
Abstract
We aimed to determine whether there is an association between teaching and the development of progressive speech and language disorders (SLDs). Occupation was compared between 100 patients with a progressive SLD, 404 patients with Alzheimer’s dementia, and the 2008 US census. In SLDs, the most common occupation was teacher (22%) versus 8% in Alzheimer’s dementia. The odds ratio (OR) of being a teacher in SLDs compared to Alzheimer’s dementia was 3.4 (95% confidence interval [CI] = 1.87-6.17). No differences were observed in the frequency of other occupations. The frequency of teachers was higher in SLDs compared to the US census, OR of 6.9 (95% CI = 4.3-11.1). Farming, forestry, and fishing occupations were more frequent in SLDs compared to the US census. We identified an association between progressive SLDs and the occupation of teaching. Since teaching is a communication demanding occupation, teachers may be more sensitive to the development of speech and language impairments.
Introduction
The development of speech and language skills occurs during early childhood and is fundamental to participation in society. Typically, language function is maintained throughout life with the ability to communicate being preserved right up until death. There are, however, progressive neurological disorders that destroy various aspects of speech and language and hence communication. In some instances, communication becomes extremely challenging, as the patients lose the ability to express themselves as well as to comprehend others around them.
The patients with these devastating neurological disorders may report to their evaluating physicians with complaints such as “I can’t find my words,” “I can’t get my words out,” “I’m having trouble pronouncing words,” or “I am losing words.” In essence, the main problem affecting the patient’s ability to function in day-to-day life is the loss of communication skills. Neurological evaluation may identify speech production sound errors, grammatical errors, problems with comprehension, difficulty in naming simple objects, or loss of word meaning. These progressive neurological symptoms were first described at the turn of the 20th century. 1 Patients are typically diagnosed as having primary progressive aphasia, 2 aphasic dementia, 3 nonfluent aphasia, 4 logopenic progressive aphasia, 5 or primary progressive apraxia of speech. 6 Of importance is the fact that these patients are different from those patients with an Alzheimer’s dementia, in whom loss of memory for events is the primary problem. 7
Over the last 2.5 years, we have been recruiting adult patients with progressive aphasia and/or apraxia of speech due to a progressive neurological disorder for a study funded by the National Institutes on Deafness and Other Communication Disorders. Intriguingly, during the course of this study we have noticed that the occupation of many patients was, or had been, teaching. As a result, we performed a case–control study to determine if there is an association between the occupation of teaching and a progressive speech and language disorder (SLD).
Methods
All patients with a progressive SLD that presented to the Department of Neurology, Mayo Clinic, Rochester, MN, between July 1, 2010 and December 3, 2012 that met criteria for primary progressive aphasia 2 or apraxia of speech 6 were recruited into the study (n = 100). All patients were accompanied by a significant other, typically a close family member, and were seen by a study coordinator (SMP) and underwent a neurological examination by a board-certified behavioral neurologist (KAJ). Occupation for each patient was recorded independently by both the study coordinator and the behavioral neurologist with 100% agreement. Each patient also underwent a detailed speech and language examination and had recordings made of their formal speech and language assessment and general conversation by 1 of the 2 speech and language pathologists (JRD or EAS).
All patients underwent magnetic resonance imaging, which did not identify any structural or posttraumatic lesions, such as strokes or tumors, which could explain the progressive speech and language impairment. All patients had focal atrophy consistent with the diagnoses. None of the patients had any features of, or met criteria for, Alzheimer’s dementia 7 or any another neurodegenerative 4,8 or vascular dementia. 9 The study was approved by the Institutional Review Board of Mayo Clinic, and all patients consented for participation.
In order to determine whether there is a particular association between teaching and progressive SLD, we compared the frequency of teachers in our SLD cohort to 404 patients that fulfilled clinical criteria for a diagnosis of Alzheimer’s dementia. 7 The patients with Alzheimer’s dementia had been recruited between January 1, 1996 and January 1, 2006 in the Alzheimer’s Disease Research Center (ADRC) that recruits individuals seeking medical care in the Department of Neurology, Mayo Clinic, Rochester, Minnesota. Occupation was documented by study coordinators. By comparing our SLD cohort to the cohort of patients with Alzheimer’s dementia from the ADRC, we account for any institutional recruitment bias. The patients recruited into both the SLD and the ADRC cohorts are from different areas of the United States but predominantly from the Midwest.
The results from the SLD cohort were also compared to occupation data from the 2008 US census (http://www.census.gov/hhes/www/ioindex). Since the census data include only paid occupations, homemakers (all of which were unpaid) were removed from the SLD cohort before comparison to the census data. The unpaid homemakers were however included when the SLD cohort was compared to the Alzheimer’s dementia cohort.
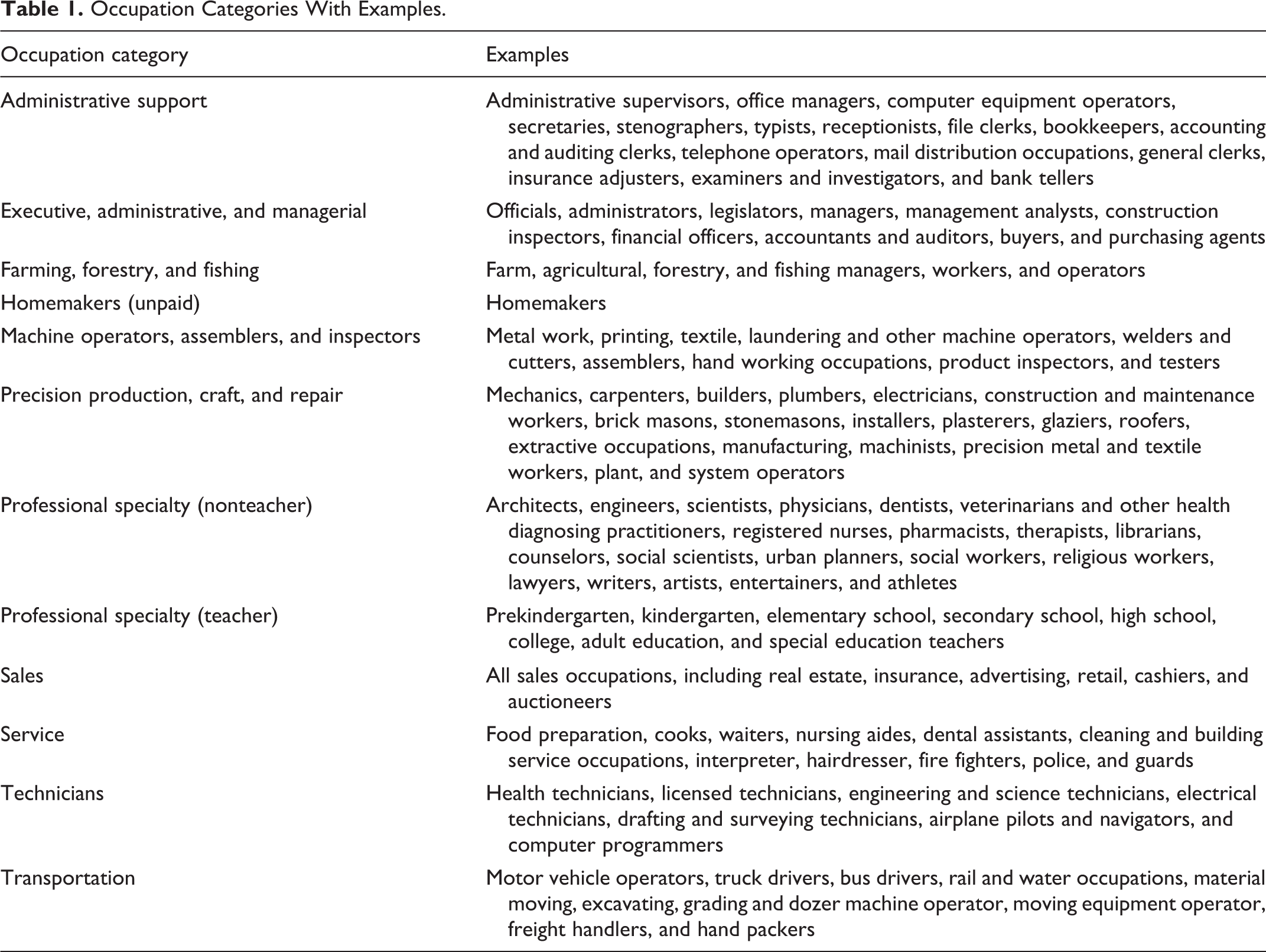
All occupations were grouped into 12 categories, as in Table 1, based on the categorization of occupations by the US Census Bureau. Chi-square analysis was used to compare the frequency of occupations between the SLD and the Alzheimer’s dementia and 2008 US census cohorts; Fisher’s exact test if small numbers. Bonferroni correction was used to adjust for multiple comparisons, with
Occupation Categories With Examples.
Results
Of the 100 patients with SLD, 53% were women. Average age at onset of communication difficulties (mean ± standard deviation) was 65.0 ± 8.4 years and education was 15.5 ± 2.7 years. Of the 404 patients with Alzheimer’s dementia, 58% were women. Average age at onset was 69.6 ± 8.8 years and education was 13.9 ± 3.1 years. Education and age at onset differed between the groups (P < .001).
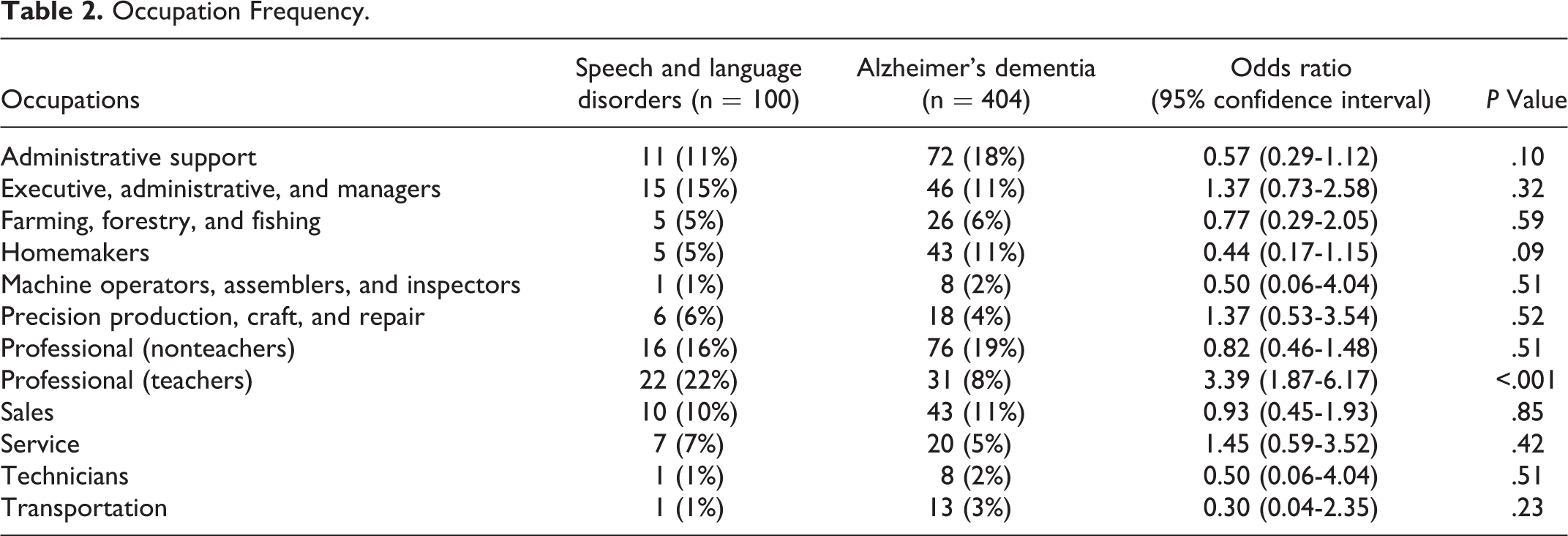
In the SLD cohort, the most common occupation was teacher (22%), followed by nonteaching professionals (Table 2). The occupation breakdown differed between the SLD and Alzheimer’s dementia cohorts (P = .01). In Alzheimer’s dementia, nonteaching professionals were the most common occupation, followed by administrative support workers (Table 2). Only 8% of the Alzheimer’s dementia cohort was teachers. The frequency of teachers was the only occupation that significantly differed across cohorts (Table 2). The OR of being a teacher in the SLD cohort compared to the Alzheimer’s dementia cohort was 3.4 (95% CI = 1.87-6.17). The frequency of teachers within professionals also differed across cohorts (P = .001).
Occupation Frequency.
The frequency of teachers in the SLD cohort was also significantly higher than the frequency of teachers in the 2008 US census (4%, P < .001; Figure 1). The OR of being a teacher in the SLD cohort compared to the US census was 6.9 (95% CI = 4.3-11.1). The only other category that differed between cohorts was farming, forestry, and fishing occupations which had a lower frequency in the 2008 US census (1%, P < .001) with an OR of 7.9 (95% CI = 3.2-19.3).
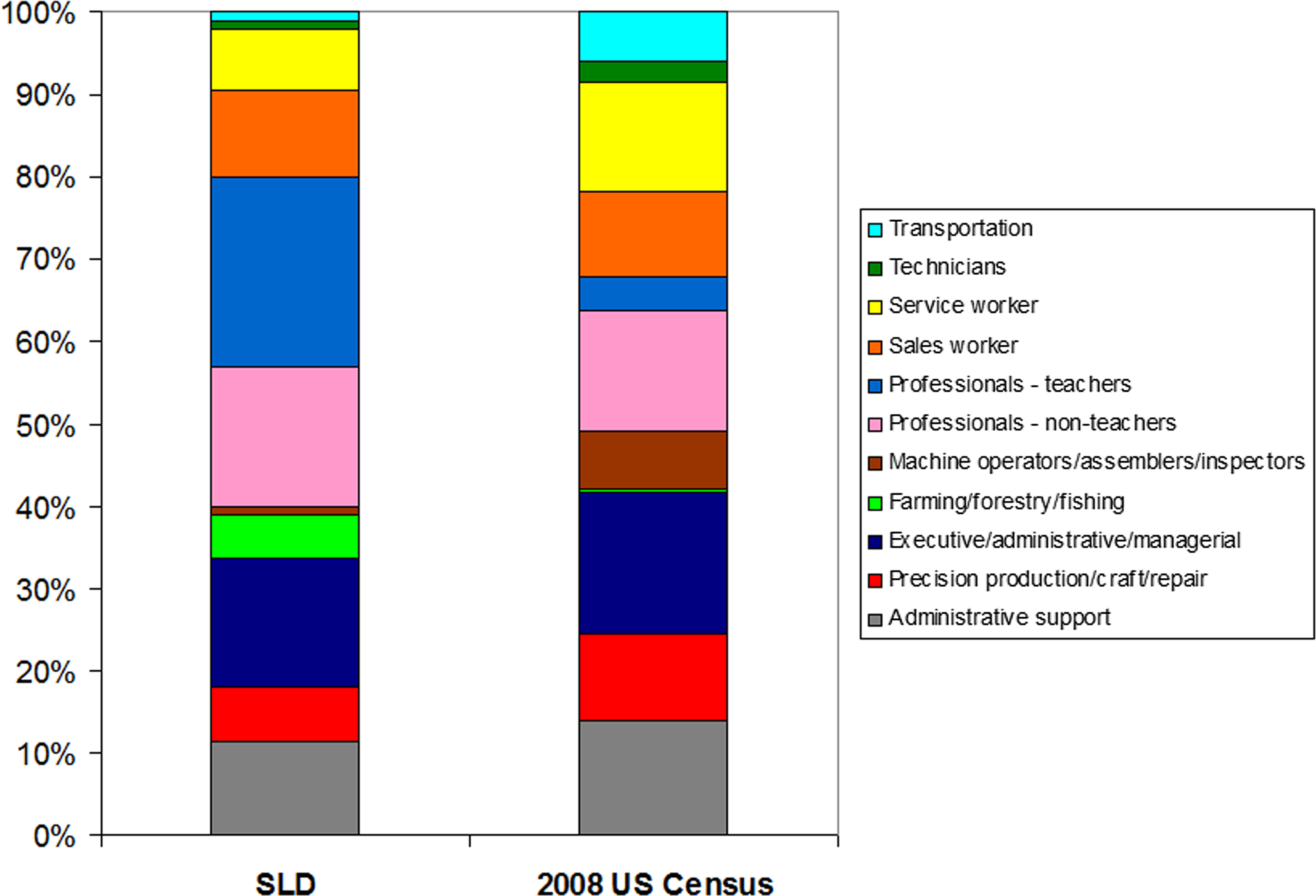
Occupation frequencies for the speech and language disorder (SLD) and 2008 US census cohorts. Plots include paid occupations.
Discussion
In our cohort of 100 patients with SLDs, almost a quarter were teachers, significantly higher than the proportion of teachers in a cohort of patients with Alzheimer’s dementia. In fact, patients with SLD were 3.6 times more likely to be teachers than patients with Alzheimer’s dementia. This finding suggests that there may be an association between progressive speech and language disorders and the occupation of teaching.
It is unlikely that this finding was confounded by a recruitment bias, since both cohorts of patients were recruited in a similar manner, from the same department and from the same institution. We do acknowledge that the patients evaluated at Mayo Clinic, and hence recruited into both studies, may be more likely to be professionals compared to the general population. However, we did not observe a difference in the frequency of professionals who were nonteachers between the SLD cohort and the 2008 US census or between the SLD cohort and the Alzheimer’s dementia cohort. Education could represent a bias, since it was higher in the SLD cohort compared to the Alzheimer’s dementia cohort. However, if this was the case, we would expect to see an overrepresentation of all highly educated professions in the SLD cohort, not just teachers. The fact that the frequency of professional nonteachers did not differ across cohorts argues against our findings being secondary to education.
It is difficult to determine why there is an association between teaching and the development of a progressive speech and language disorder. One possibility is that teaching requires continuous, daily verbal, and written communication, and hence teachers have more opportunity to observe changes in their speech and language. Similarly, teachers may be more sensitive to subtle changes in their speech and language abilities, because they are attuned to proper speech and language, and are constantly evaluating the spoken and written language of their students. Other professionals, while highly educated, may not depend as much on constant or correct or accurate verbal and written communication. Physicians, for example, while highly educated, typically communicate using abbreviations, modified sentence structures, telegraphic speech, and even incorrect grammar. We cannot entirely exclude the possibility that the development of progressive speech and language impairments are due to the continuous and daily use of verbal and written communication. However, there are other occupations that involve a similar amount of daily communication that were not more frequent in our SLD cohort. This latter argument is also contrary to the popular notion that “the more you use it the less likely you are to lose it” and the concept of cognitive reserve. 10 The difference observed between SLD and Alzheimer’s dementia could also suggest that teaching may in fact be protective for Alzheimer’s dementia. Although this is possible, the higher proportion of teachers in the AD cohort compared to the US census argues somewhat against this hypothesis. Additionally, the lower proportion of teachers compared to nonteaching professionals in the US census suggests that the lower proportion of teachers in the Alzheimer’s dementia cohort is typical.
Compared to the 2008 US census, the SLD cohort had a higher proportion of teachers, consistent with the differences observed with Alzheimer’s dementia but also had a higher proportion of farming, forestry, and fishing occupations. The latter finding is most likely driven by the fact that the Mayo Clinic is located in the Midwest where these occupations are common.
This study has important implications for early detection of progressive SLDs. A large cohort study focusing on teachers may improve power to identify the risk factors for these disorders.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was funded by National Institute of Health grants R01 DC010367 and P50 AG16574.