
Abstract
This study utilized a community-based, participatory research model between the Association for Frontotemporal Degeneration (AFTD) and the Education Core of the Indiana Alzheimer Disease Center. A total of 30 caregivers of persons with frontotemporal dementia (FTD) participated in 6 focus groups in 3 cities. The majority of participants were spouses of the person with FTD and had been providing care for an average of 6 years. Transcript analysis revealed 7 prominent themes: willingness to participate, when/how the issue of brain donation is raised, who initiates discussion about brain donation, who is involved in decisions about brain donation, motivation for participating in brain donation, lack of effective communication, and barriers to research participation. Caregivers demonstrated a strong desire to participate in research and contribute to advancing knowledge. The lack of effective communication between the clinicians and caregivers was a barrier to developing positive rapport, detrimentally impacting research participation.
Introduction
Currently there is no published information describing attitudes related to brain donation among caregivers of persons with frontotemporal dementia (FTD). There have, however, been a handful of studies previously published that investigated this issue in persons with Alzheimer’s disease (AD). For example, Schmitt, Wetherby, Wekstein, Dearth, and Markesbery found that healthy elderly individuals who had signed up to be brain donors were influenced by knowing someone with AD, were referred to participate by someone already enrolled, and had a desire to promote scientific research. 1 Similarly, Garrick, Howell, Terwee, Redenback, Blake, and Harper 2 found in their Web-based survey of people involved in a brain donation program for research that the majority of donors were young, well-educated females. Most of their respondents indicated that donating their brain for science and to benefit mankind were important motivators, followed by “access to honest and accurate information” and “family illness” which was not necessarily AD as this was a generic organ donation program. 2 However, FTD is distinguished from AD in several key aspects, which may impact attitudes about brain donation among this group of family caregivers. Frontotemporal dementia is a heterogeneous disorder with younger age of onset than AD, prominent behavioral and/or language features, 3 and a current reported prevalence in persons 45 to 64 years from 15 to 22 per 100 000 person-years. 4 The duration of illness is shorter than AD, with current estimates for FTD ranging from 6 to 9 years 4 . In general, patients with young onset dementias are more likely to be misdiagnosed and experience a delay in diagnosis. 5 All these features would suggest that the demographics and concerns of caregivers and family members engaged in brain donation decision making may be different for patients with FTD versus AD (eg younger, employed spouses rather than retired spouses or adult children, frustrated with the health care environment after diagnostic challenges, and isolated due to the relative rarity of the condition) and warrant further investigation. Indeed, in a recent study investigating the needs, burden, and levels of depression and anxiety in a group of 30 caregivers of persons with AD compared with 30 caregivers of persons with FTD, the researchers concluded that needs of caregivers of persons with FTD were significantly higher than those of the AD caregivers. The increased needs were related to the younger age at onset of FTD, financial burdens, typical FTD behavioral characteristics, and lack of access to appropriate services, information, and support. 6
While knowing that these differences exist among caregivers of persons with FTD is important, there remains a void in our understanding of what caregivers of persons with FTD understand about the importance of biomedical research for this rare disease. To advance science and understand morphological and biochemical changes in FTD, it is important to understand caregivers' concerns and perceived barriers to research participation, particularly brain donation. Therefore, this study was undertaken to identify potential barriers to participation in brain donation programs among FTD families and to better understand the caregivers' attitudes, awareness, and understanding of research and brain donation.
Community-Based Participatory Research
Community-based participatory research (CBPR) is defined as “A collaborative approach to research that equitably involves all partners in the research process and recognizes the unique strengths that each brings. CBPR begins with a research topic of importance to the community and has the aim of combining knowledge with action and achieving.…change”. 7 Commonly acknowledged benefits of CBPR to researchers include an increased investment in and commitment to the research process by the study participants and facilitated participant recruitment and retention. Benefits for the community include assuming the role of “partner” rather than “subject” and having a voice in both study objectives and design, thus ensuring respect for the culture and goals of the community. Both partners gain from the increased likelihood that the project will reach a successful completion. 8
Community-based participatory research is especially relevant in the area of rare diseases, where the relatively small number of patients exacerbates the issues of grant funding, statistical sample size, and lack of interest from the biotech and pharmaceutical industries (traditionally, the largest source of funds for translational research). In this situation, it has been noted that advocacy organizations such as the Association for Frontotemporal Degeneration (AFTD) “can combine their ability to coordinate the communities of individuals they serve with the engagement of research scientists to drive forward research that is aimed at translational goals.” 9
This CBPR study was designed to identify attitudes about brain donation among caregivers of persons with FTD with the goal of understanding variables that may enhance participation in brain donation and those that serve as barriers in that process.
Methods
This study utilized a community-based, participatory research model between the AFTD, an international nonprofit support, education, and advocacy organization based on Radnor, Pennsylvania, and the Education Core of the Indiana Alzheimer Disease Center at Indiana University School of Medicine, an academic medical center in Indianapolis, Indiana.
Study Design and Recruitment
A caregiver committee was convened to advise the investigators on design of the focus groups and the project’s recruitment brochure, with a goal of maximizing caregiver participation. This group met by phone a total of 3 times. Focus groups were advertised via mailing of brochures and flyers to support group leaders and clinicians in the area, announcements on the AFTD Web site and in the AFTD newsletter, and e-mail notices sent to caregivers registered with AFTD. Respondents were mailed a demographic questionnaire in advance of their focus group meeting, and upon completion of the study were mailed a post questionnaire that queried them on their experience. Each participant received a $25 gift card as a token of appreciation for their time.
Focus Groups
Members of AFTD’s Medical Advisory Council were queried as to the barriers they perceived as they address the topic of brain donation with families of persons with FTD. Themes emerging from this brief poll (cost, religious and cultural proscriptions, emotional difficulty with the topic, lack of logistical support, and lack of planning ahead) were used to develop the semistructured interview questions for the focus group discussion. During the focus groups, caregivers were asked to answer the questions but to feel free to share any comments, concerns, or issues associated with brain donation. The qualitative data collected and transcribed reflect very rich and diverse answers to the interview questions.
Six focus groups were held in 3 different cities: Group A (Philadelphia)—Families here had access to more than 1 FTD caregiver support group and a local clinical research program. Group B (Indianapolis)—Families here did not have access to a formal FTD caregiver support group but did have local access to a clinical research program. Group C (Boston)—Families here had access to an FTD caregiver support group but no clinical research program in the region. A clinical research program was begun in Boston during the study period.
Focus group discussion was guided using a semistructured interview with questions about caregiver experience with medical research, understanding of brain donation and its importance, and effectiveness of communication with researchers (M.G.A. and S.L.J.D. facilitated all focus group discussions).
Data Collection
Each focus group lasted 1.5 to 2 hours and was audiotaped. Recordings were transcribed by a professional transcriptionist. Moderators created an informal atmosphere so that participants felt comfortable sharing both positive and negative perceptions. The co-moderator took notes that reflected the tone and processes of each group, noting characteristics of the groups' conversation (such as participation, signs of emotion, and nonverbal responses).
Data Analysis
A grounded theory design guided data collection and analysis. Grounded theory is an inductive approach, meaning that there is no preconceived theory (eg, about barriers to research participation) that drives data collection, and the theory evolves from the data. 10 Themes emerge from systematic data collection and the observation of the interrelationships of categories of information. 11,12
As an initial step in the analysis, each of the analysis team members, 4 researchers from various disciplines, independently reviewed the focus group transcripts using a whole-text analysis, open-coding method to identify themes around barriers and facilitators of research participation. 13 The codes were developed from the major themes that emerged from the first phase of analysis, along with the original focus group guides. The list of theme-generated codes was compared with the original focus group interview guide and items that were not identified by the themes were added as codes. In the next step of analysis, independent focused coding 14 was carried out by the team and the team members discussed differences in the coding of significant statements until 100% agreement was reached. Where inconsistencies in the coding occurred, the raters came to a consensus on discrepancies. Next, M.G.A. and S.L-J.D. reviewed all coded transcripts to ensure that the final list of codes adequately reflected the data.
Results
Participants
A total of 30 caregivers participated in 6 focus groups. Demographic characteristics of the caregivers were collected from 30 caregivers (13 from Philadelphia, 8 from Boston, and 9 from Indianapolis). The majority of participants were female (24), Caucasian (28), and spouses of the person with FTD (17). Caregivers had been providing care from 6 months to 20 years. Demographic details are presented in Table 1 . The majority of persons with FTD were still living (24) and had been diagnosed on average within the past 5 years with a mean age at diagnosis of 62 (range 47-89). Data on the persons with FTD are presented in Table 2 .
Demographic Characteristics of Caregivers (N = 30)
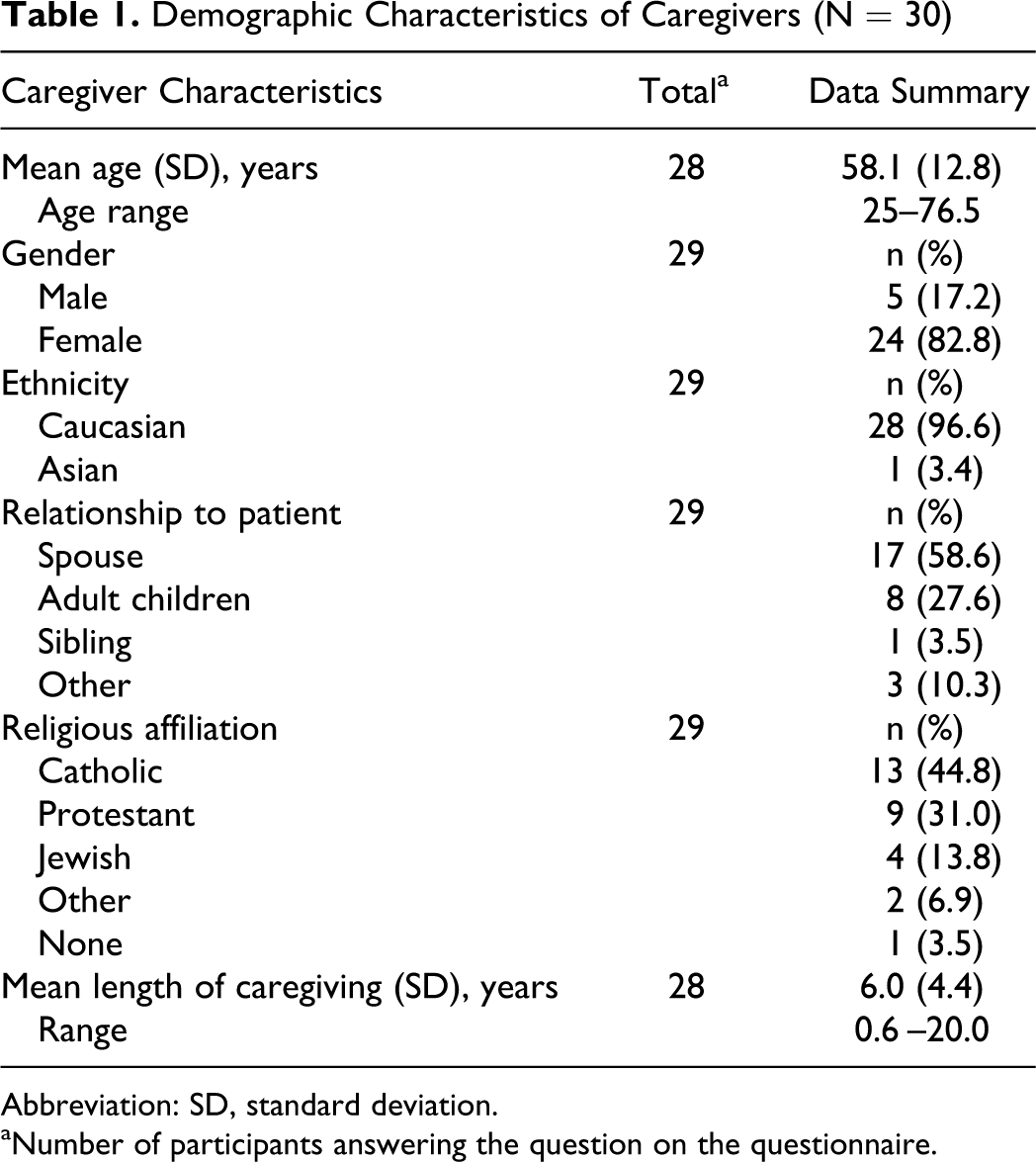
Abbreviation: SD, standard deviation.
aNumber of participants answering the question on the questionnaire.
Demographics Characteristics of Persons With FTD (N = 30)
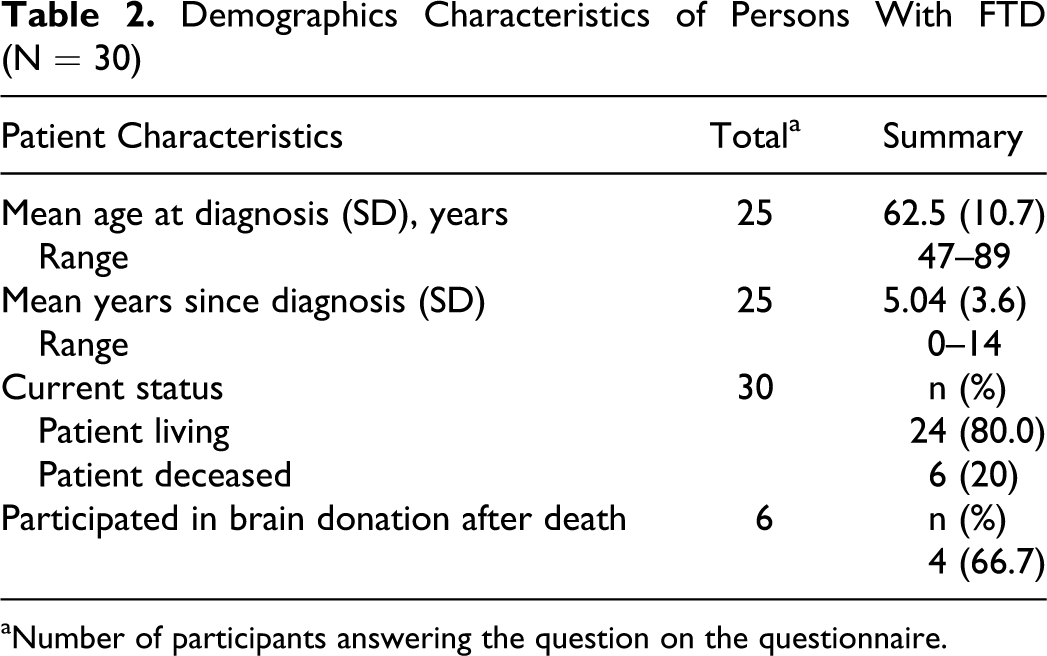
aNumber of participants answering the question on the questionnaire.
Major themes identified from focus groups transcripts
The following 7 prominent themes emerged from the transcripts. Following each theme are direct quotes from caregivers to illustrate the types of responses that were included in each theme.
Interest and willingness to participate in brain donation, but lack of knowledge about opportunities. Caregivers generally want to help with research but have many questions that often do not get answered during their visit to the clinic and/or research center. We want to help but we don’t have enough information. What’s the difference between the brain autopsy and brain donation?
When and how the issue of brain donation is initially raised with the caregiver. Caregivers deemed it inappropriate to raise the issue of brain donation for the first time at the initial clinical meeting or at the end-stage of disease: The first thing that [the physician] said to [my parents] when he walked in was: ‘Have you considered brain donation?’ They were really put off. We were so blown away at the beginning that you could have talked us into selling shoes. After she was wheelchair ridden, the doctor [asked] … if we would like to donate her brain for research. My Dad, to him, it’s just like that’s just a sign of death. You should bring it up … maybe the second [visit] because … by the second appointment I think [the reality of the diagnosis] sets in. Yes, [revisit] it with the caretaker … I just feel like I need a little reminder and a little more explanation.
Who initiates the discussion about brain donation. There did not appear to be consensus on who initiated the discussion about brain donation. Various health care providers (research assistant, neurologist, and physician) initiated the discussion about brain donation; in some instances, it was the family caregiver. The assistant … talked to us about it … Our neurologist definitely talked to us. Actually, I was the one who asked the question. The neurologist didn’t approach me.
Who is involved in the decision about brain donation. Most caregivers were comfortable if the topic was introduced early in the disease course so the patient can make his or her wishes known. Hopefully the person that has been diagnosed will have some input and can say yes, I want my brain to be used for research. When she’s in diminished capacity and can’t respond to him he should have never brought that up. I think if [the patient is] still able to consent and understand it then it definitely should be brought up. If [the patient is] incapable of giving any kind of opinion then it needs to be discussed separately, when they’re not in the room. We talked about it as a family and we decided that this was definitely something we wanted to do. Everybody has got to make the decision. It’s got to be unanimous. In terms of the people I would contact about decision-making it would be a couple of my siblings only and then I would make a decision. [He] does want to go talk to the Rabbi about donating his brain.
The motivation for participating in brain donation. The primary reasons caregivers identified for considering brain donation included getting a definitive diagnosis, being able to provide risk information for family members, and advancing scientific knowledge. It’s really the only way for them to know for sure what the diagnosis is. Because there are so many in the next generation and now even grandchildren coming along that people … want to know [if there are] genetic factors there. So one day, maybe not in my lifetime, but one day a doctor can look at families like us and not say “I don’t know” and not say “I don’t have an answer.”
Lack of communication or details about the brain donation procedure itself; when and what to do as death approaches. One of the caregivers' greatest concerns related to the lack of information regarding the brain donation procedure and the lack of clear instructions on what to do near or at the time of death. I’m unclear about what to do, who to call, what to do at the time of death. What are you physically going to get back? When is the report going to be due? When are you going to be able to get the final diagnosis? And there’s no charge for the family for that, is there? [The brain] doesn’t go back the funeral home? What will happen at [the medical center]? Do you know how long it takes to … get the person’s body back? I just feel like I need some correspondence or some reminders or something, some follow up periodically …. I have too many things on my mind to wonder: Okay, what am I supposed to do? I need it in black and white.
Barriers to research participation. Analysis of the focus group transcripts also revealed a number of underlying issues that may act as barriers to the caregivers' participation in research in general, including brain donation. Examples of these issues included:
Inappropriate and/or unmet expectations around clinical care. Some caregivers described confusion about the lack of follow-up by the clinical team and/or concerns about specific appointments during which they had thought or misunderstood that something was to happen or to be scheduled but did not hear back. Several caregivers were unsure whether they had consented to participate in research or had assumed they consented but had not.
Positions of major religious faiths about organ donation, including brain donation. Some caregivers in this study were unclear about what their religion has to say about brain donation.
Inconsistency among state laws regarding powers of attorney. This issue is particularly problematic when the person with FTD moves to another state for part of the year or might move to live with another family member. Some caregivers were surprised to learn that the expensive legal documents they had worked hard to prepare were not valid in another state.
Discussion
Results from this CPBR focus group study found that family caregivers demonstrated a strong desire to participate in research and contribute to advancing knowledge about FTD, specifically through brain donation. However, our results also showed that there is a significant amount of ineffective communication and misunderstanding around the topic of brain donation between researchers and caregivers. Although all participants in this study indicated genuine interest in brain donation, especially as a means of confirming diagnosis and contributing to improved care for future patients and families, most caregivers demonstrated a significant lack of knowledge about the specific procedures involved in brain donation: for example, what it is, what it entails, where it is conducted, and how it might impact other end-of-life arrangements. Complicating this dearth of knowledge is the fact that these emotionally charged issues must be faced while coping with a neurodegenerative condition for which there is currently neither disease-modifying treatment nor cure. Particularly difficult for patients and caregivers is the fact that FTD has an onset earlier than most other dementias, typically during the prime years of professional and family life. By the time most patients and caregivers find a clinical center with an FTD research program, many of these patients have endured a series of misdiagnoses over a period of several years. Another layer of complexity is added by the fact that established patterns of communications may vary widely among families and are not always easy for the clinician to discern.
Taken within this context, it should not be surprising to note that in all focus groups—but especially the ones conducted in areas where caregivers do not have easy access to a support group—a significant proportion of the discussion was dedicated to the caregivers' sharing their stories, their feelings of isolation, and general frustrations around dealing with this rare disease. In our opinion, the current state of knowledge on FTD (lack of means for definitive clinical diagnosis, lack of approved treatments, and general lack of hope in the immediate term) does much to set the tone of the relationship between the clinician and the family, to some extent undermining the chance for establishing positive trust and rapport. Equally important, however, this study demonstrated that caregivers are interested in learning about brain donation, are open to an honest discussion of the emotionally sensitive issues that it entails, and that such an open discussion does impact the caregiver’s attitude toward research participation. The results further indicated some concrete steps that can be taken to help establish a collaborative, trusting relationship, notwithstanding the lack of diagnostic and therapeutic tools available to the clinician. These may include:
Training clinical research staff
The topic of brain donation raises a variety of issues; some, such as the need for factual information and the emotionally charged, sensitive nature of the topic, are similar for most caregivers. Other issues, such as established communication patterns among family members and professionals, and religious beliefs and practices, will vary widely among caregivers. A compassionate member of the clinical team trained in acknowledging and addressing these issues, who recognizes that families will differ in their comfort level with emotionally charged issues, will have the greatest chance to develop a positive rapport with the caregiver and thus impact not just research participation but the entire clinical care journey, which may last for more than a decade.
Development of educational materials that address the facts about brain donation (where, what, when, how) for family members
These materials can be available not just at the clinic or research center but also through AFTD, a voluntary health organization that can provide caregivers with information when they are ready to receive and process it—factors that may vary widely among individuals.
Provide materials that explain the positions of the major religious faiths about organ donation, including brain donation
Some caregivers in this study were unclear about what their religion has to say about brain donation. Most major religious/faith traditions are supportive of brain donation particularly if done with the intention to further science and help others. 15
Develop a protocol that establishes a standard procedure for when and how the topic of brain donation should be raised with the caregiver
A brain donation protocol should include professional, respectful materials in clear, lay language as well as the opportunity for the caregiver to ask questions. The topic should be revisited by a member of the clinical team throughout the course of the illness. It is worth noting that a clearly proscribed process (the existence of checklists, action steps, and forms) may help to depersonalize some of the more emotionally charged aspects of the discussions and provide the caregiver with some practical tools as well as a broader perspective on the disease experience.
Limitations of the Study
There are some limitations to this study. The lack of minority representation makes it difficult to generalize the results to the general population of persons with FTD and caregivers. Minority groups may have different attitudes about research, brain donation, and cultural and religious issues. Based on research with minority caregivers of persons with AD and brain donation, recent research has shown that while some of the issues about brain donation and research participation are similar to those found in this study (perceptions and misconceptions about brain donation procedures, influence of religion and spirituality, and family perceptions of and involvement in brain donation), significant concerns about racial disparities, discrimination in medical settings, and historical issues about minority participation in research are important among minority participants and cannot be minimized or overlooked. 16 Therefore, minority caregivers of persons with FTD may feel differently than the caregivers who participated in this study. Further study is needed with minority caregivers of persons with FTD. The majority of our caregivers (80%) were female, thus the lack of male caregiver representation makes it difficult to generalize these findings to the general population of persons with FTD and their caregivers. Male caregivers may have different attitudes about research and brain donation. Also, almost 60% of our sample was spouses of persons with FTD, thus making comparisons of attitudes among caregivers with different relationships to the person with FTD difficult.
While the purpose of the focus groups was described in the recruitment materials and at the beginning of each group, participants' emotional/social needs often outweighed the purpose of the focus group in the cities where no formal FTD support groups were available. It became apparent that caregivers of persons with FTD have many unmet social and emotional needs. The need to develop and deliver appropriate supportive interventions to caregivers of persons with FTD was obvious. Had the social and emotional needs of participants not been so great, responses to the questions about brain donation specifically may have been qualitatively different.
Next steps
Based on the results of this study, a larger survey of family members of persons with FTD is necessary to determine whether the themes and issues identified in the focus groups would be consistent in a larger sample and such a study would provide valuable quantitative data associated with the issues raised in this study. Additional next steps include the development of an informative booklet for families on brain donation, to be available at clinical research centers and on the AFTD Web site. The development of training materials for researchers and clinical staff and a standard protocol to guide when and how the issue of brain donation is raised with the person with FTD and their caregiver throughout the course of the illness would be beneficial and is also being planned. Working with the existing research centers and the AFTD to expand the number of FTD caregiver support groups available across the United States is a critical next step. Increased access to emotional support, caregiving skills training, caregiver education, problem solving, and information about local resources may decrease feelings of isolation and help caregivers and families adjust to the diagnosis, prepare for the course of disease, and become more effective, confident caregivers.
Conclusions
Not unlike previous research on brain donation among family caregivers of persons with AD, 17 the family caregivers of persons with FTD participating in this CBPR study demonstrated a strong desire to participate in research, understood that only through a postmortem evaluation would they get a definitive diagnosis and thus potentially better define the risk of first-degree relatives, and wanted to contribute to advancing knowledge about FTD so that some day other families may be spared, specifically through brain donation. However, this study also revealed several specific obstacles to families' participation in brain donation: Caregivers are very interested in participating but have insufficient information on how to do so. Researchers may not be sensitive as to when and how to best approach the subject of brain donation within the framework of the caregivers' experience. Researchers may not have had the opportunity to establish a positive relationship with the family before the subject of brain donation is introduced. Researchers often do not have the opportunity to understand how such a delicate decision should be addressed within the complexity of an individual family’s dynamics. The family’s motivations for participating in brain donation are typically emotionally charged and extremely personal, which complicates the clinician’s task in addressing the issue. The lack of a process that acknowledges that the issue of brain donation needs to be addressed regularly throughout the clinical relationship as the family’s questions and ability to absorb various levels of detail will evolve over time.
The study also identified additional, broader issues that may negatively impact research participation including the lack of clear, effective communication between the clinical team and caregivers which, in turn, creates a significant barrier to the establishment of positive rapport, detrimentally impacting research participation. Our findings are similar to those reported by Stevens who found that “time spent with individuals and their families addressing fears and dispelling common misconceptions appeared to be helpful and offered something in return for their donation” (p. 628). 18 A revised process that is informed by the caregivers' perspective should encourage families to feel ownership in the research process and help decrease barriers to research participation. Of particular note is the motivation for families to understand the risk of FTD and related disorders for future generations, which may be useful for clinicians and researchers to know as they approach a family about brain donation. Although there is no one “right” way to address the sensitive topic of brain donation with every caregiver, this study found some common themes and suggested approaches that can lay the groundwork for a more successful partnership between the clinical researcher and the caregiver/caregivers. We expect these results may be applicable to other neurodegenerative disorders.
Footnotes
Portions of this research were presented in poster format at the 7th International Frontotemporal Dementia Conference, Indianapolis IN, 10-6-8-2010 and the 63rd Annual Meeting of American Academy of Neurology, Honolulu, HI, April 9-16, 2011.
Acknowledgments
We gratefully acknowledge the family caregivers who participated in the focus groups.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed the receipt of the following financial support for the research,authorship,and/or publication of this article: This research was supported by NIH R03NS065489-01 (PI: Guerriero Austrom) and R03NS065490-01 (PI: Dickinson). Drs. Guerriero Austrom, Matthews and Gao were also supported in part by NIH P30AG10133.