
Abstract
Memory decline is often among the first signs heralding the emergence of mild cognitive impairment or dementia regardless of etiology. Despite its limited inclusion of memory screening, the Mini-Mental State Exam (MMSE) continues to be the most ubiquitous, first-line screening tool for dementia and cognitive decline. In response to well documented problems with the sensitivity of this instrument and the growing importance of cognitive screening, we assessed the utility of the MMSE as a screening tool among older adults presenting for evaluation at a memory clinic. The Standardized MMSE and a standardized verbal memory test — the Hopkins Verbal Learning Test-Revised (HVLT-R) — were administered to 304 consecutive referrals at a university-based outpatient memory clinic. Among patients scoring above 25 on the MMSE (n = 169), over half exhibited at least moderate memory impairment (HVLT-R delayed recall z ≤ −2.0) and more than 25% showed severe impairment (delayed recall z ≤ −3.0). Perhaps even more striking was that among those who achieved perfect (30/30) or near perfect (29/30) scores on the MMSE (n = 70), 43% displayed moderate to severe memory impairment. Although newer screening measures have shown improved sensitivity, more in-depth memory testing appears to be a vital component of successful screening and early detection.
Background
Memory loss is a growing concern among older adults seeking consultation with their general care physicians. According to the Alzheimer’s Association, an estimated 7.1 million Americans aged 65 years and older will have Alzheimer’s disease in 2025, representing a roughly 40% increase over the next decade. 1 Mild cognitive impairment is a term coined by Petersen and colleagues 2 to define individuals who display cognitive deficits without functional impairment. Although a mild cognitive impairment diagnosis does not require memory impairment, amnestic mild cognitive impairment is the most prevalent subtype 3,4 and may convert to dementia more frequently and more quickly than nonamnestic subtypes. 5 –8
Given the central role of memory impairment in both dementia (regardless of etiology) and the most common type of mild cognitive impairment, successful screening and early detection of these disorders hinge largely on adequately sensitive detection of memory impairment. Over 2 decades ago, Welsh and colleagues 9 demonstrated that tests of delayed recall had particular utility in the early detection of Alzheimer’s disease, suggesting that such tests should be a point of focus in screening for dementia.
The Mini-Mental State Examination (MMSE) 10 has been the most widely utilized screening tool for dementia for more than 25 years. Although initially viewed as an inpatient screen for general cognitive impairment, it is often utilized as the standard screening tool for cognitive impairment and dementia in outpatient settings. 11 Mitchell 12 conducted a meta-analysis of 39 studies examining the utility of the MMSE for detecting cognitive impairment across a variety of clinical settings. In memory clinic settings, the MMSE was found to have a pooled sensitivity of 0.79, a positive predictive value of 0.86, and a negative predictive value of 0.73 for detection of dementia. The case-finding ability of the MMSE was best in specialist settings when used to confirm a suspected diagnosis.
Despite these relatively promising findings, the problem of high false-negative rates has surfaced repeatedly across 3 decades of literature on the MMSE. 13 –17 For instance, echoing longstanding concern over the measure’s inadequate sensitivity, Galasko and colleagues 18 found that 5 (nearly 19%) of 27 patients with a diagnosis of mild Alzheimer’s disease scored 27 or above on the MMSE. Shiroky et al 19 revealed that, although uncommon (eg, 8 of 632 patients in their study), patients with a diagnosis of probable Alzheimer’s disease can actually perform perfectly (30 of 30) on the MMSE. More recent investigations have revealed that the MMSE is particularly insensitive to subtle cognitive deficits and is not a valid screening tool for early stage Alzheimer’s disease 20 or mild cognitive impairment. 21 For instance, using the commonly employed a cutoff of ≤25, Nasreddine and colleagues 21 revealed that the MMSE had a sensitivity of only 18% for the detection of mild cognitive impairment.
Debate over the sensitivity and overall utility of the MMSE has been compounded by a considerable lack of uniformity or agreement around a single standard cutoff score. In fact, a rather wide range of cutoff scores has been suggested with no single cutoff emerging as a “gold standard” for classifying a patient as impaired. In addition, based on longstanding evidence that MMSE scores are mediated by age and educational attainment, 22,23 attempts have been made to identify optimal cutoffs for different groups based on these demographic factors. 24 –26 In spite of such efforts, there remains a lack of uniform clinical guidelines for adjusting the cutoff score based on age and education, leaving clinicians to rely solely on their judgment on a case-by-case basis. In a recent review and update of cognitive screening procedures, 11 a cutoff of ≤25 was indicated as reflective of normal, intact functioning. However, others 27 have recently demonstrated that a higher cutoff of ≤28 may be most useful in screening for mild cognitive impairment. Thus, there remains a lack of clarity as to what score may indicate impairment and for whom.
In response to concerns about individual raters using idiosyncratic procedures (ie, offering hints and giving half points) when administering and scoring the MMSE, attempts have been made to standardize administration and scoring procedures so as to improve the interrater and intrarater reliability of this measure. The Standardized MMSE (SMMSE), 28 although identical to the original MMSE with respect to test content, follows strict guidelines and instructions for standardized administration and scoring. Specifically, the SMMSE provides verbatim instructions to be read aloud to the examinee for each item, detailed rules for standardized scoring, and time limits on all tasks (see Molloy and Standish for a review). 28
Against a backdrop of a wide range of suggested cutoffs and serious concerns about the test’s sensitivity, a number of authors have explored the specific limitations of the content and structure of the MMSE. Leading criticisms include the fact that embedded memory testing is limited to a brief delayed recall of 3 words with no long delayed recall or recognition component; the lack of direct tests of executive/frontal abilities; single-item assessment of most functions with no graded scoring; and the lack of more challenging, cognitively demanding items. 29 The lack of sufficient memory assessment may be the most limiting characteristic of the test, as detection of memory impairment is fundamental to the diagnosis of amnestic mild cognitive impairment and dementia.
Many formal neuropsychological measures have been developed to provide more robust, in-depth assessment of memory function. Given concerns over the sensitivity of the MMSE, authors have directly compared its utility to that of standard neuropsychology memory tests in the detection of dementia. Frank and Byrne 30 compared the sensitivity of the MMSE to that of the original list-learning measure, the Hopkins Verbal Learning Test (HVLT), 31 in the detection of mild dementia among older adult participants. The authors found the raw learning score on the HVLT to be more sensitive (0.96) but less specific (0.80) to mild dementia than the MMSE (sensitivity = 0.88; specificity = 0.93) using optimal cutoff scores of 18 and 25, respectively. Noting the higher susceptibility of MMSE to ceiling effects among those with mild impairments, the authors concluded that the HVLT may be more useful in the early detection of dementia. Building on these findings, Hogervorst and colleagues 32 found that the inclusion of the HVLT recognition discrimination index improved the test’s sensitivity in the detection of dementia slightly from 0.87 (raw learning score alone) to 0.91 (raw learning score and recognition discrimination index combined).
Others have called into question the overall utility of the original HVLT, which lacks a delayed recall trial, as a dementia screening tool. Kuslansky and colleagues 33 noted relatively modest sensitivities and positive predictive values for both the MMSE (sensitivity = 0.86) and the HVLT (sensitivity = 0.83) in the detection of dementia, suggesting that a large number of individuals with significant cognitive impairment would be misclassified as “intact” by either test used alone.
The most recent version of the HVLT, the Hopkins Verbal Learning Test-Revised (HVLT-R), 34 was reworked to include a delayed (20 minutes) free recall trial. This newer version has been shown to have high sensitivity (0.95) and moderate specificity (0.83) in distinguishing patients with probable Alzheimer’s disease from normal controls. 35 Given that tests of delayed recall have been shown to have good utility for cognitive screening, 9 there is a need to compare the utility of the MMSE to that of the HVLT-R in screening for cognitive impairment among older adults presenting with cognitive complaints. This need is underscored by ongoing uncertainty and debate as to the viability of the MMSE as a screen for milder manifestations of cognitive impairment.
Objective
Given the current public focus on early detection of memory decline and the central diagnostic role of memory decline in dementia diagnosis across etiologies, the focus of this investigation was to address the sensitivity of the MMSE as a screening measure for memory impairment. By International Classification of Diseases, Tenth Revision diagnostic definition, 36 memory impairment is a core symptom of dementia, regardless of etiology. In addition, although several subtypes of mild cognitive impairment are recognized, the amnestic subtype is most prevalent and may convert to dementia more frequently and more rapidly than other subtypes. 3 –8 Thus, successful detection depends largely on the utilization of screening measures that are adequately sensitive to memory impairment, including more subtle, emergent memory deficits. Although a total SMMSE score above 25 has recently been indicated as reflective of normal, intact functioning, 11 others 27 have revealed that a cutoff of ≤28 may be most useful in detecting mild cognitive impairment. Using both of these cutoffs (≤25 and ≤28) successively, we examined the utility and sensitivity of the SMMSE as a screening tool by exploring the extent to which it captured those individuals with significant memory impairment as defined by performance on a more in-depth, standardized verbal memory measure.
Design
This study was approved by the University of Chicago institutional review board. Retrospective data from a clinical database of older adult (65 years or older) memory center patients seen for neuropsychological evaluation by a University of Chicago neuropsychologist were collected and analyzed. Medical records and neuropsychological reports were examined for demographic data along with SMMSE raw scores; Wide Range Achievement Test-Fourth Edition (WRAT4) 37 Reading subtest standard scores; and HVLT-R raw and z scores for total learning (ie, total correct responses across 3 immediate recall trials), delayed recall (ie, total correct responses spontaneously recalled after a 20-minute delay), and recognition discrimination (ie, number of true positives − number of false positives on the recognition paradigm). Hopkins Verbal Learning Test-Revised delayed recall and recognition discrimination z scores served as our primary indicators of memory performance. All measures were administered on the same day by a master-level neuropsychology-trained technician under direct supervision of a licensed clinical neuropsychologist. All data analyses were conducted using SPSS-19. In order to analyze the screening utility (in this case, the sensitivity to memory impairment as observed on the HVLT-R) of the SMMSE at 2 different cutoffs proposed in the recent literature, 11,27 participants were initially grouped based on a SMMSE cutoff score of ≤25 and then again at a cutoff score of ≤28. Additionally, memory performance of those scorings perfectly on the SMMSE was analyzed.
Participants
Patients (N = 304) were older adults referred for neuropsychological examination by their geriatrician, neurologist, or primary care physician. Patients’ ages ranged from 65 to 95 years (mean = 78.55; standard deviation [SD] = 7.24). In all, 30% were caucasian and 67% were African American. Mean education was 13.47 years (SD = 3.48). In all, 31% were male and 69% were female.
Measures
The SMMSE is a 30-item clinician-administered cognitive screening measure allowing for brief and simple assessment of a limited set of cognitive abilities. It has been shown to have adequate test–retest and interrater reliability (r = .89 and .82, respectively) and to discriminate between patients with probable Alzheimer’s disease and healthy controls with 87% sensitivity and 82% specificity. 29
The HVLT-R is a clinician-administered auditory verbal list-learning task consisting of 3 learning trials of a 12-item word list, 1 delayed (20 minutes) recall trial, and a recognition discrimination paradigm. This measure has been shown to have adequate test–retest reliability (total recall r = .74). 34 For the purposes of our study, z scores for total learning, delayed recall, and recognition discrimination were analyzed. Consistent with common standards for interpreting neuropsychological performance on standardized measures, “mild” impairment was defined as a performance of at least 1.5 SDs below the mean (z ≤ −1.5), “moderate” impairment was defined as a performance of at least 2 SDs below the mean (z ≤ −2), and “severe” impairment was defined as a performance of at least 3 SDs below the mean (z ≤ −3).
The WRAT4 Reading subtest has been shown to have strong internal consistency, moderate alternate-form reliability, and adequate concurrent validity as measures of verbal intellectual achievement. 37 It is a widely utilized estimate of premorbid intellectual functioning.
Statistical Analyses
The relative contribution of age, educational attainment, estimated premorbid intellect, gender, and race to SMMSE scores in the full sample was explored via multiple regression analysis. Based on results, partial correlations were performed to analyze the correlation between SMMSE scores and HVLT-R memory performance while controlling for age and education. After analyzing SMMSE and HVLT-R performance of the full sample, we split the sample into “intact” and “impaired” groups based on a SMMSE cutoff of ≤25 and conducted within-group and between-group analyses of HVLT-R memory performance. The group means for HVLT-R total learning z score, HVLT-R delayed recall z score, and HVLT-R recognition discrimination z score were then calculated. Frequency distributions were analyzed to determine percentages of “intact” patients (SMMSE > 25) demonstrating mild, moderate, and severe levels of memory impairment on the HVLT-R. Finally, independent samples t tests were conducted to compare HVLT-R memory performance between “intact” (SMMSE > 25) and “impaired” (SMMSE ≤25) groups. These analyses were then replicated utilizing a SMMSE cutoff of ≤28. Additional analyses were performed to assess the HVLT-R performance of those scoring perfectly on the SMMSE.
Based on evidence that MMSE scores are mediated by age and educational attainment, 22,23 supplemental analysis was conducted to explore the question of whether patients who exhibited a similar magnitude of memory impairment (ie, mild, moderate, or severe) on the HVLT-R would perform differentially on the SMMSE as a function of age and educational attainment.
Results for Full Sample
The SMMSE overall group mean was 25.22 (SD = 4.15). More than half (55%; n = 169) of the sample obtained a SMMSE score above 25, with 23% (n = 70) scoring above 28 and 8.5% (n = 26) scoring perfectly. Demographic differences between those patients scoring above and below suggested cutoffs of ≤25 and ≤28 are presented in Tables 1 and 2. When SMMSE performance was predicted via multiple regression, it was found that age (β = −.22, P < .001), educational attainment (β = .23, P < .001), and estimated premorbid intellect (ie, WRAT4 Reading SS; β = .30, P < .001) were significant predictors, while race (β = −.03, not significant [ns]) and gender (β = −.001, ns) were not. The overall model fit was R 2 = .25.
Age, Education, and Estimated Premorbid Intellect Among “Intact” Versus “Impaired” Participants Using a SMMSE Cutoff of ≤25.
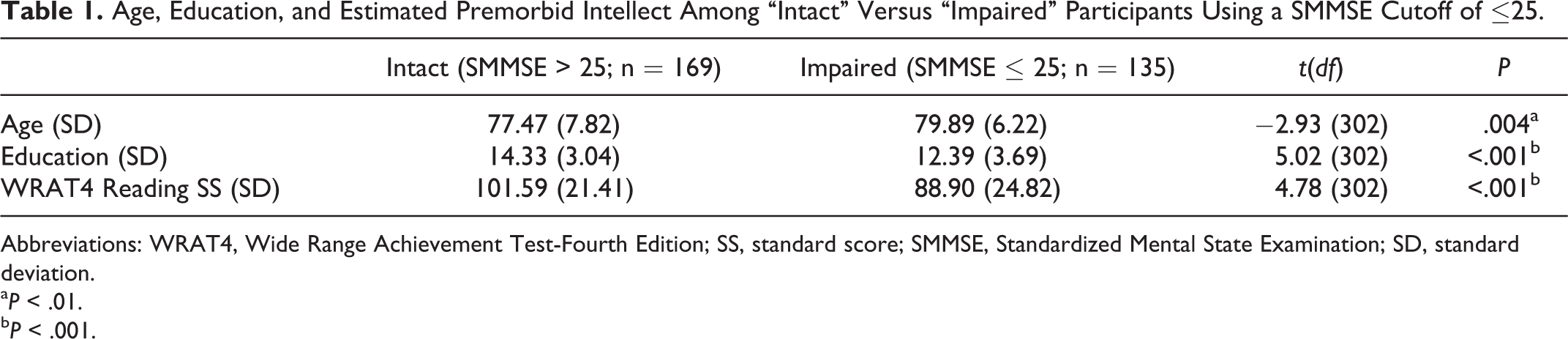
Abbreviations: WRAT4, Wide Range Achievement Test-Fourth Edition; SS, standard score; SMMSE, Standardized Mental State Examination; SD, standard deviation.
a P < .01.
b P < .001.
Age, Education, and Estimated Premorbid Intellect Among “Intact” Versus “Impaired” Participants Using a SMMSE Cutoff of ≤28.

Abbreviations: WRAT4, Wide Range Achievement Test-Fourth Edition; SS, standard score; SMMSE, Standardized Mental State Examination; SD, standard deviation.
a P < .001.
On the HVLT-R memory measure, mean total learning for the full sample was in the mildly impaired range (z = −1.89, SD = 1.06). Both mean delayed recall (z = −2.28, SD = 1.32) and mean recognition discrimination (z = −2.82, SD = 2.22) were in the moderately impaired range. Group means for HVLT-R total learning, delayed recall, and recognition performance of patients grouped by SMMSE performance are presented in Table 3. For the full sample, there was a significant correlation between the SMMSE total score and the total learning (pr = .55, P < .001, df = 299; pr 2 = .30), delayed recall (r = .43, P = .001, df = 299; pr 2 = .18), and recognition discrimination (r = .46, P < .001, df = 299; pr 2 = .21) trials of the HVLT-R, even after controlling for age and education.
Mean HVLT-R Total Learning, Delayed Recall, and Recognition Performance of Patients Grouped by SMMSE Cutoffs.

Abbreviations: HVLT-R, Hopkins Verbal Learning Test-Revised; SMMSE, Standardized Mini-Mental State Examination; SD, standard deviation.
Results for SMMSE Cutoff of ≤25
On the HVLT-R, those “intact” patients scoring above 25 on the SMMSE (n = 169) obtained a mean total learning z score of −1.42 (SD = 0.95), a mean delayed recall z score of −1.79 (SD = 1.46), and a mean recognition discrimination z score of −1.83 (SD = 1.89), suggestive of mild memory impairment overall. On delayed recall, 62% (n = 106) of these “intact” patients showed at least mild memory impairment (HVLT-R delayed recall z ≤ −1.5). Moreover, more than half (51.5%; n = 87) of these patients displayed at least moderate impairment (HVLT-R delayed recall z ≤ −2.0) and more than 1 (25.4%; n = 43) in 4 displayed severe impairment (HVLT-R delayed recall z ≤ −3.0). With respect to recognition discrimination, more than half (53.3%; n = 90) of these patients exhibited at least mild impairment, 41.4% (n = 70) exhibited at least moderate impairment, and 23.7% (n = 40) exhibited severe impairment. As a group, those patients scoring above 25 on the SMMSE performed significantly better than those patients scoring below that cutoff with respect to HVLT-R total learning, delayed recall, and recognition discrimination (all Ps <.001; see Table 4).
HVLT-R Memory Performance of “Intact” Versus “Impaired” Patients Using 2 Different SMMSE Cutoff Points.
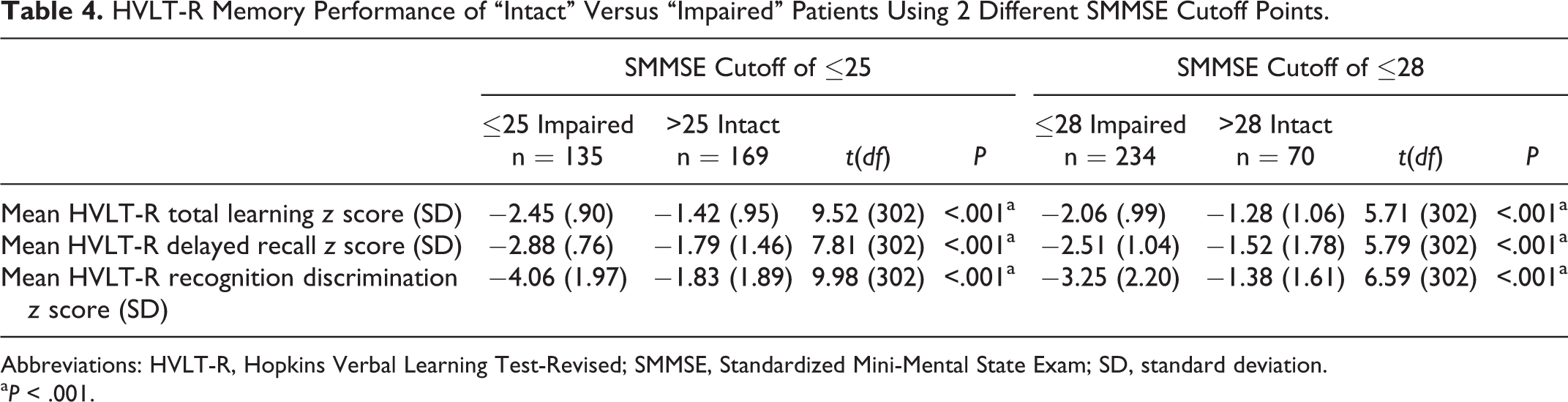
Abbreviations: HVLT-R, Hopkins Verbal Learning Test-Revised; SMMSE, Standardized Mini-Mental State Exam; SD, standard deviation.
a P < .001.
Results for SMMSE Cutoff of ≤28
On the HVLT-R, those “intact” patients scoring above 28 on the SMMSE (n = 70) obtained a mean total learning z score of −1.27 (SD = 1.06), a mean delayed recall z score of −1.52 (SD = 1.78), and a mean recognition discrimination z score of −1.38 (SD = 1.60), suggestive of low average to mildly impaired memory function overall. On delayed recall, 55.7% (n = 39) of these “intact” patients showed at least mild memory impairment (HVLT-R delayed recall z ≤ −1.5). Moreover, 43% (n = 30) of these patients displayed at least moderate impairment (HVLT-R delayed recall z ≤ −2.0) and more than 15% (n = 11) displayed severe impairment (HVLT-R delayed recall z ≤ −3.0). With respect to recognition discrimination, more than 40% (n = 29) of these patients exhibited at least mild impairment, more than 30% (n = 22) exhibited at least moderate impairment, and 15.7% (n = 11) exhibited severe impairment. As would be expected, those patients scoring above 28 on the SMMSE performed significantly better than those patients scoring below that cutoff with respect to HVLT-R total learning, delayed recall, and recognition discrimination (all Ps <.001; see Table 4). Patients who scored above 28 performed significantly better than patients who scored in-between the 2 cutoffs (ie, those who achieved a score of 26, 27, or 28; n = 99) with respect to HVLT-R delayed recall (P < .05) and recognition discrimination (P < .001), but not total learning (P = .08).
Results for SMMSE = 30
Finally, even among the 26 patients (8.6% of our full sample) who performed perfectly (30 of 30) on the SMMSE, more in-depth memory testing (ie, HVLT-R) revealed significant memory impairment. These patients obtained a mean total learning z score of −1.38 (SD = 1.37), a mean delayed recall z score of −1.69 (SD = 1.29), and a mean recognition discrimination z score of −1.17 (SD = 1.17), suggestive of low average to mildly impaired memory function overall. On delayed recall, more than half (53.8%; n = 14) of these patients showed at least mild memory impairment (HVLT-R delayed recall z ≤ −1.5). Perhaps most striking, nearly half (46.2%; n = 12) of these patients displayed at least moderate impairment (HVLT-R delayed recall z ≤ −2.0) and 5 (19.2%) of them displayed severe impairment (HVLT-R delayed recall z ≤ −3.0). With respect to recognition discrimination, 10 (38.5%) of these patients exhibited at least mild impairment, 8 (30.8%) exhibited at least moderate impairment, and 1 (3.8%) showed severe impairment.
Results of Supplemental Analysis
Supplemental analysis was conducted to explore the question of whether patients who exhibited a similar magnitude of memory impairment (ie, mild, moderate, or severe) on the HVLT-R delayed recall trial would perform differentially on the SMMSE as a function of age and educational attainment. In total, 30 (9.8%) patients exhibited mild impairment on HVLT-R delayed recall, 71 (23.4%) exhibited moderate impairment, and 131 (43.1%) exhibited severe impairment. After grouping patients by this parameter, we split each group into 2 subgroups based on age and educational attainment (group 1: age ≤79 and years of education ≥16; group 2: age ≥80 and years of education ≤15) and conducted between-group analyses of SMMSE performance (see Table 5). In short, younger, more educated patients with memory impairment performed better on the SMMSE than older, less educated patients with a similar degree of memory impairment, although these differences reached significance only among moderately memory-impaired patients (t 24 = −2.54, P = .018; Table 5). As a group, those patients with moderately impaired HVLT-R delayed recall achieved a mean SMMSE score of 25.98 (SD = 3.1). However, mean SMMSE performance within the subgroup of younger, more educated patients rose to 28.25 (SD = 1.98), surpassing even the most stringent cutoffs employed in clinics.
Comparison of SMMSE Performance Among Memory-Impaired Patients Grouped by Age and Educational Attainment.

Abbreviations: HVLT-R, Hopkins Verbal Learning Test-Revised; SMMSE, Standardized Mini-Mental State Examination; SD, standard deviation.
a P < .05.
Discussion
Primary care clinicians are often the first to address patients’ anxiety over aging, emergent cognitive decline, and the subsequent risk of developing dementia. In spite of longstanding concern over its sensitivity, the MMSE is often utilized as a first-line tool in response to such complaints. The current study examined the utility of this widely utilized screening tool under conditions of standardized administration and scoring (ie, the SMMSE) 28 in response to the emerging literature and, more notably, public interest around early detection and prevention of dementia.
In the current study, more than half of the sample performed above the suggested MMSE cutoff score of ≤25 used in many clinics. Notably, more than half of these patients displayed moderately to severely impaired memory performance on more in-depth assessment (ie, HVLT-R relayed recall and recognition discrimination). Prior research suggests that memory impairment of this magnitude increases the risk for future diagnosis of dementia and is associated with functional impairments and diminished capacity for activities of daily living. 38 These findings strengthen the argument that primary reliance on the MMSE as a cognitive screening tool clearly leads to underdiagnosis and possible delay of care.
Although previous literature has suggested that raising the MMSE cutoff to 28 would improve sensitivity, 27 this did not appear to address the problem. In fact, in our study, using this method continued to result in a high false-negative rate (n = 39; 13%) which translates to 1 in 8 patients being misdiagnosed in the clinic. Of those patients, 43% showed impairment considered to be in the moderately to severely impaired range, again suggesting a strong likelihood of impaired functioning in daily life. Perhaps most striking, even among those patients who performed perfectly (30 of 30) on the SMMSE (n = 26), more than half (n = 14) exhibited at least mild impairment and nearly half (n = 12) displayed moderate to severe memory impairment suggesting increased risk of dementia.
When interpreting the significance of the MMSE score, research also suggests that the age and education level of patients must be taken into account. 22,23 Authors 24 –26 have proposed adjusting the cutoff score based on these patient demographics to improve sensitivity and specificity. Indeed, patients in our study who performed above suggested cutoffs tended to be slightly younger with higher educational attainment (see Table 1). However, raising the cutoff to ≤28 (the most stringent cutoff possible short of a perfect score) clearly did not adequately address the problem of undetected memory impairment (see Table 3), and younger, more educated patients were the most likely to surpass this cutoff in spite of documented memory impairment. Of the patients in our study who were younger than 80 and completed at least 4 years of college (n = 49), roughly half (n = 24) scored above 28 on the SMMSE. Despite their high SMMSE scores, these patients demonstrated mild memory impairment on more in-depth testing (mean HVLT-R delayed recall z = −1.64, SD = 1.50), with just under half (n = 10) showing moderate to severe memory impairment. Interestingly, our results suggested that being younger and more educated may serve as “buffer” against poor SMMSE performance particularly among patients experiencing moderate levels of memory impairment, as shown in Table 5. Thus, our data provided further indication that younger, more educated patients may be more likely “pass” the SMMSE well after the onset of progressive cognitive decline. These patients may be at particular risk for being missed by the SMMSE and other common screening procedures in the clinic due to the less demanding format.
Given that sensitive detection of memory impairment is paramount in the process of cognitive screening, our findings raise serious questions regarding the utility of the MMSE as the field moves further toward a more preventive approach to dementia in patient care. Reliance on the MMSE would possibly lead to erroneous reassurance about a patient’s cognitive risk and subsequently a lack of close monitoring in these cases. Within practice guidelines offered over a decade ago, Petersen and colleagues 39 called for close follow-up and monitoring of those diagnosed with mild cognitive impairment due to the increased risk of developing a dementia. Although these authors listed the MMSE as a supported Practice Guideline, our research and other subsequent data 15,18,19 suggest that more aggressive assessment should be considered instead or in conjunction with this instrument. Thus, our findings are consistent with prior research indicating that reliance on the MMSE, particularly for younger, well-educated patients, increases risk of underdiagnosis and missed opportunities for early treatment intervention. Our results also support the notion that more robust assessment of delayed recall has particular utility for cognitive screening, as this was the most sensitive memory parameter at milder levels of impairment.
The Montreal Cognitive Assessment (MoCA) 21 measure was introduced in 1996 and has been suggested to be a more sensitive screening tool due to increased memory and executive components. Although promising, findings have been mixed in recent studies. Hoops and colleagues 40 found the MoCA but not the MMSE sensitive to early features in Parkinson’s disease, while Kasai and colleagues 41 recently concluded that the MoCA was not superior to the MMSE in the detection of mild cognitive impairment within a group at risk of dementia related to small vessel ischemic disease. Thus, additional research examining these measures against more in-depth neuropsychological measures is needed for conclusion.
Although the lack of final diagnosis may be viewed as a limitation of our study, the objective of this analysis was to examine the ability of a widely utilized screening measure to detect memory impairment regardless of etiology. Because our key focus was the sensitivity of SMMSE to this core early symptom of dementia and amnestic MCI, our findings speak directly to the measure’s utility for early detection of these disorders independent of underlying cause. An additional limitation was that 67% of our participants were African American, and all participants were memory center referrals, limiting the generalizability of our findings to some degree.
In summary, the current report provides further evidence that the MMSE/SMMSE should not be utilized as a screen for mild cognitive impairment and is questionable as a sensitive detector of early dementia. Our data also underscored the necessity of more robust assessment of memory function—especially delayed recall—in cognitive screening. Although the MMSE maintains utility for brief assessment of global cognitive status and tracking of dementia, our results demonstrated that even a perfect or near-perfect score on the MMSE does not necessarily signal intact cognitive functioning. In fact, perfect or near-perfect scores appear to be routinely achieved by patients with moderate to severe memory impairment who are likely experiencing at least subtle decrements in daily functioning. Finally, adjusting MMSE cutoffs based on age and educational attainment appears to be of modest value and does not appear to result in sufficiently sensitive screening.
Footnotes
Authors’ Note
An earlier, preliminary version of this study was presented as a poster at the meeting of the Midwest Neuropsychology Group in 2012.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.