
Abstract
Background:
Caregivers of persons with dementia are stressed. Stressors not related to care recipients’ needs impact caregiver outcomes, yet are seldom reported. The purpose of this study was to report the most stressful events experienced by spouse caregivers of older adults with Alzheimer s disease during a 6-month period.
Methods:
31 caregivers completed the Most Stressful Event form, Patient Health Questionnaire (PHQ-9) and the Revised Memory Behavioral Problem Checklist (R-MBPC). Fisher’s exact test and two-sample t-test were used to compare Most Stressful Events between caregivers. ANOVA model tested whether the PHQ-9 and R-MBPC subscales differed by stressor.
Results:
Caregivers reported no stressors 21.5% of the time, 1-2 stressors 25% of the time, and 3 stressors 53% of the time with 318 stressors reported in total. Care recipient needs (30.2%), caregiver needs (26.7%), and decision-making (16.7%) were the most frequently reported stressors. Using a mixed effects model, there were associations between the Most Stressful Events and depression (p = 0.016), mobility (p = 0.024) and caregiver issues (p = 0.009) subscales of R-MBPC.
Conclusion:
Results can be used to develop targeted intervention and support strategies for spouse caregivers experiencing non-caregiving related stressorsas well as the traditional challenges with caregiving related issues.
Introduction
The fact that family caregivers of persons with dementia and Alzheimer’s disease (AD) are stressed, burdened, and have high levels of depression compared with the general population has been well documented. 1 –3 Caregiving stress and burden have been shown to be related to the care recipient’s functional characteristics (eg, need for assistance with personal care like bathing, toileting), severity of their cognitive, behavioral, or psychological symptoms (eg, agitation, aggressive behavior), and level of depression. 2 Additionally, stressors not directly related to the care recipient’s needs will also impact caregiver stress, yet these are seldom addressed, measured, or reported in the literature. 4,5
Research assessing caregiver stress and burden has become more advanced. For example, we now know that caregivers’ appraisal of the stress may be more important than objective measures of stress per se. 6 –8 Yet, methods of assessing caregiver stress tend to vary across studies, and in most studies it is difficult to determine when caregivers are asked about issues of concern and if those issues change over time. 8 –10 Because a key feature of AD is the progressive nature of the disease, stressors can and do change and fluctuate over time, thus the timing of assessing caregiver stress may also impact the outcome. For example, what a caregiver finds stressful one day may not be what is most stressful the next day or week.
In order to examine the challenges that caregivers faced, as part of a clinical trial studying the impact of collaborative care for older adults with AD, 11 we asked family caregivers participating in the psychosocial educational support group the open-ended question, What are the 3 most stressful things in your life right now as a measure of their current stressors. Caregivers were asked to respond to this question each time they attended the psychosocial educational support group meeting and met with the advanced practice nurse (APN). The purpose of this study was 3-fold:
to explore the most stressful events (MSEs) reported by intervention caregivers over a 6-month period;
to examine the association between the caregivers’ MSEs reported and their depressive symptoms as measured by the Patient Health Questionnaire (PHQ-9) and the care recipient’s memory and behavioral problems as measured by the Revised Memory and Behavioral Problems Checklist (R-MBPC); and
to examine the impact of direct caregiving stressors and nondirect caregiving stressors on caregiver’s depressive symptoms (PHQ-9) and care recipient’s R-MBPC scores.
Methods
The data for this article were collected from caregivers participating in the monthly psychosocial educational support group meetings in the National Institute of Health–supported Collaborative Dementia Care trial that has been described in detail elsewhere. 11,12 Briefly, the intervention group received 1 year of care management by an interdisciplinary team led by an APN working with the care recipient’s family caregiver and integrated within primary care. All intervention care recipients and their caregivers were also invited to participate in voluntary monthly support group sessions. During these sessions, caregivers participated in a psychosocial educational support session led by M.G.A. that focused on education about AD and dementia, common caregiving stressors, including aspects of care that most caregivers report as stressful based on the literature and clinical experience. Caregivers were welcome to bring their care recipient with them to the support group. Following welcome and introductions, persons with dementia were taken to a nearby room for a chair-based exercise class led by a health psychologist and the APN. 11
Study Population.
There were a total of 153 dyads of care recipients and caregivers, 84 of these dyads were in the intervention arm of the trial. It became clear during the support group sessions that caregivers experienced a wide range of stressful events, many of which had little to do with direct care recipient issues. Indeed, some caregivers reported such complex social situations that those stressors appeared to be more challenging than issues directly related to the care recipient.
Procedures
Following every psychosocial educational support group meeting and during face-to-face contacts, the APN asked the caregivers to complete the following measures:
Patient Health Questionnaire 9 (PHQ-9) is a 9-item self-report measure that was used as measure of severity of caregiver depression. 13
Revised Memory and Behavioral Problems Checklist (R-MBPC) is a 24-item, caregiver report measure and a standard reliable measure of the frequency of cognitive, functional, behavioral, and psychological symptoms of the person with AD as well as a measure of the caregiver’s reaction to such symptoms. 14 It is an overall assessment of specific types of behavior problems including memory, depression, and disruption subscales. The scores of the R-MBPC are computed for the presence/absence of each problem first and then for caregiver “reaction” or the extent to which caregivers were “bothered” or “distressed” by each behavior. Reactions are assessed by asking how “upsetting” the behavior was on a Likert-type scale of 0 to 4. The R-MBPC has been widely used in various ethnic groups and demonstrated good reliability (with α of .84 for care recipient’s behavior and .90 for caregiver reaction) and validity. 14
Most Stressful Events was measured by asking caregivers to record, in writing, their responses to the open-ended question, What are the three most stressful things in your life right now? The item was asked by the APN at each visit. This item was introduced midway through our Collaborative Dementia Care study. A total of 318 stressors were reported from the 144 APN visits. The stressors were analyzed using qualitative content analyses. 15,16 Initially, M.G.A. and Y.Y.-F.L. worked independently to code selected session summaries and combined the findings for a preliminary list of categories, which were then entered into a database. Both M.G.A. and Y.Y.-F.L. met to review 20 items that showed disagreement in coding. Interrater reliability was approximately 95%. The major discrepancy was how to code items about “caregiver needs,” for example “having the hand brace and not being able to do what I need to do,” as it was not very clear whether the caregiver’s stressor was associated either directly or nondirectly with care recipient’s needs, however, we decided this stressor was most likely impacting the caregiving role and therefore categorized it as indirectly related to caregiving. Once M.G.A. and Y.Y.-F.L. reached consensus, the database was reviewed by M.G.A. and H.C.H. and based on similarities of content, the stressors were initially grouped into 9 detailed categories and then further combined to form 4 major categories for analysis: direct caregiving stressors care, indirect caregiving stressors, noncaregiving stressors, and no stressors.
Direct caregiving stressors included typical care recipient issues such as:
dealing with behavioral symptoms—agitation and repetitive behaviors worsening, hallucinations;
concerns about finances, for example, care recipient recently sold stock without telling her;
constantly having to monitor everything;
having to repeat everything constantly;
breaking partial dental plate;
care recipient went to jail recently; and
dealing with care recipient’s sleep problems, other health issues.
The indirect caregiving stressors, included issues that caused the caregiver concern, were related to caregiving but did not include direct hands on care:
decision making related to care such as selecting appropriate long-term care facility, for example, deciding when and where to move;
emotional issues related to care, for example, fear of losing care recipient after 62 years together;
family relationships are strained, for example, children are not visiting; difficult to get the family to agree on issues that need to get done; and
role transition process, for example, being responsible for everything, doing all the driving, having to get the car repaired.
Of particular interest to us was the impact that noncaregiving stressors might have on the caregiver’s symptoms of depression, anxiety, and physical health. Typical examples of noncaregiving stressors included:
caregiver’s feelings of stress trying to manage his small business;
other family member’s health issues, for example, daughter was diagnosed with cancer and was under treatment;
other family member’s financial and marital stress, for example, daughter was going through a divorce;
conflicted relationship with adult step-children;
financial concerns related to health care payments and reimbursement issues for their own health care;
granddaughter’s upcoming wedding and caregiver was asked to bake the wedding cake; and
concern about grandson’s problems and legal issues, for example, grandson currently in prison.
Although caregivers were not asked to rank order the 3 stressors in terms of severity, for this study, we used the caregiver’s first recorded stressor as the MSE in our analyses.
Statistical Analyses
Fisher’s exact test and 2-sample t tests were used to compare whether intervention spouse caregivers who completed the MSE form were different than caregivers who never completed the form. We used an analysis of variance (ANOVA) model to test whether the PHQ-9 and subscales of the R-MBPC differed by the type of primary stressor noted. Since caregivers had multiple visits, we used a mixed effects model with a random effect model for the caregiver to account for within caregiver correlations. Due to the skewness of some of the scales, we performed additional analyses transforming the scales by using the log (scale + 1). Since results were similar between the original scales and the transformed scales, we only report results for original scales.
Results
Caregiver and Care Recipient Demographics
Descriptive caregiver and care recipient demographics are included in Table 1. As indicated in Table 1, there were some significant differences between the caregivers completing the MSE form and those who did not. Caregivers completing the MSE form were on average 68.5 years old, more likely to be a spouse (80%), and had completed more years of education (13.1 vs 11.6 years; P < .05) than those caregivers not completing the MSE form. The nonattendees were more likely to be adult child caregivers and unable to attend support group meetings due to jobs and family commitments. Thus, this group of participants is most representative of spouse caregivers of persons with dementia and AD.
Caregiver and Care Recipient Characteristics.
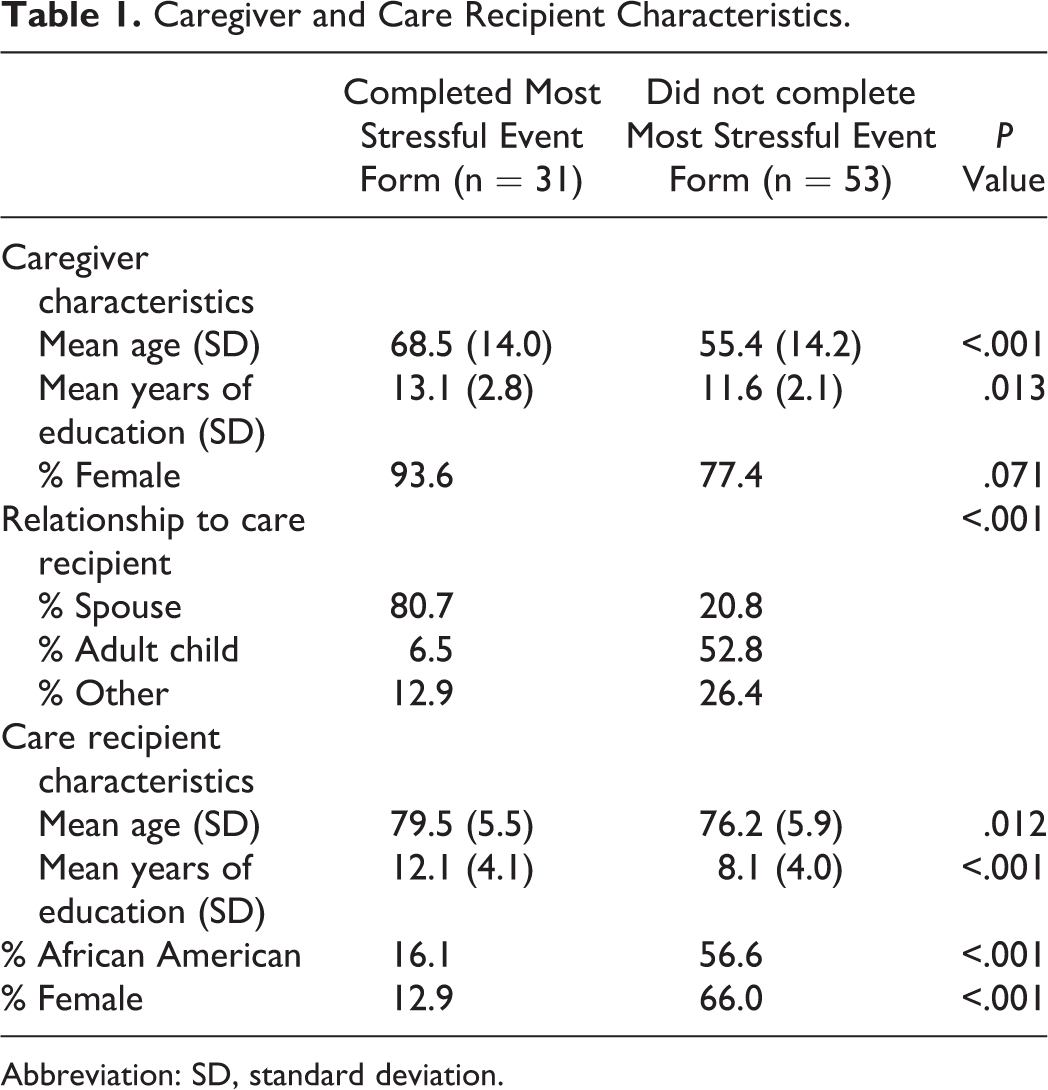
Abbreviation: SD, standard deviation.
There were 31 dyads that attended the intervention support group where they were administered the MSE form. They averaged 4.6 visits (± 3.4 visits) where they completed the MSE form and were followed for an average of 5.3 months (±3.4 months) and a total of 144 visits. Comparison of dyads who completed the MSE form and those that did not is presented in Table 1. Caregivers completing the MSE form were on average 68.5 years old, more likely to be a spouse (80%), and had completed more years of education (13.1 vs 11.6 years; P < .05) than those caregivers not completing the MSE form. The care recipients of the caregivers completing the MSE form were more likely to be male, white, older, and also have more years of education.
Caregivers’ MSEs
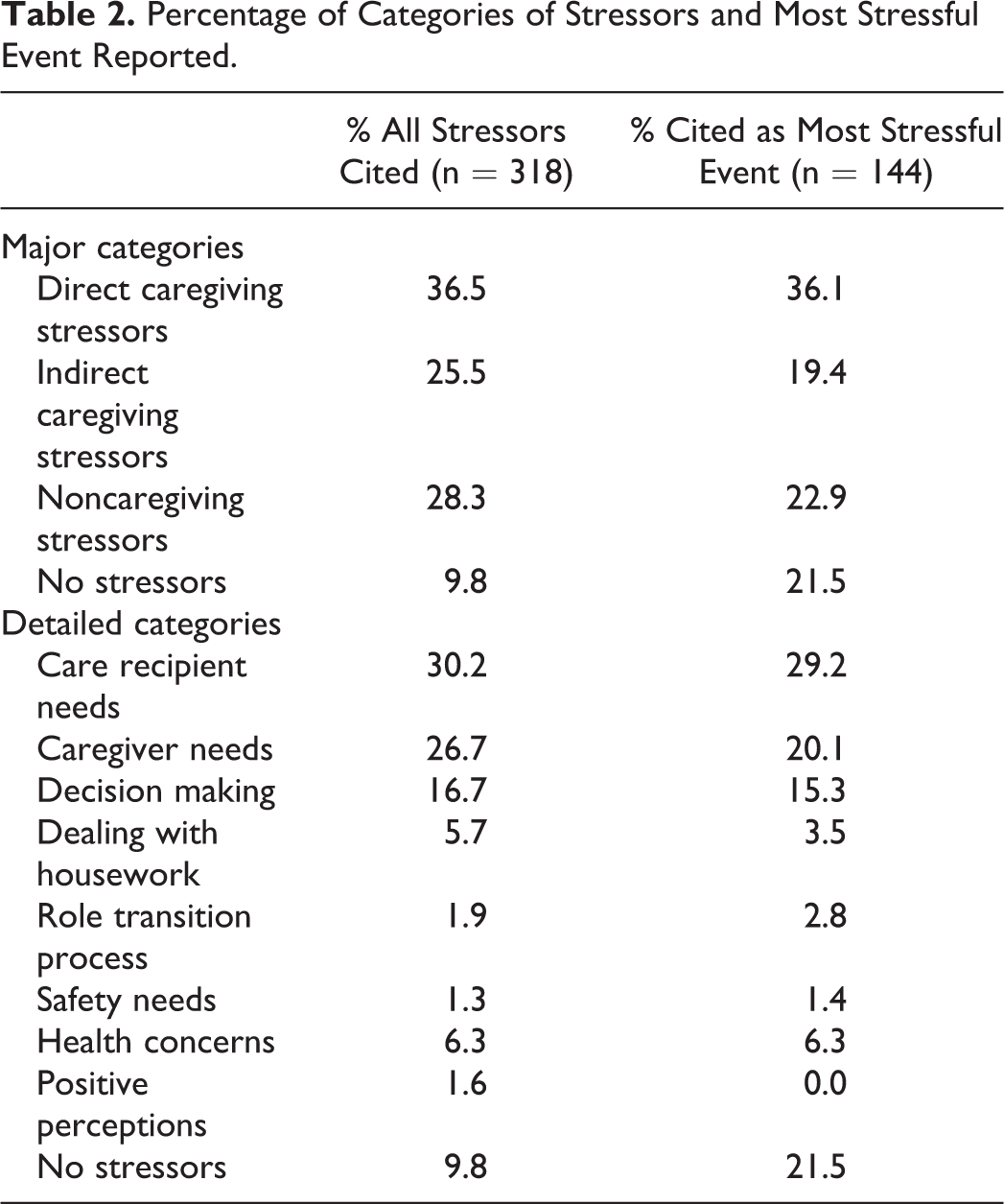
Table 2 summarizes the percentage of all stressful events reported, divided into the major and detailed categories, the percentage reported as the MSE, percentage of visits where stressors were reported, regardless of order, and the percentage of visits where caregivers reported any stressor. Of the 144 visits, caregivers reported no stressors 21.5% of the time, 1 or 2 stressors 25% of the time, and 3 stressors 53% of the time for a total of 318 stressors. For the major categories, direct caregiving stressors are reported most often by caregivers when using all stressors (36.5%) as the denominator and when using only the MSE (36.1%). A majority (78.5%) of caregivers report 1 of the 3 major categories at some time in the study. For the detailed categories, care recipient needs (30.2%), caregiver needs (26.7%), and decision making (16.7%) were the most frequently reported stressors. Approximately three-quarters (78.5%) of caregivers reported these 3 categories of stressor at some point in the study. Caregivers were likely to cite different MSEs over time. Only 10 caregivers cited the same major category as the primary stressor at all visits. In all, 10 cited 2 different categories, 10 cited 3 different categories, and 1 caregiver cited stressors across all 4 categories at different visits.
Percentage of Categories of Stressors and Most Stressful Event Reported.
Association Between Caregivers’ MSE, Depressive Symptoms, and the Care Recipient’s Memory, and Behavioral Problems
In Table 3, the mean scores on the subscales of R-MBPC are compared to the caregivers’ response to the overall category of the MSE. For all subscales, there were significant differences across the 4 primary stressor categories with the exception of sleep disturbance and repetitive behavior, when using an ANOVA model. Generally, those caregivers reporting direct-patient-related concerns had higher R-MBPC than those reporting other stressors. Using a mixed model to account for repeated visits by the dyads, only the patient mobility and caregiver issue subscales of the R-MBPC are significantly higher for visits where the MSE is a direct patient-related care issue. The PHQ-9 scores were also higher for caregivers reporting direct patient-related care as the MSE but did not reach significance. When we collapsed the major categories into 2 categories, direct caregiving stressors (n = 52) versus other stressors (n = 92); results were similar with 1 exception. The PHQ-9 was significantly higher (P = .034) for direct caregiving stressors (mean 3.8, standard deviation [SD] 3.8) than those with other stressors (mean 2.5, SD 3.1).
The Association of Most Stressful Event With Scores on R-MBPC Subscales.
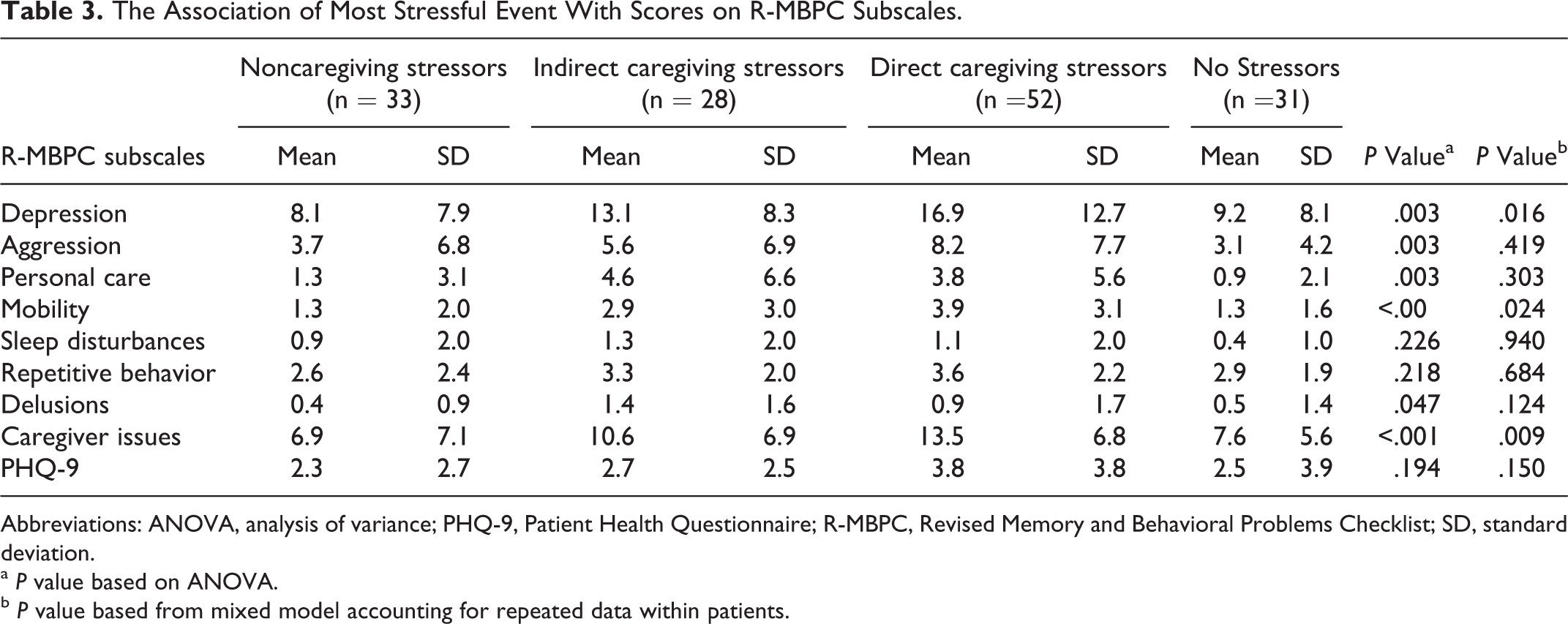
Abbreviations: ANOVA, analysis of variance; PHQ-9, Patient Health Questionnaire; R-MBPC, Revised Memory and Behavioral Problems Checklist; SD, standard deviation.
a P value based on ANOVA.
b P value based from mixed model accounting for repeated data within patients.
Impact of Direct Caregiving Stressors and Nondirect Caregiving Stressors on Caregivers’ Depressive Symptoms and Care Recipient’s Memory and Behavior Problems
Of those 52 visits where direct caregiving stressors were cited as the MSEs, specific issues included were care recipient needs (n = 39), decision making (n = 11), and safety needs (n = 2). To investigate whether care recipient needs (n = 39) was the sole reason for differences observed earlier, we compared care recipient needs versus all other stressors. As seen in Table 4, the t test results indicate 4 of the R-MPBC subscales including depression, aggression, mobility, and caregiver issues were significantly higher when the MSE was a direct caregiving issue. When analyses were computed using a mixed model to account for repeated data within caregivers, only the depression, mobility, and the caregiver issue subscales were significant.
The Association of Most Stressful Event With Scores on R-MBPC Subscales.
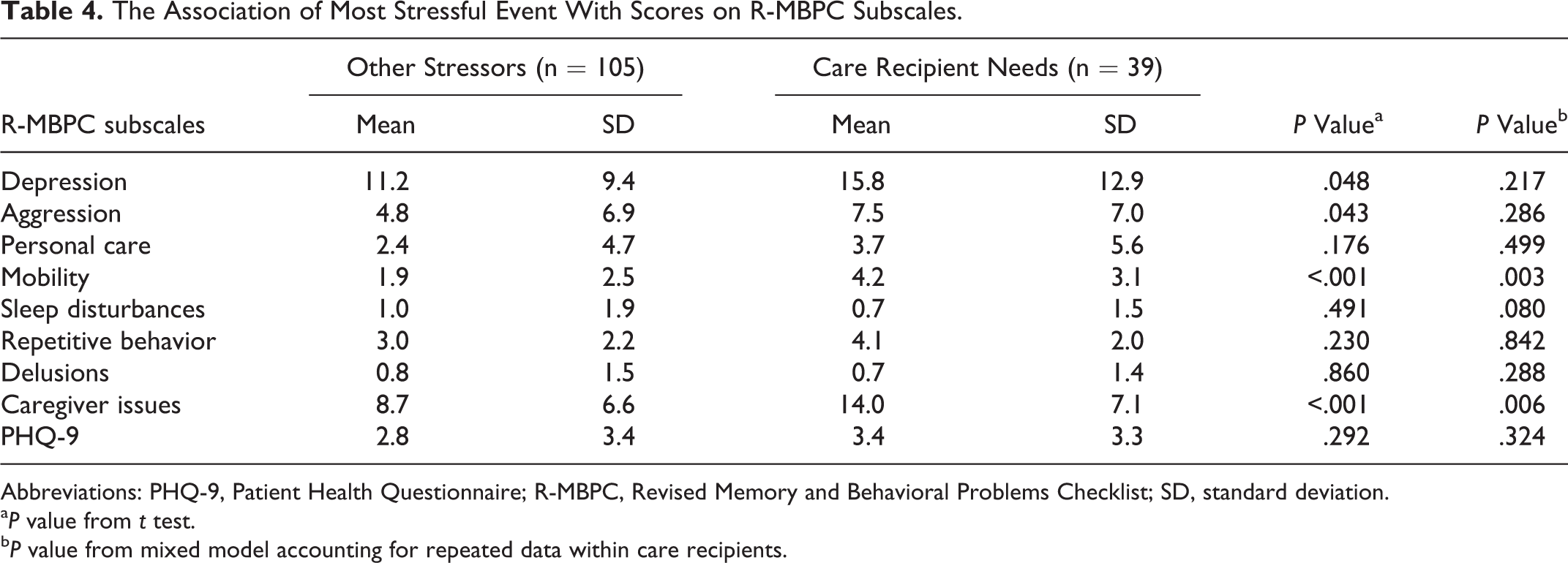
Abbreviations: PHQ-9, Patient Health Questionnaire; R-MBPC, Revised Memory and Behavioral Problems Checklist; SD, standard deviation.
a P value from t test.
b P value from mixed model accounting for repeated data within care recipients.
Discussion
In this study, using qualitative methods to identify the MSEs, we found that caregivers of persons with dementia and AD reported many types of stressors, including both direct caregiving stressors and noncaregiving stressors. Four categories of stressors were identified: direct caregiving stressors care, indirect caregiving stressors, noncaregiving stressors, and no stressors.
Noncaregiving stressors were almost as common as direct caregiving ones. These included dealing with concerns over other members of the family such as adult children’s health issues and marital distress and concerns about grandchildren’s well-being. Similar results have been reported by others. 17,18 Reported stressful events also differed over time supporting our premise that stressful events do change and fluctuate constantly. Approximately one-third of the caregivers cited the same type of issue as the MSE at all visits; another third of the caregivers cited 2 different types of issues, and the remaining third of the sample cited 3 different issues over time. One caregiver cited stressors in all 4 major categories at different times. It is important therefore that clinicians, service providers, and support group leaders be aware of the wide range of possible stressors that caregivers may be dealing with. It is likely that given the context of support groups for caregivers of persons with AD and dementia, unless asked directly about any and all stressors, caregivers may not offer this information freely.
Nevertheless, our findings also demonstrated that direct caregiving stressors remained the most commonly cited stressor for the caregivers in this study. Of the 144 visits and the 318 stressors reported, direct caregiving stressors were reported most often by caregivers (36.5%), with care recipient needs (30.2%), caregiver needs (26.7%), and decision making (16.7%) as the most frequently reported stressors. Similarly, our data also confirmed previous findings that addressing direct caregiving stressors, in at least 3 areas, is essential to caregiver education: providing care in general, dealing with the care recipient’s behavioral symptoms, and providing assistance for activities of daily living (ADLs). 18,19 Educating caregivers about direct caregiving stressors during support group meetings was especially helpful in this study as has been previously reported by others. 20,21 In fact, providing nonpharmacological interventions designed to assist caregivers in understanding dementia and AD to help them provide direct ADL care as well as addressing their own health care needs was the essential component of our collaborative care intervention. 11,12 Severity of patient symptoms in depression, aggression, mobility, and caregiver issue subscales of the R-MBPC, was significantly higher in those caregivers who reported direct caregiving stressors as their MSE. These behavioral symptoms have been associated with both caregiver depression and patient institutionalization. 22 –24 Behavior problems are quite common in dementia and are perhaps the most difficult stressor faced by the caregivers. Findings from previous psychosocial educational support and skill-building interventions have been shown to be effective in decreasing caregiver burden and increasing caregiver ability. 8 Similar to previous studies, we also found that due to the frequency of the care recipient’s behavioral symptoms, most commonly depression, agitation, aggression, and delusions, these behaviors were reported by caregivers as the MSEs, increased their burden and sleeping problems, and also taxed their ability to care for their care recipient. 25 –27
Caregiver depression scores were modestly correlated with stressor type. The PHQ-9 scores in caregivers who reported no stressors were lower, but not significantly so, as compared to those caregivers reporting any stressor. This was likely due to the fact that the caregivers in our sample were active participants in the monthly psychosocial educational support group, which was designed to increase caregiving skills and self-management. Although depressive symptoms have been the most widely used outcome measure in caregiver intervention studies and have a significant prevalence (25%-50%) in caregiver samples, it is by no means a universal problem for all caregivers. 22,24 These researchers report that between 50% and 80% of the caregivers do not have significant depressive symptoms and they might not benefit from an intervention designed to reduce depression.
It is only when a comparison was made between caregivers reporting direct caregiving stressors to those reporting noncaregiving stressors that we saw a significant difference in depression scores, which is similar to Farran’s pilot study findings, where care recipient’s behavioral symptoms were stable during the intervention. 18 During the monthly psychosocial educational support group meetings, sharing information about their stressors in a mutually supportive environment with other caregivers, while helpful, is not likely to be an effective treatment for major depression. 28 The potential benefits of support group interventions may also depend on other problems the caregiver has and whether there is a need for increased support over time. 29 Aside from the monthly psychosocial educational support group meetings, a major benefit of our collaborative care intervention was the APN’s involvement and her ability to tailor the intervention during one-on-one meetings with the caregivers and the immediate assistance in responding to their needs including assisting caregivers in addressing needs not necessarily related to the care recipient.
The findings of this study are similar to previous intervention studies, where caregivers have changed their behavior toward the person with dementia as a result of the intervention, because they have gained new knowledge, increased skills in assessing disruptive behaviors, learned the underlying causes of these behaviors, and improved their abilities to adapt to the change in the care recipient over time. 22,24,30,31 However, our findings are also unique in that we were able to identify stressors not related directly to caregiving, which had an impact on caregiver coping. It is important that all issues faced by caregivers be included in discussions when addressing caregiver coping skills, self-management skills, and improving their abilities to adapt to changes in any stressors over time. As reported, our caregivers’ MSEs changed over the 6-month period; therefore, clinicians and service providers should prepare caregivers for the fluctuations in care recipient needs over time, so that caregivers can feel better prepared by changes in care needs and less overwhelmed as the disease continues to progress. Teaching and coaching caregivers to anticipate changes in their own situations, as well as that of the care recipient, for example, jobs, concerns about extended family members, changes in their own health over time can help reduce the impact of noncaregivng stressors.
Limitations
Although the sample of 31 caregivers may not be representative of all caregivers, it is a good representation of spouse caregivers. Other caregivers such as adult children may have a different stress profile, but we were unable to measure this in this small sample. Indeed, caregivers who attend support groups may have less severe outside stressors and/or more resources and support to attend support groups. Although in our collaborative care trial we provided transportation and additional resources as needed for the intervention dyads, not everyone took advantage of the resources available. Also, the support group attendance was voluntary rather than mandatory, as we believed making attendance mandatory would add an additional burden to these caregivers. Another limitation in this study was that we did not ask caregivers to rank order their stressors in terms of severity. For the purposes of analyses, we used the first recorded stressor as the MSE. Finally, the MSE form was introduced halfway through the intervention as it became clear that caregivers were experiencing many different types of stressors. Thus, participants were already receiving what proved to be an effective intervention; introducing the MSE form at the beginning might have revealed different stressors.
Implications
Nevertheless, the results of this study can be helpful in developing targeted intervention and support strategies for caregivers experiencing various stressors in providing care. Given these findings, support services, either in clinical or community settings, could provide much needed education on understanding the progressive nature of dementia, how this will impact the care recipient and his needs over time, and how caregivers can prepare and learn strategies to manage stressful situations as they arise including both direct caregiving and noncaregiving-related stressors. In addition, teaching caregivers about the long-term needs and consequences of these diagnoses can help them to pace themselves over the long haul. Equally important is the education of caregivers about their own health care, health promotion strategies, and stress management techniques to reduce their level of stress and burden over time. Caregivers do not provide care in a vacuum. Caregivers come to their caregiving role experiencing both direct caregiving- and noncaregiving-related stressors. Open-ended interviewing techniques can be helpful in identifying all stressors that caregivers are dealing with and effective psychosocial education interventions can result in a reduction in caregiver burden, depressive symptoms, and improved care. Continued coaching throughout the course of the care recipient’s disease and teaching caregivers self-management skills, including the ability to identify the source of their stressors and utilizing available resources will mitigate the impact of those stressors.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by AHRQ RO1 HS10884. In addition, support was provided to MG Austrom by NIH P30AG10133 and to Y. Y-F Lu by NINR 1R21NR013755-01.