
Abstract
Background
Interventional pain procedures (IPPs) may be necessary for some cancer patients when conservative treatment fails. However, many IPPs are often delayed or cancelled for cancer patients who are referred to the pain clinic.
Methods
We retrospectively analyzed the reasons for such cancellations to identify clinically avoidable causes of the delay in IPP.
Results
We enrolled 350 cancer patients who were referred to our pain clinic for an IPP between March 2016 and February 2018. There were 213 (60.9%) cases that were cancelled, among which 115 (54%) cases were potentially avoidable and 98 (46%) were unavoidable. The most common reasons for cancellation were patient-derived factors, which accounted for 85 (39.9%) cases. Patient refusal was a common reason for cancellation, with 33 (15.5%) cases attributed to this cause. The primary avoidable causes of cancellation were a recommendation that the patient continue with their current pharmacological pain treatment, conflict with another planned treatment, and pain characteristics that were not suitable for an IPP. Together, these accounted for 76.5% of all avoidable cancellations.
Conclusions
Comprehensive and accurate pain assessments before IPP may result in more favorable outcomes for the efficient use of medical resource and effective pain relief in cancer patients.
Introduction
Individuals with cancer are likely to experience critical pain from many sources including the tumor, chemotherapy, radiation therapy, and various other painful disorders such as herpes zoster and degenerative disease. These diverse forms of pain can have a significant impact on patients’ quality of life.1–3 Although conservative treatments such as pharmacotherapy and physical therapy may be sufficient for some patients, additional invasive interventional pain procedures (IPPs) such as nerve blocks and injection therapy may be beneficial for certain patients. For cancer patients, pain procedures reduce pain, and if they are used as part of a combined regimen for pain control, they can reduce daily analgesic use and, in this way, improve a patient’s overall quality of life.4–7
IPPs for cancer patients who are referred to the pain clinic are often delayed or cancelled. There are numerous reasons why pain procedures may be delayed, including patient preference, medical conditions, incomplete medical evaluation, and medical personnel-related problems. However, failure to perform pain procedures can lead to an inefficient use of medical resources and personnel, while a delay in pain procedures can inconvenience patients and their families, leading to dissatisfaction. Additionally, delays in pain procedures can interfere with the appropriate timing of pain management. 8
The purpose of this study was to analyze why certain cancer patients who are referred to the pain clinic for an IPP do not undergo the intended procedure. Ultimately, we sought to identify clinically avoidable reasons why IPPs are cancelled and provide solutions and recommendations to prevent these outcomes while also improving consultation efficiency.
Methods
Study population
This retrospective study was approved by the Institutional Review Board of Severance Hospital, Yonsei University Health System (No. 4-2018-0558). The requirement for informed consent by was waived, and patient records were anonymized and de-identified before analysis. The study population consisted of cancer patients who were referred to the pain clinic at our institution to receive IPP between March 2016 and February 2018. Data were obtained from a clinical data retrieval system at our institution and from typical consultation sheets that are used at the pain clinic.
Demographic and clinical data
Each patient’s medical chart was reviewed to obtain baseline data on demographics, cancer characteristics, and pain characteristics when the patient presented to our clinic. Patient demographic data included age, sex, body mass index, and Eastern Cooperative Oncology Group performance status (ECOG-PS; 0, asymptomatic, fully active; 1, symptomatic but nearly fully ambulatory; 2, ambulatory and capable of all self-care but unable to carry out any work activities, <50% in bed during the day; 3, capable of only limited self-care, >50% in bed but not bedbound; 4, completely disabled, bedbound). 9 The type of primary cancer, presence of distant metastasis, and history of chemotherapy or radiation therapy were also investigated.
Analysis of outcome assessments
For the purpose of this study, data were collected for the following variables: number of consultations for the intended pain procedure, number of cancelled cases, reason for cancellation, and type of admission. Reasons for failure to perform pain procedures were placed into one of five categories: (1) Patient; (2) Pain intervention; (3) Work-up/medical condition; (4) Facility/Resource; and (5) Pain physician.
In the patient category, the cancellations were due to patient (or family member)-directed refusal or postponement of the procedure. This category included patients who wanted and were recommended to continue to with their current pharmacological pain management regimen. Because pain intervention is not curative, invasive pain procedures should be avoided if the pain is tolerable. However, if there is a need for dose correction due to severe side effects, pain intervention could be considered, although a period of observation before proceeding to an IPP is generally warranted. Patients discharged early included patients who had left without providing notification, and if there had been earlier notification of discharge, appropriate schedule modification would have been performed.
The pain intervention category included cases of incorrectly indicated IPP. Patients with pain characteristics that were not suitable for intervention consisted of those patients whose pain would not be expected to subside with the intervention or where the procedure would be technically impossible. Examples include patients with multiple bone metastases, CNS metastasis, simple myalgia, pain due to abdominal distension, and catheter-related pain. This category also included patients who were not taking proper oral medication for pain control before attempting the intervention. 7
We performed a review of recent surgical history reports of patients who were scheduled for an IPP, which identified some patients who requested a consultation for intervention during the immediate post-operative phase. Cancer-related pain may be obscured immediately after surgery, and the surgery can cause many painful side effects. Thus, it is important that the patient be in an adequate general condition before undergoing any intervention. Similarly, a recent history of another pain intervention may raise the issue of whether the advantages of another intervention will outweigh the risk of side effects of their recent intervention. In our study, interventions were cancelled for several reasons including abnormal laboratory values that were contraindicated for the intervention and signs of infections such as high C-reactive protein (CRP) or suspicion of pneumonia on chest X-ray. 5 Other reasons for cancellation included contamination of the injection site, which made performing an intervention difficult due to the increased likelihood of infection.
In the work-up/medical condition category, reasons for cancellation of an IPP included incomplete medical evaluation and incomplete cancer work-up including patients requiring further workup for the source of their pain. It is important that interventions be performed after adequate evaluation of the cause of the pain because interventions can be invasive and may lead to unexpected side effects. Patients undergoing treatments such as radiotherapy or chemotherapy submit to a planned regimen based on their previously treatment and are continuously re-evaluated for intervention. Treatment in such cases is usually palliative rather than curative. Thus, it is reasonable that non-invasive procedures should be attempted first to avoid potential adverse effects such as infection, hemorrhage, and nerve damage. 10 The last component of the work-up/medical condition category was disease progression. Some patients in our study were unable to participate due to an inability to maintain proper posture, poor functional status, or increase in tumor burden and change in medical status such as cancer progression.
For the Facility/Resource category, there were some instances where no procedure room was available or the operating room was full, which led to postponement of the intervention. Another reason under the facility/resource category was the pain physician who referred cases where when the surgeon was not available.
Avoidable and unavoidable causes
The reasons for cancellation were assessed by consultation charts that were written by residents or clinical fellows after the patient interview and detailed chart review. The assigned pain clinic staff confirmed the reason for cancellation and added additional explanation if necessary by calling patients or through direct inquiry of clerical and clinical staff. For cancellations where the recorded reason was inconsistent with that reported by residents or clinical fellows, the assigned pain clinic staff initiated a detailed investigation to ascertain the true reason. Finally, a consensus was reached to avoid assigning more than one category to a single cancellation. This proved challenging given the complex nature of real clinical practice; however, two experienced pain physicians addressed this by agreeing to assign a root cause to a cancellation. Cancellations were further classified as potentially avoidable and non-avoidable. 11 Avoidable cancellations were defined as those cancellations that could have been avoided had there been adequate review of the patients’ medical records or better communication by hospital personnel before the patient’s consultation at the pain clinic.
Statistical analysis
Continuous variables are presented as the mean ± standard deviation (SD) and categorical variables are shown as the number (percentage). Descriptive and basic analytical statistics were used to summarize the data. The Pareto principle, which is also known as the 80:20 Rule or the Law of the Vital Few and Trivial Many, was used as a tool to identify and prioritize measures to improve effectiveness or safety.12,13 It is applied to quality control, and it states that roughly 20% of the errors cause 80% of the problems. With a small, wisely applied effort, a considerable reduction in problems may be reached. To prioritize future improvement efforts, we constructed a Pareto chart and identified the reasons that accounted for 80% of the avoidable IPP cancellations. All statistical analyses were performed using the Statistical Package for the Social Sciences, version 23.0 (IBM Corp., Armonk, NY, USA).
Ethical approval
This retrospective study was approved by the Institutional Review Board of Severance Hospital, Yonsei University Health System (No. 4-2018-0558).
Results
There were 942 people who were referred to our department during the March 2016 to February 2018 study period. The exclusion criteria included patients with non-cancer pain (n = 412), patient preference for non-intervention (n = 15), and insufficient data (n = 165). Finally, 350 patients were included in our study, of whom 137 patients underwent an intervention and 213 patients did not receive an intervention (Figure 1). The overall cancellation rate was 60.9%.
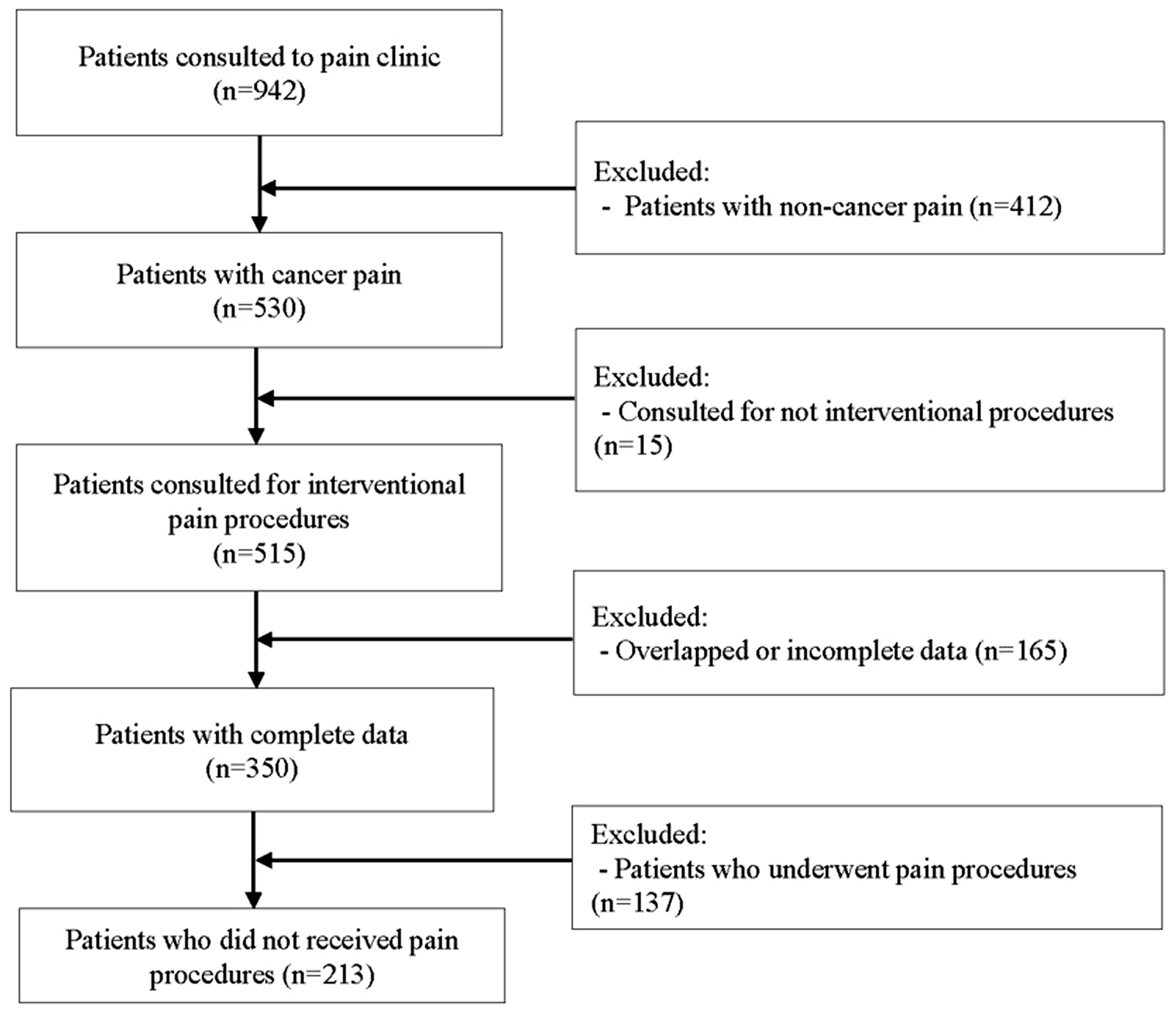
Flow chart of the study.
Among the 213 patients with a cancelled pain procedure, the average age was 60 years and the relative percentages of men and women were 41.8% and 58.2%, respectively. We found that 82% had an ECOG score that was >2, and 18% had an ECOG score <3. The most common type of cancer was upper gastrointestinal cancer (34%) followed by cancers of urological, gynecologic, colorectal, lung, and hematological origins (Table 1).
Demographics and cancer type about failure to perform IPP.

All data are presented as the mean ± standard deviation (SD) or the number of patients (%).
IPP, interventional pain procedures; ECOG-PS, Eastern Cooperative Oncology Group performance status; GI, gastrointestinal; GB, gallbladder.
The most common cancellation category was “patient”, which comprised 85 patients (39.9%), followed by “pain intervention” (n = 68, 31.9%) and “work-up/medical condition” (n = 57, 26.8%) (Table 2). The most common single reason for cancellation was “patient was recommended to continue with their current pain management” (n = 48). As shown in Table 3, other reasons included “Patient refusal of procedure” (n = 25), “other treatment planned” (n = 20), and “pain characteristics not suitable for intervention” (n = 20).
Frequency and percentage of IPP cancellations by category.

All data are presented as the number of patients (%).
IPP, interventional pain procedures; PTBD, percutaneous transhepatic biliary drainage; PVP, percutaneous vertebroplasty; EUS-CPN, endoscopic ultrasound‐guided celiac plexus neurolysis; CRP, C-reactive protein; INR, international normalized ratio; ESR, erythrocyte sedimentation rate.
Reasons for failure to perform IPP stratified by avoidable and unavoidable causes.

All data are presented as the number of patients (%).
IPP, interventional pain procedures; CRP, C-reactive protein: INR, international normalized ratio; ESR, erythrocyte sedimentation rate.
Among the 213 cancellations in our study, we found that 115 were potentially avoidable (54%) and 98 (46%) were unavoidable (Table 3). On the basis of the Pareto chart analysis, 76.5% of all cancellations were due to patients who were recommended to continue with their current pain management, having other treatment planned, or having a type of pain that was not suitable for the intervention. Thus, it may be important to focus on decreasing cancellation rates in these categories (Table 4, Figure 2).
Frequency and percentage of avoidable reasons for failure to perform IPP.

All data are presented as the number of patients (%).
IPP, interventional pain procedures.

Pareto chart of the avoidable cancellation reasons.
Discussion
IPP can be useful for cancer patients when conservative treatment fails. However, such pain procedures are often delayed or cancelled for many of the cancer patients who are referred to the pain clinic. In this study, we investigated the causes of such cancellations. We found that patient-derived factors were the most common cause of cancellations, which we attributed to the fact that the IPP focuses on conservative management rather than fundamental treatment. Thus, patients may be less likely to hesitate cancelling an IPP compared with a non-elective treatment such as surgery.
We attempted to identify the reasons for patient refusal of IPP. Although it was difficult to analyze the exact reason for refusal due to the retrospective nature of the study, we found that many patients expressed doubts regarding pain procedures due to their non-curative nature. Another common reason for patient refusal of IPP was anxiety about side effects. Many patients also expressed resistance to undergoing an invasive therapy, while others expressed negative feelings due to not having enough information about the procedure. Pain control for cancer patients is managed at cancer centers, with drugs, chemotherapy, and radiotherapy representing more conservative treatments. However, explanations about IPP are often only provided at the time of scheduling. Thus, it is imperative that patients are given enough information about the intervention because it is an important modality for managing cancer-related pain. Otherwise, because of a lack of information on interventions, many patients may become worried and subsequently resistant to the procedure, ultimately leading them to postpone treatment.
The most common unavoidable cause of cancellations was “Disease progression”. When a cancer reaches an advanced stage, patients often develop other medical problems that make IPP either difficult to perform or otherwise problematic due to potential side effects. Studies1,14,15 have shown that the incidence of pain increases with cancer progression, and many patients with pain that is caused by cancer are at an advanced disease stage. Similarly, the intensity of pain in advanced cancer patients is higher in patients with poor performance status. Consistent with this observation, we previously showed that in patients with pancreatic cancer, celiac plexus block has a better analgesic effect when performed in patients with early stage disease. 16 Although not all IPP can or should be performed early, timely IPP can be advantageous in certain cancer patients.8,16,17
The Pareto chart analysis revealed the following three reasons for avoidable potential intervention cancellation: 1) the patient was recommended to continue with their current pain management plan; 2) the patient had another treatment planned; and 3) the patient’s pain characteristics were not suitable for intervention. Identifying these key causes of cancellation in turn should allow for targeted efforts to decrease cancellation rates. Below, we briefly discuss the causes of these reasons for cancellation in patients with pancreatic cancer.
Patient was recommended to continue with their current pharmacological pain treatment
IPP are usually performed for patients with pain that is intractable to other therapies. However, when a patient’s pain is somewhat tolerable, intervention may not be warranted and their current therapy can be maintained. Specifically, invasive procedures always have potential side effects and it is advisable to not proceed with treatment if the pain is tolerable. Thus, before planning an IPP, it is imperative that a comprehensive pain assessment be performed. In addition, because individual pain scales may fluctuate on a day-to-day basis, it is important to closely follow the patient’s pain scale to prevent unnecessary procedure cancellation.4,7,8
Other treatment planned
Cancellations that result from a patient having another scheduled radiotherapy treatment, chemotherapy treatment, or palliative surgery were categorized as having another treatment planned. Planned cancer treatments, which may be more helpful in managing pain, should take priority over IPP.4,18
Pain characteristics that are not suitable for intervention
Finally, before performing an intervention, it is important to clearly elucidate the cause of the pain. It is important to be able to anticipate the outcome of the procedure and whether the specific cause of the pain is likely to be addressed by the intervention. 8 Whole body pain, catheter-related pain, abdominal discomfort due to distension, and pain due to edema, infection, or simple myalgia are not indications for IPP. Interventions are usually performed in cancer patients for neurogenic pain, but they cannot be used to address non-cancer-related and nonspecific pain.5,8 Therefore, it is important to diligently investigate causes of pain and rule out identifiable sources such as catheters. Physiological and psychiatric aspects of pain should also be evaluated. 14
Limitations
There were some limitations to our study. First, bias is unavoidable when categorizing cases with multiple factors to a single category. To reduce this bias, we conducted our study using a team consensus approach. Second, the accuracy of this study may have been compromised due to the sole reliance upon medical records. Finally, the approach to pain management in our study may not be applicable to every hospital, and thus, it is not clear how well our results can be generalized to other hospitals. However, there were several clear trends with respect to the reasons for cancellation of pain procedures.
Conclusions
Our study showed that the cancellation ratio for IPP in cancer patients was 60.9%. We found that 54% of cancelled cases were potentially avoidable, with the most common reason for cancellation stemming from the patient, who may have been recommended to continue with their current pain management, have another treatment planned, or have a form of pain that was not suitable for intervention. Our results suggest that a more comprehensive and accurate assessment of pain before attempting IPP may result in more favorable outcomes in cancer patients, especially as it pertains to the efficient use of medical resources and achieving effective pain relief.
Footnotes
Author contributions
Ki Wook Kim, Sang Jun Park: formal analysis, investigation, methodology, supervision, validation, writing, review, and editing; Shin Hyung Kim, Hun Jang: data curation, methodology, validation, and visualization; Ji Yeon Won: writing, review, and editing.
Availability of data and materials
The datasets that were generated and analyzed during the present study are available from the corresponding author upon reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.