
Abstract
Aggression is a common form of behavioral disturbance in dementia. Strategies to prevent and treat aggressive behavior are underdeveloped. However, recent work points to several modifiable risk factors that may be targets for intervention. Pain management is an evidence-based, feasible, but potentially underused, strategy that may be incorporated with other behavioral interventions to prevent aggression. In this article, we review areas of overlap in interventions for pain and for behavioral disturbances and describe an intervention concept that may hold promise for older adults with dementia who are at risk of developing aggressive behavior.
Keywords
Introduction
Dementia is often accompanied by behavioral disturbances, a subset of which includes aggressive behaviors. Aggressive behavior has been defined elsewhere as an overt (ie, observable) act involving delivery of noxious stimuli toward others. 1 Aggressive behavior can be further subdivided into categories of physical aggression (eg, hitting, shoving, kicking) and verbal aggression (eg, cursing, threats of violence toward others). 2 When defined in these terms, aggressive behavior has an incidence of approximately 40% in people with dementia. 3 The origins of aggressive behavior in dementia are not fully understood but may be broadly conceptualized as a response to unpleasant internal or external cues that are interpreted as threatening. For instance, aggression is often linked to antecedents such as caregiving attempts (eg, aggressive resistance 4 or rejection of care 5 ). Potential costs of aggression include injuries to self and others, increased care costs, heightened risk of institutional placement, and greater potential for suboptimal care (such as use of physical restraints).
In clinical settings, aggression is most commonly treated with antipsychotic medications. These treatments have limited efficacy and are associated with high morbidity and mortality among people with dementia. 6 Thus, there is an urgent need to develop alternative approaches for management of aggressive behaviors in dementia. Because aggression frequently persists after its onset, 7 an ideal strategy is one that can prevent aggression before it occurs.
Current nonpharmacologic interventions to prevent and manage aggression are typically not specific to aggressive behavior but focus more broadly on behavioral disturbance, which may also encompass disruptive but nonaggressive behaviors. The interventions described in the literature are heterogeneous and may target the affected person, the caregiver/caregivers, and/or the environment. 8,9 Despite the variety of approaches, some common themes have emerged. In particular, interventions involving use of pleasant events have improved both mood and behavioral disturbance in people with dementia. 10 –12 Interventions that use environmental modifications, such as light therapy, 13 aromatherapy, 14 and modified bathing procedures, 15 have been shown to reduce behavioral disturbances including aggression. Most of these interventions target persons with dementia who exhibit emerging or existing problematic behaviors. Preventive interventions, particularly those targeting community-dwelling older adults with dementia rather than nursing-home residents, are underdeveloped.
Theoretical Basis for Nonpharmacologic Management of Behavioral Disturbance
The unmet needs model 16 provides a useful framework for understanding aggression and other forms of behavioral disturbance in persons with dementia. This model posits that behavioral disturbances are caused by the person’s unmet underlying biopsychosocial needs, which could be influenced by internal factors (eg, physical unmet needs such as pain or thirst) or external factors (eg, too much or too little stimulation provided by caregivers or by the physical environment). The unmet needs model acknowledges that disruptive behaviors including aggression are multiply determined and that many of their causes are mutable. Accordingly, a central focus of intervention is the caregiver’s ability to recognize and respond appropriately to the person’s unmet needs.
Needs-based interventions to address problems such as sleep, hunger, and communication difficulties have shown promise for reducing problem behaviors in people with dementia. 17,18 One limitation of these highly specific approaches is that they may not consistently address the underlying cause/causes of behavioral disturbance. Cohen-Mansfield and colleagues 19 demonstrated a broader application of the unmet needs model in a structured clinical intervention to manage behavioral disturbance in nursing-home residents with dementia. In contrast to many previous interventions focused on a single activity or environmental modification, the intervention was tailored to the individual’s apparent needs as determined through observations of his or her behaviors and use of a decision tree protocol. For instance, unmet needs such as physical discomfort, boredom, or restlessness were addressed through changes in the person’s environment, activities, medical care, or communication. The intervention, delivered systematically to 89 residents across 6 facilities, was compared to a placebo-control condition at 6 comparable facilities that received a staff education presentation. Despite a very brief intervention period of 10 days, verbal and physical problem behaviors in the intervention group were significantly reduced compared to those observed in the group randomized to the control condition (n = 78). This study, distinguished by its size and randomized design, provides promising evidence for behavioral interventions that target multiple underlying causes of behavioral disturbance, consistent with the unmet needs model. Whether a similar approach might prevent the onset of aggression and behavioral disturbance is unknown.
Using Evidence to Inform Preventive Strategies: The Case for Pain Management
Critical to a preventive approach is the identification of modifiable risk factors for the onset of aggression. Although some possible risk factors such as frontal lobe dysfunction are not currently treatable, observational studies have pointed to several risk factors that are potentially adjustable with treatment. These include pain, 3,20 –22 delirium, 4,23 depression, 24 psychosis, 25 –28 and relational problems in the caregiver–care recipient dyad. 3
A recent, 2-year, prospective study examined the risk factors for onset of aggression in 215 newly diagnosed older adults with dementia who had no prior history of aggressive behavior. 3 Significant risk factors in this cohort included pain, depression, caregiver burden, dyadic relationship problems, and lack of pleasurable activities. The hazard ratio for pain was greatest (1.41), followed by hazard ratios for caregiver burden (1.04) and caregiver–care recipient relationship quality (0.50). Hazard ratios for depression and pleasant events were significant in univariate regression models but not in a multivariate model, suggesting significant interrelationships among depression, pleasant events, and other risk factors. Whereas these risk factors may not necessarily cause aggression, they may be related to more proximal antecedents to aggressive behavior.
Pain is both common and undertreated in people with dementia and in older adults in general. Pain is present in approximately 50% of older adults with dementia in community and nursing-home settings, 29,30 but only about half receive treatment. 29 Other studies highlight systematic undertreatment of pain in older adults, especially those with cognitive impairment, 31 –35 despite abundant evidence to support pain management in these populations. Recent guidelines for pain management in older adults have emphasized pharmacologic treatment, 36 although evidence also supports the use of nonpharmacologic modalities such as relaxation, psychological intervention, and some forms of physical activity. 37 –39
The relationship between pain control and behavioral outcomes in dementia is not well established (for review, see Husebo, Ballard, and Aarsland 40 ). However, recent evidence suggests that improved pain control reduces behavioral disturbance. Husebo and colleagues reported that an 8-week stepwise analgesic protocol resulted in decreased behavioral disturbance among nursing home residents with moderate-to-severe dementia, compared to a usual-care control group. 41 Thus, optimal pharmacologic management of pain may have an important role in preventing behavioral problems.
Nonpharmacologic techniques for pain management overlap somewhat with interventions for psychological and behavioral symptoms. Pain is associated with mood disturbance and often co-occurs with depression in a cyclic, reinforcing relationship. 42 Thus, it is not surprising that treating depression has been shown to improve pain outcomes in older adults. 43 Several controlled trials support the efficacy of cognitive behavioral therapy (CBT) in reducing pain 44 and improving pain coping skills among older adults without dementia. 45 Similarly, behavioral self-management interventions are efficacious for older adults with pain 39,46 and depression. 47 Although these interventions may not directly translate to dementia care settings, some therapeutic techniques can be modified for people with dementia, particularly when a caregiver can provide coaching or assistance. For example, 1 uncontrolled study suggested that a CBT-based intervention tailored for long-term care residents with pain and dementia reduced pain, depression, and behavioral disturbance. 48
In summary, pain is significantly associated with development of aggression in people with dementia. Pain is highly prevalent in this population and is often not managed appropriately, making it an ideal target for efforts to prevent aggression and other behavioral disturbances. Depression is a second, related risk factor for aggression; and the frequent association of pain with depressed mood suggests that comanagement of these conditions may be an optimal strategy. Pharmacologic pain management in this population should be complemented by behavioral interventions to maximize pain control and address closely related psychosocial risk factors. However, the role of pain control in preventing aggression has not been evaluated, particularly in populations with no prior history of aggression.
Practical Management Strategies for Pain and Related Risk Factors
Teaching caregivers and, when possible, individuals with dementia to recognize and respond appropriately to pain and distress may help prevent the development of aggression and other behavioral disturbances. Below we describe several strategies for delivering these interventions to older adults with dementia and their caregivers.
Recognizing and Responding to Pain and Distress
Many caregivers lack skills to assess pain, particularly in noncommunicative persons. Eritz and Hadjistavropoulos 49 found that family caregivers’ reports of pain in older adults with dementia were unrelated to the nonverbal pain behaviors (eg, bracing, grimacing, etc) observed by the researchers. Informal caregivers may not consistently observe or consider such behavioral cues in their assessments of pain. Thus, interventions with caregivers should focus first on appropriate recognition of pain. Improved pain assessment alone improves management of pain in people with dementia. 50
The American Society for Pain Management Nursing has published guidelines for pain assessment in older adults with dementia who have limited verbal ability. Although the person’s self-report should be used as an indicator of pain whenever possible, other recommended pain-management strategies include searches for potential causes of discomfort and observation of the person’s behavior. 51 The same guidelines may also be applied to observing signs of emotional distress. Caregivers can be taught to recognize multiple behaviors that indicate pain and distress and to monitor nonverbal cues especially closely. Simple monitoring strategies, such as a pain and distress diary or checklist, can be developed and individually customized to help the caregiver appreciate the scope of the problem, identify important symptom patterns, and track outcomes. To better enable caregivers to engage patients with dementia in this process, communication skills training may focus on methods to increase the likelihood of successful communication. 52 –54 For example, caregivers may benefit from suggestions to minimize environmental distractions, monitor their own body language in addition to that of the other person, and use simple words that are meaningful to the care recipient.
Problem-solving approaches such as the serial trial intervention (STI) developed by Kovach and colleagues 55 offer a practical application of pain and distress monitoring. Interestingly, these interventions resemble techniques to manage behavioral disturbance in that their essential component is identification of possible unmet needs. For instance, STI and similar interventions frame behavioral disturbance as a symptom of distress for which the underlying cause may or may not be readily apparent. 55,56 Serial trial intervention is a stepwise process by which caregivers assess physical and sensory-affective needs and intervene appropriately until behavioral symptoms are reduced by 50% or more. 57 When taught to nurses and nursing assistants, STI, coupled with practical pain management techniques, appears to improve patient outcomes related to pain. 55,58 When similar behavioral problem-solving approaches have been taught to family caregivers, positive effects have been achieved in related outcomes, such as agitation and caregiver burden. 11
Psychoeducation
People with dementia and their caregivers may benefit from education about pain to better understand the rationale for pain management interventions, particularly nonpharmacologic management. Key teaching points include the bidirectional relationship between pain and emotional distress and the benefits of using a combination of pharmacologic and nonpharmacologic strategies. 42 This discussion may not only improve the recipients’ knowledge of pain treatment but also address compliance-related barriers to pain management, which are prevalent among older adults. 59 –61 For instance, fear of addiction to pain medication is a common but easily overlooked concern that can be addressed through psychoeducational intervention. 62 Older adults may also delay or minimize use of pain medication until discomfort is “bad enough,” 63 often stating fears that if pain medication is taken “too soon” it will not work “when I really need it.” These and other common pain myths 64 may have significant negative effects on older adults’ daily functioning.
Caregivers, in particular, may benefit from tools and coaching to advocate to health care providers when pharmacologic pain relief is inadequate. Studies examining proactive communication with physicians have shown that requests for clinical services (eg, a medication prescription or diagnostic test) were powerful predictors of “request fulfillment,” especially when a trusting relationship had been established with the clinician. 65
Nonpharmacologic Pain Management
Caregiver and patient interventions should incorporate education about behavioral management to maximize pain relief. Deep breathing for relaxation is a useful pain management technique that can be used with many older adults, including those with dementia. 66,67 Modified daily activity pacing and scheduling (eg, to avoid prolonged activity and allow time between activities for rest) is another simple behavioral strategy to limit provocation of pain and possibly reduce agitation as well. 68 Finally, education about body mechanics, support for difficult or complex movements, and appropriate body positioning can help caregivers correct unsafe or uncomfortable conditions. Ultimately, caregivers and people with dementia (when possible) should be encouraged to use a “toolbox” consisting of these and other behavioral strategies to manage pain.
Finally, increasing pleasant activity through behavioral activation is both a useful pain management strategy and an effective treatment for depression in older adults. 12,69 From a behavioral standpoint, engagement in activity offers access to potentially reinforcing stimuli and generation of positive affect. 70 For example, studies of nursing-home residents with dementia have found that expressions of positive affect are significantly more frequent during scheduled activity than during other periods. 71,72 Behavioral activation also directly counteracts avoidance that can lead to reduced environmental reinforcement and secondary problems such as deconditioning. This is especially important in the case of pain, as withdrawal and avoidance represent common maladaptive coping responses. 73,74 As an additional potential benefit, activity planning may improve the caregiver–care recipient relationship by providing the dyad an opportunity to increase mutually rewarding experiences. From a practical standpoint, activity planning may include introduction of pleasant activities or, for persons with greater functional limitations, modifications in the existing daily routine to increase opportunities for reinforcement.
Putting It All Together: An Intervention Concept to Prevent Aggression in People With Dementia
Nonpharmacologic interventions can potentially address multiple simultaneous risk factors for the development of aggression in patients with dementia, including pain, mood disturbance, and problems in the caregiving relationship. Already, promising evidence links nonpharmacologic interventions to fewer behavioral and psychological symptoms of dementia. Because of the strong relationship between pain and aggression onset, a greater focus on pain management may enhance the benefits of these interventions.
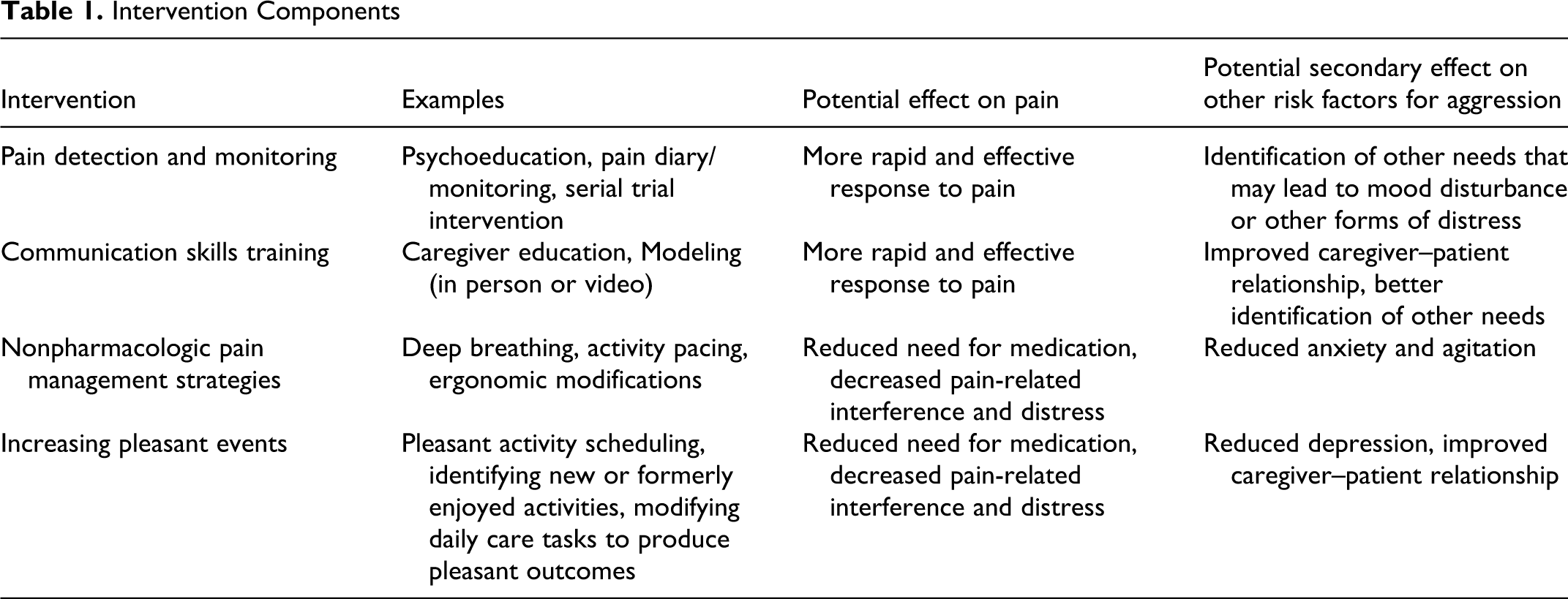
In practice, interventions should be relatively brief, skills-oriented, and delivered in the home or living environment to facilitate implementation. Importantly, caregivers should be educated and empowered to the greatest extent possible to improve their ability to identify signs of pain, employ a toolbox of nonpharmacologic pain management strategies, and advocate effectively to health providers on behalf of the person with dementia. Additional targets of intervention include the caregiving relationship and the care recipient’s mood and involvement in activities. Treatment goals may include improving identification of pain in daily activities, modifying the daily routine to make regular activities more comfortable and reduce interference from pain, and introducing (or resuming) new activities that are pleasurable and/or meaningful to the affected person. The interventionist can encourage caregivers to set concrete, realistic activity goals, with an emphasis on the care recipient’s enjoyment and engagement. The Pleasant Events Schedule-AD 75 provides a tool for brainstorming new activities. Additional treatment components may include discussion of communication challenges and suggestions for more effective communication (eg, modified use of language, breaking complex requests into simpler steps, changes in environmental distractions), with role-play or facilitated practice as indicated. The interventionist may also directly demonstrate techniques for effective communication and management of challenging behaviors. Table 1 describes several possible intervention components and how they might be applied to target both pain and other modifiable risk factors for aggression. Future research in this area should investigate the relationship between these broad risk factors and proximal antecedents for aggressive behavior. For example, severe pain in people with dementia has been linked to care-resisting behaviors, 76 which in some cases may escalate to aggressive behavior.
Intervention Components
Summary
Aggression and other behavioral disturbances in dementia are common, and the current typical approach to management is reactive rather than proactive. Nonpharmacological approaches to behavioral disturbance are in high demand and should be tested not only as treatment but also as preventive strategies. Behavioral interventions that cut across multiple risk factors for aggression have the potential to transform current practice and enhance the health outcomes of this challenging population. Emphasizing pain management, which is both common and widely undertreated in people with dementia, may enhance the efficacy and value of existing interventions to improve psychosocial outcomes and quality of life. Consistent with a goal of prevention, we advocate home-based interventions that target community-dwelling older adults and home-based caregivers, although residential facility staff and residents may also benefit from the approach we have described. Targeting people with dementia and known pain, even with no or minimal prior history of aggression, is crucial to confirming the acceptability and benefit of this shift to preventive management.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
This work was supported by Grant IIR009-351 from the Department of Veterans Affairs Health Services Research & Development Service and from support by the Veterans Affairs South Central Mental Illness Education, Research and Clinical Center. This work was also supported in part by the Houston VA HSR&D Center of Excellence (HFP90-020). The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs/Baylor College of Medicine.