
Abstract
Introduction:
At the end of life, patients with dementia often experience high levels of pain due to complex interplay of disease processes and numerous barriers to symptom management. In the hospice setting, informal caregivers play an essential role in pain management. This study describes their experience managing pain in hospice patients with dementia.
Methods:
We conducted a qualitative analysis of audio-recorded interviews with informal caregivers of hospice patients with dementia who had chosen pain as the challenge they wanted to work on within a problem-solving therapy intervention.
Results:
The thematic analysis of sessions with 51 caregivers identified 4 themes: difficulty in communicating with patients, lack of consistent guidance from health-care professionals, perceived uncertainty about the etiology of pain, and secondary suffering.
Discussion:
Our findings indicate the possible need for increased support for caregivers, including educational interventions targeting pain etiology and assessment, and improved communication with health-care professionals.
Introduction
In 2013, over 1.5 million people received hospice care in the United States. Of these, over 15% had dementia as their primary diagnosis, with many more having dementia in addition to other ailments. 1 Numerous health-care professionals have observed shortfalls in hospice care for patients with dementia, especially in the area of pain management. The Medicare Advisory Commission’s 2014 report to Congress highlighted the lack of data about the quality of hospice care for patients with dementia and included a call for research in this area. 2 Past studies have shown a mixed impact of hospice enrollment on pain management for patients with dementia. In a paired cohort study of long-term care residents with dementia, patients who were enrolled in hospice were more likely than unenrolled patients to receive pharmacological treatment for pain, even when both had standing orders for such treatment. 3 Even though access to pain medication may be improved for hospice enrollees with dementia, there is little evidence that these patients actually experience less pain than those without hospice services. In their survey of caregivers, Shega et al found that roughly half of caregivers reported moderate or severe pain for patients with dementia, irrespective of hospice enrollment. 4
In the general population of older adults with dementia, attempts to precisely estimate the prevalence of pain and quality of pain management have met with varied success. One study of long-term dementia care units found that 18% to 30% of patients self-reported pain, but prevalence of pain jumped to 34% to 48% when behavioral observation scales were used. 5 In a different study of patients with advanced dementia, pain prevalence ranged from 38.4% to 83.8% depending on which assessment tools were used by clinicians. 6 In the majority of clinical settings, self-report is the gold standard for pain assessment, but for patients with communication disorders and cognitive impairment, specialized tools have been shown to more effectively measure pain. 7 Throughout studies of pain in patients with dementia, self-report consistently gave the lowest estimate of prevalence, yet the majority of care providers and facilities still rely on self-report rather than standardized, clinically validated pain assessment tools. 8
Communication about pain can be extremely challenging for patients with advanced dementia, and the etiology of pain difficult to determine. In addition, patients may resist pain treatments due to their inability to understand the purpose of analgesia and may receive decreased benefit from analgesia due to the disruption of the placebo effect. 9,10 Pharmaceutical pain treatments may also exacerbate symptoms of dementia such as agitation and confusion. 11 The problems with pain management for patients with dementia lie not only in assessment and effect but also in the delivery of pain treatment. Studies comparing patients with dementia and patients with cancer have found that patients with dementia were prescribed lower doses of opioids than patients with cancer with similar pain scores, and opioids were more likely to be prescribed as monotherapy in patients with dementia, which is inconsistent with industry recommendations. 9,12
Dame Cicely Saunders, one of the founders of the hospice movement, identified pain management as the first priority of hospice, with the acknowledgment of suffering in patients and their families as the second. 13 Many of these family members can be referred to as informal caregivers, individuals who are essential to the delivery of hospice services but who often lack formal health-care training. A typical informal caregiver of a hospice patient with dementia will spend at least 46 hours per week assisting with basic and higher order activities of daily living, including personal hygiene, medication management, household chores, and transportation. 14,15 Informal caregivers are “on call” 24 hours a day and are at high risk for chronic stress, deteriorating physical health, financial difficulties, and premature death. 16 Informal caregivers have high rates of depression, anxiety, and grief, and in the few studies that have focused on their experiences, pain management for their charges has been the most commonly expressed concern. 17
In a survey of hospice nurses caring for patients with dementia, nurses reported frequently asking relatives to interpret patient’s pain signals and identified “knowing the life story of the patient” as one of the best tools for assessing pain, suggesting that informal caregivers may have some insights that professionals lack. 11 An experimental study comparing pain assessments by formally trained caregivers using a validated tool with assessments from informal caregivers after watching a video recording of their patient found little correlation between the assessments of the 2 groups. 18 A number of studies have highlighted communication about pain between patient and caregiver and between caregivers and clinicians as a recurring theme when caregivers are asked to describe their struggles; understanding the origin of this difficulty could lead to improvements in training. Many caregivers describe clinicians’ strategies for pain management as “mysterious” or “suspicious.” 13,19,20 These data suggest that informal caregivers have different strategies for managing pain than clinicians. It would therefore seem that a great deal could be gained from a phenomenological study of caregiver experiences.
In this study, we aimed to detect pain management barriers and challenges that informal caregivers of persons with dementia who identify pain as a challenge experience in the hospice setting.
Methods
In order to gain insight into the informal caregiving experience of pain management for patients with dementia in hospice, we utilized secondary data generated from a large randomized clinical trial testing the efficacy of a problem-solving therapy intervention for hospice caregivers. In the parent study, caregivers were recruited from 2 large hospice agencies in the Pacific Northwest. Inclusion criteria required that participants be designated informal caregivers of a hospice patient, older than 18 years, with at least a sixth-grade education, and ability to speak and read English, and caring for patients receiving home hospice services. Audio recordings were comprised of participants taking part in the intervention and discussing their caregiving experiences. 21 For our study, we analyzed a subsample of all participants, namely, only those who were caregivers of a patient with primary diagnosis of dementia and who had chosen pain as the challenge they wanted to work on within the problem-solving therapy intervention.
Thematic analysis was performed using audio recordings and transcripts. Data codes were inductively generated. A thematic analysis of the data was performed by the first author, and credibility of interpretations was checked by the second author. Transcript data were coded by line and sentence for descriptive (first level) and theme (pattern) codes. A list of major thematic elements was extracted by thorough study and coding of the interview transcripts. The analysis was organized into an expanding list of themes, arising from content, concepts, and descriptive categories. 22
Results
In the parent study, a total of 514 caregivers were recruited; of these, 172 were randomly assigned to an attention control group, 171 to an intervention group receiving the problem-solving intervention via face-to-face sessions, and 171 to an intervention group receiving the intervention via video calls. Of the 342 caregivers in the 2 intervention groups, 77 were taking care of a patient with primary diagnosis of dementia and 51 of them had chosen pain as the challenge they wanted to work on during the problem-solving therapy intervention. The audio recordings and transcripts of the sessions of these 51 caregivers provided the sample for this study.
Demographics of Study Sample
Table 1 summarizes the characteristics of the 51 caregivers and patients with dementia. The majority (82.4%) of the caregivers were female with an average age of 62.4 years, and 84.3% of them had been in the caregiving role for 3 years or more.
Characteristics of Caregivers and Patients With Dementia.a
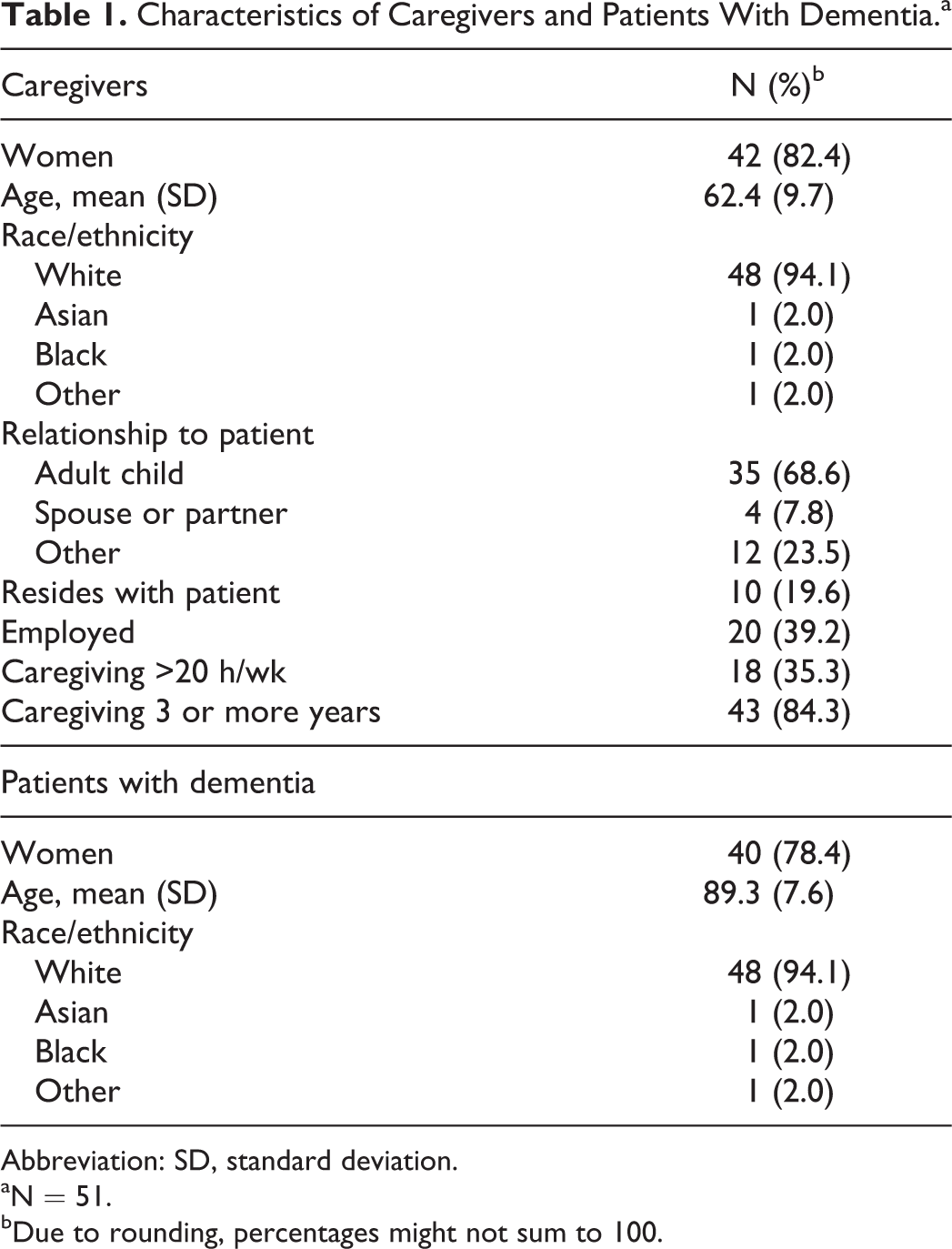
Abbreviation: SD, standard deviation.
aN = 51.
bDue to rounding, percentages might not sum to 100.
Qualitative Analysis
Thematic coding of sessions led to the identification of 4 distinct themes examining the pain management challenges that caregivers of patients with dementia face in the hospice setting, which are summarized in Table 2.
Four Themes of Pain Management Challenges Identified by the Thematic Analysis, With Descriptions and Example Quotes.
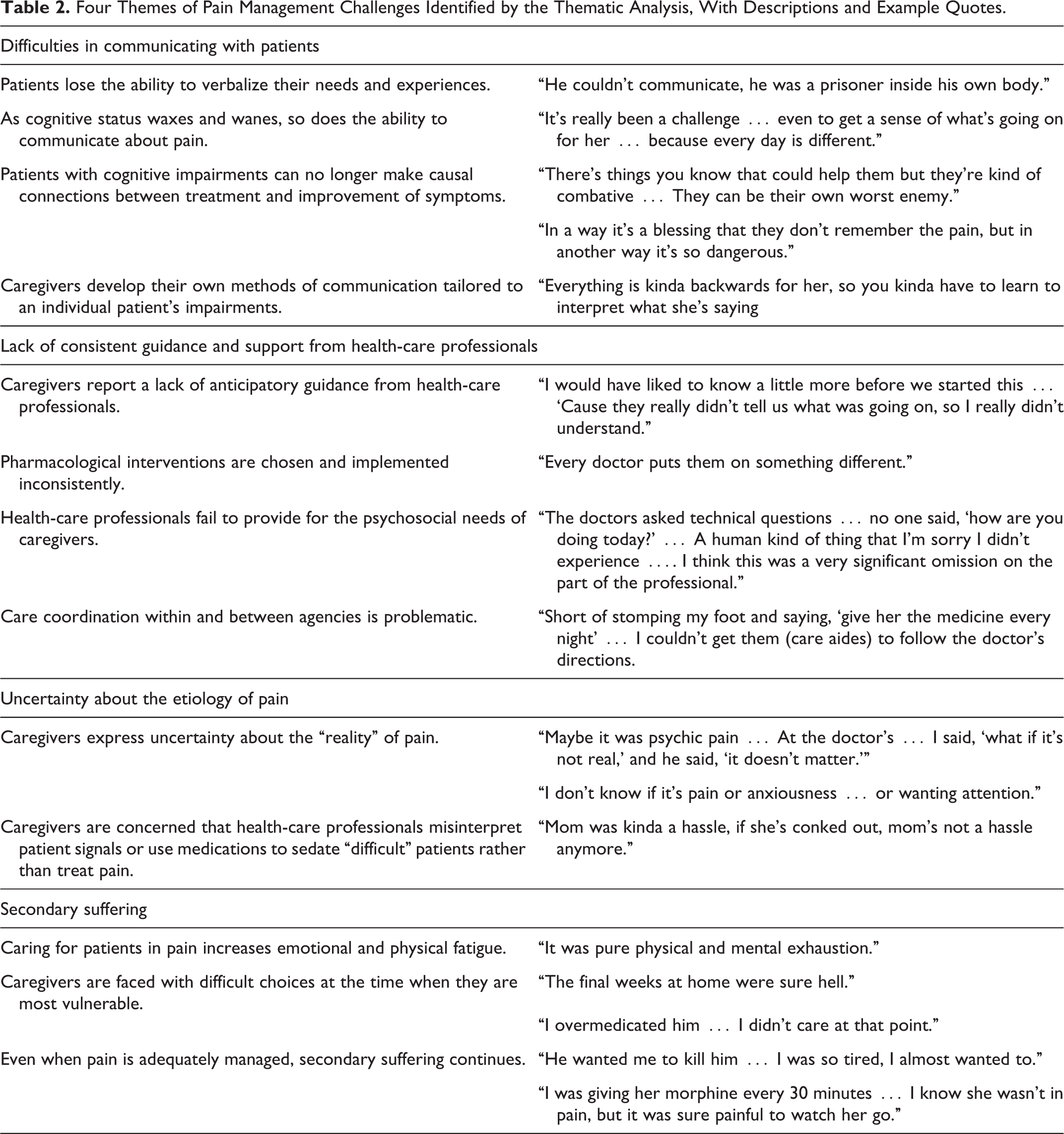
Difficulties Communicating With Patients
The first theme presented the challenges posed by the need to communicate with loved ones with dementia. Caregivers repeatedly described difficulties in gathering information about patient’s pain due to the patients’ aphasia, both receptive and expressive. Feelings of frustration and defeat characterized caregivers’ descriptions of how patients’ cognitive deficits and emotional lability prevented them from communicating about their internal states. Multiple participants described patients as “prisoners” inside their bodies, empathically assuming that their loved ones with dementia were as troubled by their inability to communicate as they were. Whether or not this was the case, imagining their loved ones feeling trapped was greatly disturbing to them.
Another communication barrier reported by caregivers was the variability in patient behavior and mental status. Patients stated that as cognitive status waxed and waned, so did patients’ ability to communicate about pain so strategies that “worked one day would be useless the next.” Perhaps most difficult of all was the fact that many patients were unable to make causal connection between treatments and pain relief, which prohibited effective communication. Caregivers stated that patients were combative because they could not understand that interventions were meant to help them, or that they forgot about past pain, and so rejected attempts at assessment and treatment.
In spite of the many barriers, participants showed great creativity in their communication methods. Participants described making up “new languages” to talk about pain, learning to interpret disordered speech, and using nonverbal cues to assess pain. Without formal training or access to validated clinical assessment tools, resourceful caregivers were able to draw on their personal histories with patients to gather information about their experience of pain. For example, one caregiver reported she could always recognize that her mother was in pain because of a specific way she would move in her chair. Another participant described that he knew when his wife was in pain when a home care aide would give her a bath because in these instances she would be squeezing the aide’s hand. He specifically commented on the importance of learning to interpret such signals over time that someone else may not be able to detect.
Lack of Consistent Guidance and Support From Health-Care Professionals
The second theme pertains to the communication between caregivers and health-care professionals and, more specifically, the lack of consistent guidance and support from health-care professionals. Caregivers reported a lack of guidance from health-care professionals in what to anticipate during the hospice trajectory and a lack of proactive communication especially related to pain. Participants reported being surprised by the severity and intractability of pain in their loved ones with dementia and stated that professionals rarely addressed pain in their assessments. These comments most frequently referred to care received before patients were enrolled in hospice, but even after enrollment, many caregivers stated that hospice nurses, physicians, and other health-care providers failed to provide anticipatory guidance about potential pain crises or prepare them for managing pain.
Participants identified many instances in which pharmacological interventions were chosen and implemented in a manner that was perceived by caregivers as inconsistent. Receiving conflicting prescriptions from different providers and struggling to understand the rationales behind varying treatments contributed to a mistrust of health-care professionals. In addition, a number of caregivers stated that orders for pain interventions were unpredictably implemented by paid care staff in adult family homes and skilled nursing facilities. Finally, many participants shared their dissatisfaction with health-care professionals’ lack of attention to their psychosocial needs. A frequent sentiment was that providers never asked about the informal caregiving experience or offered support or recognition of the emotional toll of managing their loved ones’ pain, further contributing to a lack of trust between caregivers and health-care professionals.
Uncertainty About the Etiology of Pain
Perhaps the most surprising finding of this study was how frequently caregivers stated that uncertainty about the etiology of patients’ pain caused them great anxiety and inhibited their ability to provide care. Multiple patients explained that they couldn’t differentiate between “real” and “imagined” pain due to communication barriers and a lack of obvious physiological causes. The modern clinical definition of pain is whatever the patient says it is, and clinicians, especially those in the field of hospice, are trained to treat pain symptoms even when they are unable to determine the cause, but laypersons have rarely been educated about this approach. 23 This mismatch between clinical approaches to pain, and the popular conception of pain as a clearly definable response to a singular ailment or injury, was present in numerous caregiver narratives.
Participants reported that they were troubled by providers prescribing medications to treat pain, which may or may not have been “real,” because it did not have an obvious cause, even when patients were manifesting signs of distress commonly associated with pain. This led some informal caregivers in the study to see administration of pain treatments as chemical restraints. A lack of understanding of the necessity of managing pain even when etiology is unknown contributed to some participants’ interpretation of clinically valid pain treatment protocols as attempts to sedate “difficult” patients.
Secondary Suffering
The fourth and final theme described what we labeled as “secondary suffering,” namely, the impact of pain management on caregivers themselves including both emotional and physical implications. Caregivers reported exhaustion and in many cases a sense of resignation after having experienced prolonged periods of stress and fatigue. Participants described the mental anguish of empathizing with a loved one in pain and the physical burden of providing pain treatments at the end of life.
Discussion
Our findings indicate that caregivers of persons with dementia in hospice face numerous and significant challenges when it comes to managing their loved ones’ pain. Several studies have already demonstrated that the needs of people with dementia at the end of life are not fully met and that caregivers require more support at this time as they may feel exhausted and alone. 24,25 Furthermore, while communication between health-care providers and caregivers is important, it does not often take place at times of crisis, affecting overall quality of care. 26 Our findings provide insight into concrete barriers to and challenges of pain management. Caregivers described uncertainty about the etiology of pain, difficulties in communicating with patients, lack of consistent guidance from health-care professionals, and secondary suffering as the factors that prevented them from properly and effectively managing pain in their loved ones. Thus, these findings indicate the possible need for increased support for caregivers, including educational interventions targeting pain etiology and assessment, and improved communication with health-care professionals.
Previous studies of informal hospice caregivers’ experiences with pain management have identified concerns about addiction as a barrier, but this theme was not present in this study’s sample. Likewise, concerns about the potential for overdose were not observed in our participants’ narratives. This may be due to this study’s focus on dementia, as caregivers may believe that addiction or overdose are less likely in this population or may be more worried about other issues related to pharmacological pain treatment. Whatever the origin of this difference, clinicians may need to adjust their educational techniques for informal caregivers with dementia based on these findings.
Our study findings can inform the training of hospice health-care professionals in order to prepare them to provide more effective and comprehensive support for caregivers and patients. Such training would provide tools not only to assess patients’ pain but also to improve communication with caregivers and empower them to effectively manage their loved one’s pain and to find appropriate help when needed. Training initiatives need to also address the issue of culture, which affects both the actual assessment of pain-related cues among patients and also caregivers’ attitudes and beliefs about pain management at the end of life. 27 Zborowski introduced in the early 1950s the notion that pain is not only a neurological and physiological but also a cultural experience highlighting how culture impacts the emotional, linguistic, and behavioral responses to pain. 28 Riley et al found increased expression of nonverbal pain behaviors in cognitively intact African Americans when compared to white counterparts. 29 Ford et al identified ethnic differences in the expression of pain words among older adults with dementia. 27 These studies demonstrate the need for the development of tailored approaches to care for ethnically diverse persons with dementia and their family members.
Study limitations include the focus on only one geographic region of the United States and a sample of participants with limited racial or ethnic diversity. Furthermore, participants had already agreed to participate in a clinical trial examining ways to support hospice caregivers, which may further limit the generalizability of findings to the general hospice caregiver population. In spite of these limitations, findings do provide an in-depth insight into caregivers’ experience with pain of a person with dementia in hospice and can inform the design and implementation of future educational or other interventions.
Implications for future research include the need to develop educational interventions for family caregivers to more effectively communicate with providers and support pain management of a loved one in hospice. Furthermore, communication strategies are needed to improve health-care providers’ information exchange with families, and tools need to be developed to assist providers in the delivery of culturally congruent family-centered care that addresses caregivers’ needs and concerns related to pain management.
Footnotes
Acknowledgments
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Nursing Research or the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Nursing Research Award Number R01NR012213 (Principal Investigator: G.D.) registered as clinical trial record NCT01444027.