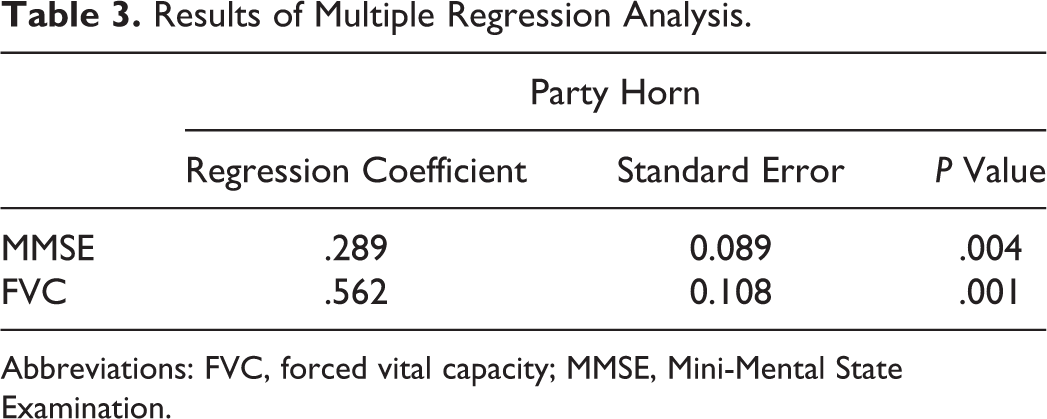
Abbreviations: FVC, forced vital capacity; MMSE, Mini-Mental State Examination.
Characteristics of the 2 Groups Based on Their Ability to Blow the 80-cm Party Horn to Its Complete Length.a
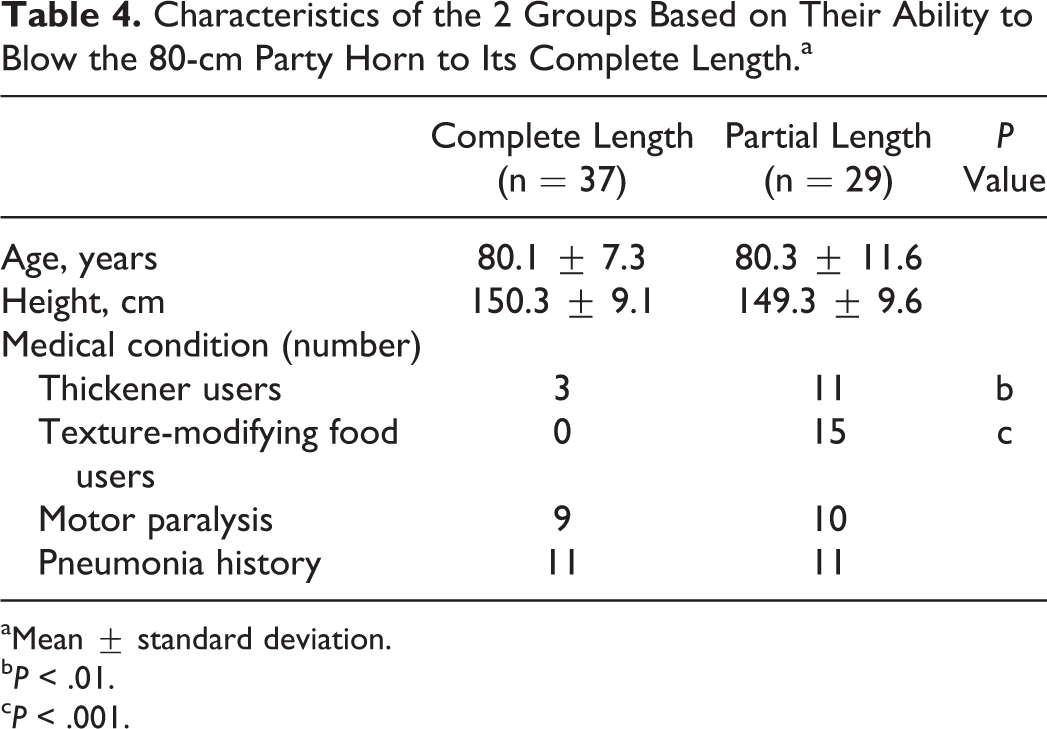
aMean ± standard deviation.
b P < .01.
c P < .001.
Discussion
Participants in this study uniformly showed relatively low MMSE scores and likewise showed low FVC. In addition, the finding of the present study was that the low ability to blow air out of the lungs as measured using a party horn was related to the users of thickening fluids and texture-modifying foods for swallowing dysfunction management. Pathan et al 13 studied correlations among respiratory function, cognitive function, and dementia. They argued that cognitive score is reduced in patients with restrictive ventilatory disorder, involving reduced FVC and forced expiratory volume in 1 second, helping to explain the higher likelihood of needing hospitalization compared to patients with obstructive ventilatory disorder. The longer the duration of hospitalization, the lower the relevance of cognitive scores and respiratory function. Our findings support the results described by Pathan et al. 13
Furthermore, the present study demonstrated that party horns can be applied as a useful tool for evaluating FVC in patients with dementia. Higashijima et al 14 investigated the association between party horn results and respiratory function in university students and identified a correlation between the duration for which a party horn could be blown continuously and FVC. The point of evaluation using a party horn is that full extension requires continuous blowing. To that end, an environmental setting in which the patient is motivated to blow the party horn is important.
Preservation of respiratory function is indispensable for safe eating activity. However, particularly in the early stage of hospitalization, antipsychotic drugs are often administered to patients with dementia to treat restlessness and aggressiveness. As a result, side effects including muscle atrophy due to low activity can arise. 15 Pathan et al 13 reported that muscle atrophy sometimes affects respiratory muscles and the intercostal muscles, greatly increasing the risk of progression to restrictive ventilatory disorder. Higashijima 16 noted that restrictive ventilatory disorder is likely to cause tachypnea and shallow breathing, in turn leading to a greater likelihood of aspiration, since the patient cannot maintain the duration of apnea required for swallowing. Unlike the acute dysphagia found in patients with cerebrovascular disease, dysphagia in patients with dementia develops with disease progression. Higashijima 17 described food coordination and swallowing training as having only a low positive impact if performed after identification of a swallowing disorder, since dysphagia becomes more serious as the state of disease progresses. Gavazzi and Krause 18 suggested pneumonia as the main cause of death in patients with severe dementia. This simply indicates the difficulty of providing proper instruction, including nutritional counseling, at an early stage.
As found by Shaker et al, 19 swallowing and breathing are 2 sides of the same coin. Party horns seem highly effective as a simple tool for testing respiratory function in patients with early-stage dementia and the ability to offer breathing rehabilitation for patients is likely to result in safer eating activity.
The present findings highlight the applicability of party horns for estimating respiratory function in patients with early-stage dementia. We currently provide patients with party horns for respiratory function training and will continue to study correlations between longitudinal changes in respiratory function and risks in eating activity.
Limitations of the Study
Dementia shows intense psychosomatic circadian rhythms and day-to-day variations. The reproducibility of data from MMSE, FVC, and party horns would thus seem low. However, in 2 values in the examination for FVC, no significant difference was seen. We therefore think that the reliability of data for testing carried out within a short interval may be adequate.
Footnotes
Acknowledgments
The authors would like to thank the staff of Deguchi Hospital and Subsection Chief Sakaguchi of Yamashita Medical Instruments (Nagasaki, Japan).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.