
Abstract
The main purpose of this study is to examine the reliability of the Bayer-Activities of Daily Living (B-ADL) scale when used as a cognitive screening instrument for mild and moderate dementia of the Alzheimer type. This is a retrospective study of 66 patients with dementia. The B-ADL scale was completed by the caregiver or the family member at the first encounter. The internal consistency was found to be 0.94 for the 27 patients that completed all 25 questions in the scale. Significant correlation and receiver–operating characteristic curve analysis were found for the B-ADL total score and subscale 1 (tasks requiring short- and long-term memory) for Clinical Dementia Rating scale. Severity of dementia by the B-ADL scale is statistically similar but not the same as Mini-Mental State Examination. Our findings confirm that B-ADL scale is a valid indicator of the cognitive status of patients with Alzheimer’s disease.
Keywords
Introduction
The measurement of functioning in daily life has significant applicability in diagnosis, prognosis, and assessing treatment benefits in dementia. The diagnosis of dementia according to Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition) (DSM-IV) criteria 1 requires the presence of difficulties in functioning in daily life. Cognitive impairment is an unreliable measure of functional capability assessed in the test situation. 2 Cognitive and functional decline do not often occur in parallel, and several studies have shown a low to moderate association between them. In a study of relationship between cognitive function, functional activities, and behavioral problems in patients with moderate Alzheimer’s disease (AD), Teri et al 3 found low but significant correlation between cognition scores and instrumental activities of daily living (IADLs) but no significant association between cognitive scores and basic self-care skill scores.
Functional scales do not often reflect factors such as cognitive impairment, disturbed behavior, caregiver burden among others, and their relationships for they have powerful influences as well. There is no lack of clinical scales to assess function and disability but each has its limitations.
A widely used scale is the Functional Assessment Staging Scale. 4 It is a 7-stage scale in changes in functioning from normal to severe AD, and the functional deterioration occurs in a progressive pattern and had been tested and substantiated by several studies. 5 The Disability Assessment for Dementia Scale 6 was specifically designed for use in patients with AD and had been shown to be a valid measure of activities of daily living. The Bayer-Activities of Daily Living (B-ADL) Scale is an objective measure of functional impairment in which a cumulative score is obtained for ratings of severity of impairment, and this takes the form of a questionnaire completed by the primary caregiver or a family member known to the patient. It is well known that often it is the family member who has noticed functional deficits long before deficits are evident by normal psychometric tests in patients having early or mild cognitive impairment. 7
The purpose of this study to evaluate the B-ADL scale as an objective measure of functional impairment and to examine its utility and reliability when used as a cognitive screening instrument for mild and moderate dementia.
Methods
This is a geriatrician’s office-based retrospective study of 66 patients referred over a period of 3 years by the general practitioner for assessment as to their suitability for use of an acetyl cholinesterase inhibitor. In many instances, however, the general practitioner may have acted as a secondary referral source at the instigation of a family member.
Diagnosis
The diagnosis of dementia was established on clinical grounds using a modified form of the Cambridge Examination for Mental Disorders of the Elderly (CAMDEX). 8 The CAMDEX comprises a number of items, namely, a medical and psychiatric history, a physical examination, mental state examination, cognitive tests, and an interview with a relative or caregiver. For the cognitive part of the examination, the Folstein’s Mini-Mental State Examination (MMSE) 9 was administered and supplemented by such items as the ability to abstract, calculate, and for perceptual abilities. Interview with the relative or caregiver included such information as to orientation, memory, behavior, and the ability to manage everyday activities. Routine laboratory investigation and special investigations were not performed in many for reasons of cost.
The inclusion criteria for the study were the satisfaction of the DSM-IV specifications for the diagnosis of dementia. This broadly includes impairment of memory, deterioration of personality or intellectual ability, and impaired functional capacity. The diagnosis of probable dementia of the Alzheimer type was made on the history, clinical presentation, evidence of progressive intellectual deterioration, and exclusion of other causes of dementia. Vascular dementia and Binswanger’s disease and Lewy body dementia were excluded by the Hachinski Ischaemia Scale, 10 clinical criteria of Caplan and Schene, 11 and McKeith et al, 12 respectively. Staging of the dementia was graded on the Clinical Dementia Rating (CDR) scale of Hughes et al 13 into grades of 1, mild; 2, moderate; and 3, severe as well as by cutoff scores on the MMSE (less than 10 severe, 10-20 moderate, and 21-25 mild). No patients in this study were classified with severe dementia according to either method.
Data Collection
The B-ADL scale incorporates 25 items subdivided into 3 major areas which evaluate general ADL competencies (2 items), specific tasks (18 items) 3 of which relies on short- and long-term memory and 3 other assess orientation, and the remaining 5 items relate to cognitive functions important for management in everyday life. 7 A global score for the B-ADL scale is computed by summating across all items without the inclusion of those rated as “unknown” or “not applicable.” The total is then divided by the number of items rated “1” to “10.” The resulting score ranges between 1 and 10. Two subscores were computed; items 5, 7, and 19 are everyday tasks requiring short- and long-term memory (subscore 1) and items 21 to 25 relating to cognitive functions important for carrying out everyday life activities (subscore 2). The scores were summed and then divided by the number of relevant items rated “1” to “10.” Higher score corresponds to more severe deficits.
Statistical Analysis
Data were collated from 66 deidentified patient records and included gender, age, MMSE, CDR, and the B-ADL scale. Descriptive analyses were used to describe the data set ranges and the association between the 2 definitions of dementia staging, MMSE, and CDR. The concurrent validity of the total B-ALD scale score and its 2 subscores was conducted by examining their associations with the other measures used to diagnose AD, that is, CDR and MMSE. Spearman’s ρ was used to assess the correlation between variables due to the limited ranges of values. Receiver–operating characteristic (ROC) curve analysis was used to evaluate the usefulness of the B-ALD scale scores for diagnostic testing of dementia. Cronbach’s α was used to measure the reliability of the B-ADL and as such measures the internal consistency of the scale rather than test–retest reliability. The IBM SPSS Version 19 was used for all analyses.
Results
According to Folstein’s MMSE, 35 patients were classified as having mild dementia with scores ranging between 21 and 24, and 31 patients were classified with moderate dementia due to having a score between 11 and 20. The overall mean for our sample of 66 was 19.1 with a standard deviation (SD) of 3.9. By definition, patients classified with moderate dementia had a lower mean score (15.6 and 2.5) than patients classified with mild dementia (mean 22.2, SD 1.5).
The CDR is an alternate form of staging dementia and produces very similar results to the MMSE as shown in Table 1. There is 88% of agreement between the 2 techniques of classification, and the Spearman’s ρ correlation was −0.79, being significant at the P < .000 level. A similar number of cases were misclassified in both the directions as illustrated in the table. Due to the high overlap, it is not expected that the 2 methods of dementia staging had a similar age and gender distribution for each classification. The patients with moderate dementia included slightly more females and slightly younger patients.
Correspondence Between MMSE and CDR Classifications of Dementia Staging.
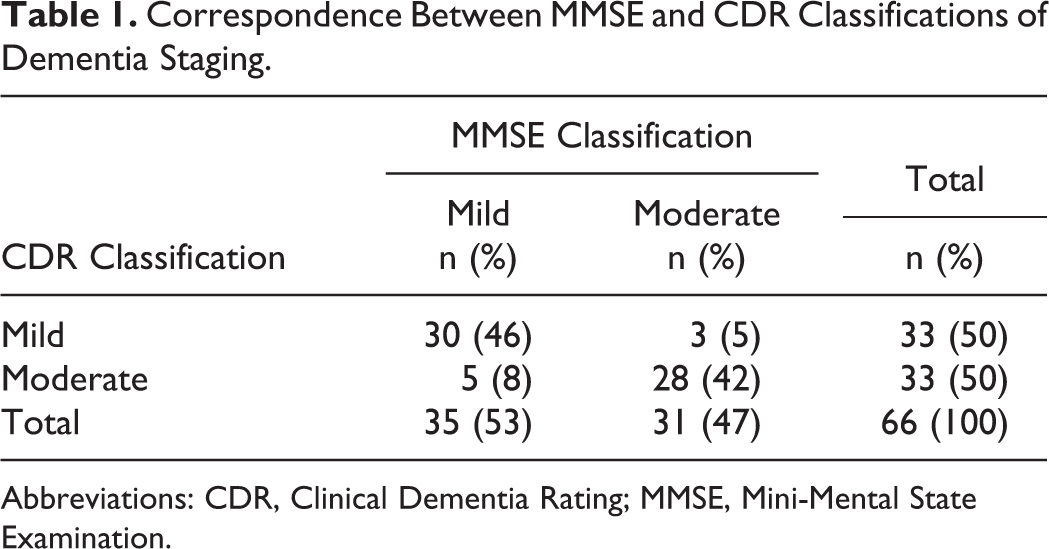
Abbreviations: CDR, Clinical Dementia Rating; MMSE, Mini-Mental State Examination.
As noted previously, the B-ADL average scores for the total scale and the 2 subscores were calculated on the basis of the number of items each patient was able to complete, that is, which were not coded as being “not applicable” or “unknown.” The completion rate for the 25 items on the B-ADL scale in this study ranged from 80% to 100% with an average of 92% of patients completing any item. The total number of “nonapplicable” and/or “unknown” answers for the whole B-ADL scale was 13.4 which averages to 5.4% per item. The 3 B-ADL items least likely to be completed were item 11 “going for a walk without getting lost” (20%), item 19 “using transportation” (18%), and item 20 “participating in his/her leisure activities” (18%). All other items were answered for 86% or more of the patients in this study. Figure 1 shows the number of B-ADL items answered by each patient for the 2 methods of dementia staging as well as the sample overall. Only 2 (41%) in 5 of the entire sample completed all the 25 items, and as shown in Figure 1, the completion rate was higher for the moderate patients with dementia as classified by the MMSE. However, the difference is small, and the median completion rate was 24 of 25 items for all groups shown in Figure 1.
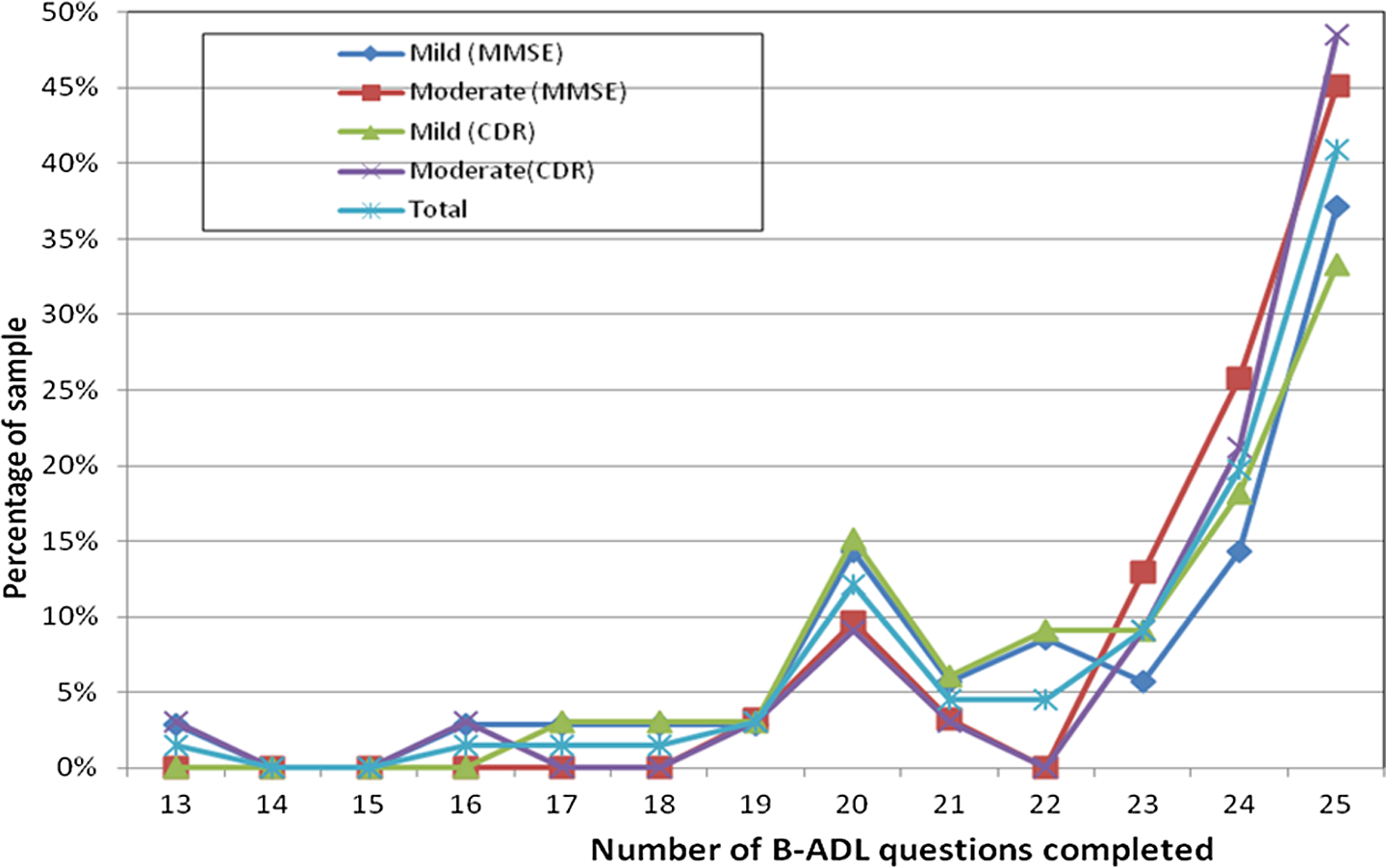
Response rate for the B-ADL scale items by dementia staging. B-ADL indicates Bayer-Activities of Daily Living.
As the reliability analysis is based on the correlation between the total score and each item of the scale, the Cronbach α could only be calculated using the results for the 27 patients who completed the entire scale. Despite the small sample, a very high reliability of 0.937 was found for the full scale of 25 items. The Cronbach α reliability of the 3 items comprising the B-ADL-subscore 1 regarding memory was 0.583 and was based on the 51 patients who had responses to items 5, 7, and 19. The reliability of the cognitive function B-ADL subscore 2 from items 21 to 25 inclusively was calculated from the results of 54 patients and was found to be 0.856 according to Cronbach α. However for B-ADL subscore 2, there was a significant additive association or multiplicative interaction within patients between items with F = 7.29 and P < .000 according to Tukey’s test for nonadditivity. This was primarily due to a high intercorrelation r = .75 between items 22 and 23 and items 22 and 25. Although based on small samples, these results do support the reliability of the B-ADL scale.
Summary statistics for the B-ADL scale and 2 subscales for each dementia staging method are presented in Table 2. Although patients with moderate dementia had a higher B-ADL total score and B-ADL subscale 1, they had a lower B-ADL subscale 2 than patients classified with mild dementia according to both the staging methods. The difference between the B-ADL mean scores of mild and moderate patients with dementia was greater for CDR classification than for MMSE.
B-ADL Scores by Dementia Staging.
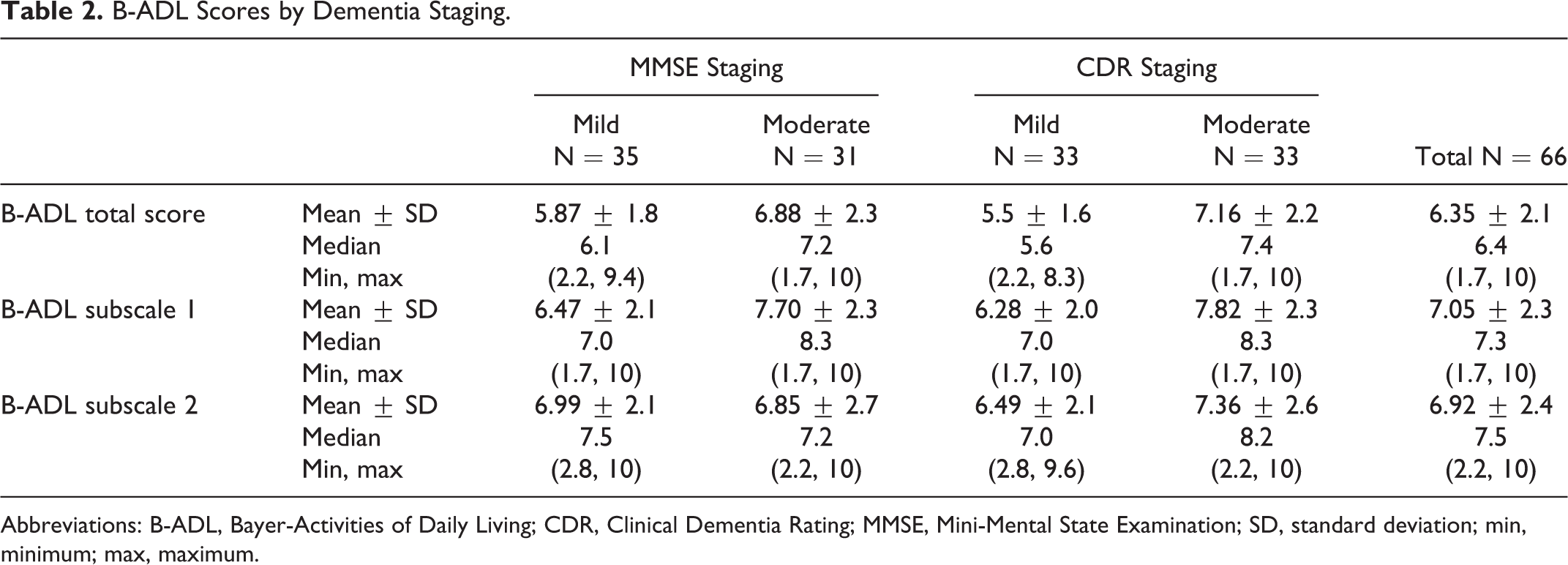
Abbreviations: B-ADL, Bayer-Activities of Daily Living; CDR, Clinical Dementia Rating; MMSE, Mini-Mental State Examination; SD, standard deviation; min, minimum; max, maximum.
Correlation analysis further illustrates the higher association between CDR and B-ADL than for MMSE and B-ADL, even when CDR is measured dichotomously and MMSE scores rather than the classification are analyzed. As shown in Table 3, the correlation between the B-ADL average score and subscore 1 was significant for both CDR and MMSE. The only significant correlations found for B-ADL subscale 2 were with the other B-ADL measures. It should be noted that the correlations between MMSE and CDR are much greater than the significantly though modest correlations with B-ADL suggesting that although they may have some commonality, B-ADL is measuring a different aspect of dementia.
Correlations With B-ADL.
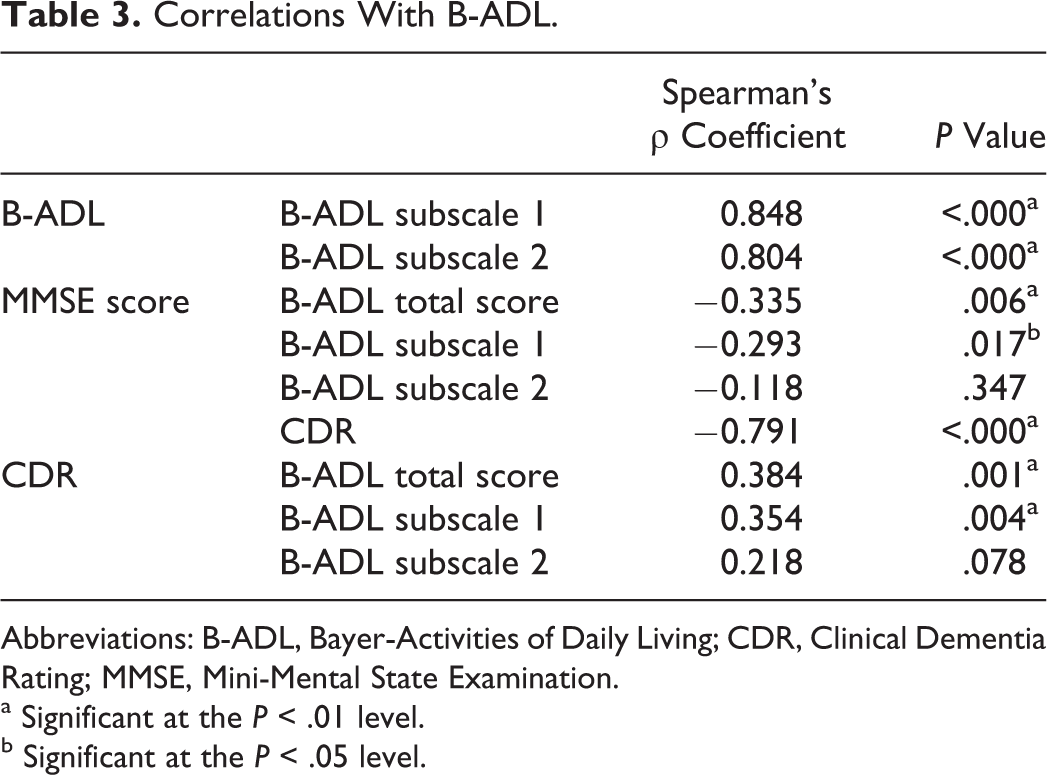
Abbreviations: B-ADL, Bayer-Activities of Daily Living; CDR, Clinical Dementia Rating; MMSE, Mini-Mental State Examination.
a Significant at the P < .01 level.
b Significant at the P < .05 level.
Table 4 presents a summary of the ROC analyses that were conducted with moderate dementia being the positive group to be diagnosed by B-ADL measures. The ROC analysis found similar results to the correlations in that the sensitivity of the B-ADL scale was greater when the CDR staging was used as the diagnosis rather than MMSE. Subscale 2 was not significantly different from the null hypothesis of the areas under the ROC = 0.5 for either staging methods. As shown in Table 4, the highest average value of sensitivity for all possible values of specificity was 0.722 for the total B-ADL scale and CDR, being significant as <.01. The ROC results are therefore only presented graphically for CDR in Figure 2.
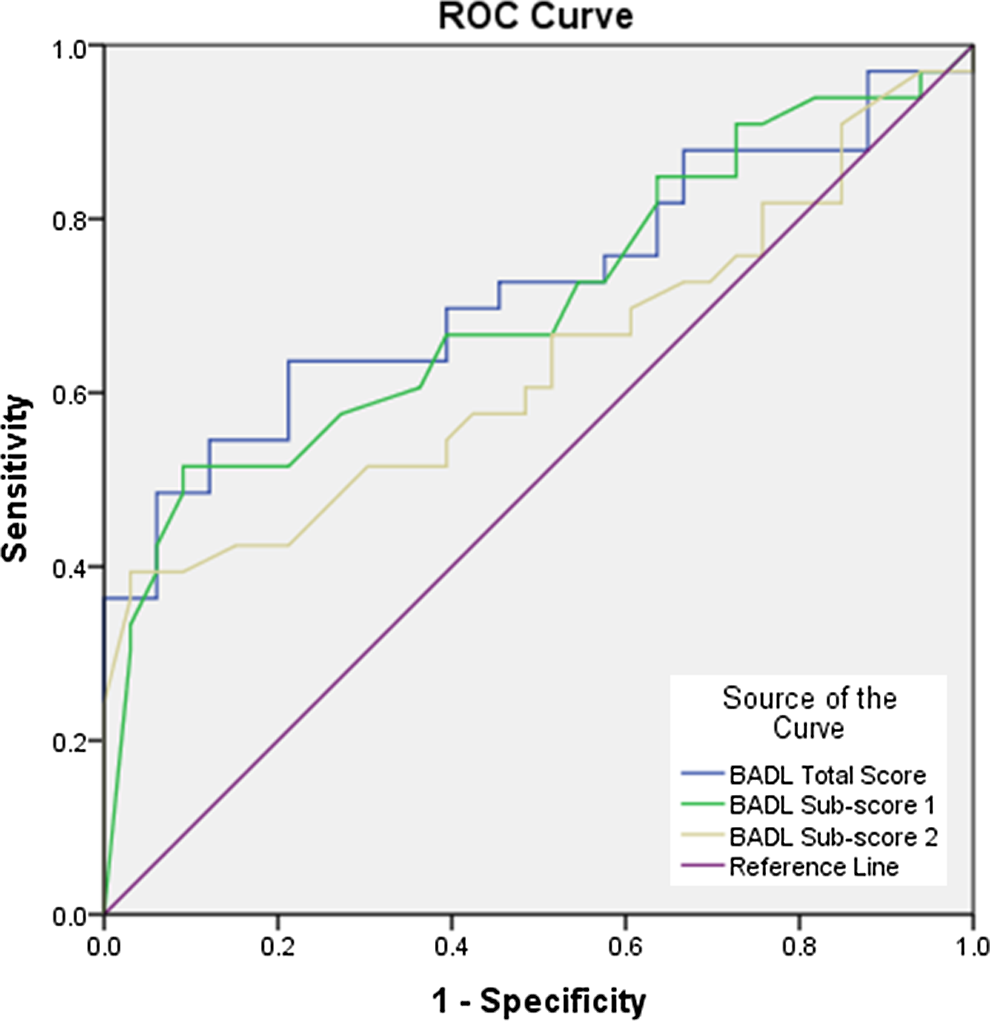
ROC curve for B-ADL scale by CDR dementia staging. B-ADL indicates Bayer-Activities of Daily Living; ROC, receiver–operating characteristic; CDR, Clinical Dementia Rating.
ROC Summary for B-ADL Diagnosis of Moderate Dementia.
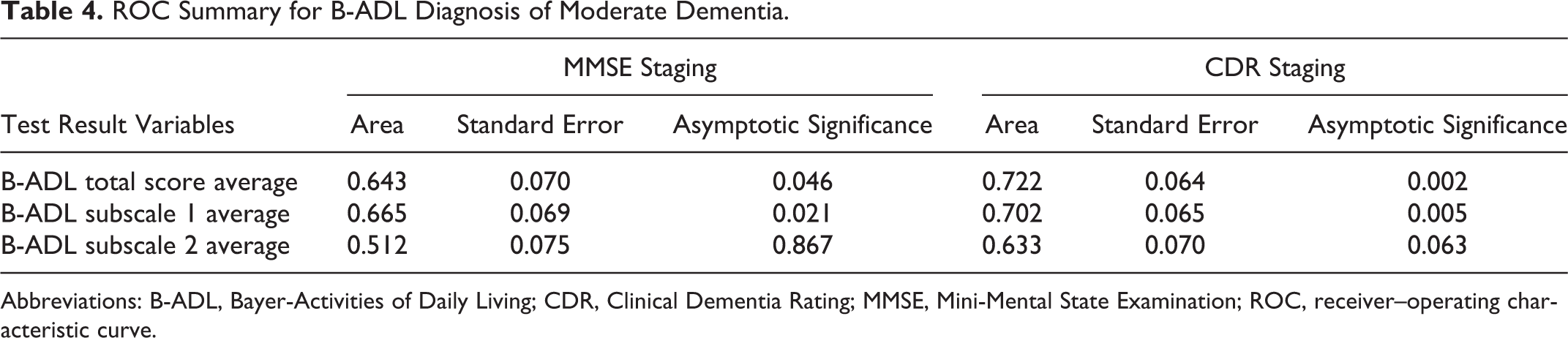
Abbreviations: B-ADL, Bayer-Activities of Daily Living; CDR, Clinical Dementia Rating; MMSE, Mini-Mental State Examination; ROC, receiver–operating characteristic curve.
Discussion
The measurement of functioning in daily life has significant relevance in the diagnosis of dementia. 3,14 The B-ADL was performed in 3 European countries, United Kingdom, Germany, and Spain to determine its validity and reliability, and it was shown that B-ADL total score was significantly increased between adjacent Global Deterioration Scale stages 1 to 5. The B-ADL proved to be as efficient as MMSE in the United Kingdom and German samples and was superior to the MMSE in the Spanish samples. 15 Although our study found significant correlations between B-ADL and MMSE, we identified higher correlations between B-ADL and CDR. The significant correlations were true for the total B-ADL average and the B-ADL subscale 1 measuring short- and long-term memory. The B-ADL subscale 2 regarding cognitive functions for everyday life activities was found not to be associated with the MMSE or CDR method of dementia staging.
According to Erzigkeit et al, 15 in order to substantiate the applicability of B-ADL, the acceptable proportion of the “not applicable” answers should be lower than 5% for the whole scale and lower than 10% for each individual item. However, Erzigkeit et al 15 reported 3 to 5 items with percentages higher than 10%. Another study 16 found 2% of the “nonapplicable” answers for the whole scale and over 10% for 2 items. In our study, the “not applicable” or “unknown response” was 5.4% for the total scale, and there were 3 items where the total nonresponse was 1 in 5 patients, item 19 “transportation”, item 11 “getting lost,” and item 20 “leisure activities.” The reason for the higher nonresponse on these items in particular warrants further investigation.
The Cronbach α determines the internal consistency or average correlation of items and higher the score the more reliable is the generated scale. 17 The internal consistency in our study was 0.94, very similar to that in other studies. 15,16,18 It should be noted that the generalizability of this study is necessarily limited by the small number of cases and that the results reported here need to be verified on further samples. Sikkes et al 19 in a study of 12 questionnaires for the evaluation of IADLs reported that no questionnaire showed a satisfactory rating in all the criteria they used. According to their criteria, B-ADL received a negative rating for internal consistency. In our study, however, given that internal reliability increases with more sampling of behavior, it is not unexpected that the reliability for the B-ADL subscales was lower than that for the total scale.
It may be useful to examine areas of function that may be important in the daily life of patients with dementia. According to Teunisse et al, 2 it is necessary to determine what aspects of function should be assessed to get a complete picture of the severity of dementia. We compared the results obtained for B-ADL scale and the subscores, B-ADL subscore 1 and B-ADL subscore 2, for assessing deficits. The data for the 66 patients included in this study demonstrate that the B-ADL subscore 1 has a stronger association with other dementia measures than B-ADL subscore 2. We found a sensitivity of 93.9% and a specificity of 12.1% for both the B-ADL total scale average and the subscore 1. However, given the high number of “nonapplicable” or “unknown” responses and our small sample size, these results need verification with other larger samples.
Some of the instruments are questionnaires, self-reported or interviews, and others are direct observations, and there is considerable debate about which is better. In patients with dementia, their insight is frequently impaired and self-reported questionnaires are hard to assess. Jorm and Korten 20 studied the feasibility of measuring cognitive decline in the elderly patients from informants. They developed a standardized interview to measure the decline in both intelligence and memory of an elderly person’s current performance and 10 years earlier. They found this was a valid measure of cognitive decline and has less contamination with premorbid ability than the MMSE. The use of informants had also been suggested by Henderson and Huppert 21 for the diagnosis of early dementia, because they are better informed of the patients performance. Other workers 22 found informant reports have little validity as to memory functioning in the elderly patients. In a study of patients with severe aphasia and possible dementia, the findings indicated the limitations of verbal and nonverbal cognitive tests and the reliance on informant reports. 23
There has been several reports of the combination of cognitive testing with informant questionnaire improving the accuracy in the screening of mild to moderate dementia, 24,25 more so in the low-educated people. 26 Others have found no advantage in combining cognitive tests and an informant report. 27 The high nonresponse found in our study further reinforces the need to ensure that all diagnostic instruments are as complete as possible.
Functions measured by the B-ADL scale are the basic activities of daily living, IADLs, and cognition. The scale combines functional performance as well as cognitive testing. It gives an indication of the extent of loss of functional autonomy and hence can be used in clinical follow-up and for documentation of the efficacy of treatments. 7 In this study, there was insufficient sample to analyze cognition along the line of disease progression. Hence, the possible limitation in this study is that it could have been more objective if the functional performance had been looked at in relation to cognitive changes. This may have helped to extend our knowledge of the loss of functional performance as the disease progressed.
In conclusion our observations reinforce previous findings. The B-ADL scale is an objective measure of functional impairment and exhibits a broad array of domains and is a valid indicator of the cognitive status of patients with Alzheimer’s disease. In our opinion, B-ADL scale is reliable and highly acceptable and may be useful as a screening tool for dementia in primary care and community services. Combination of B-ADL scale (informant questionnaire) and cognitive testing (MMSE) may improve accuracy in screening of mild and moderate dementia. We would like to suggest the combination of B-ADL subscore 1 (assess everyday tasks which require unimpaired short- and long-term memory) with CDR may enhance accuracy and efficiency of screening of dementia in the clinical setting.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.