
Abstract
The Association for Frontotemporal Degeneration (AFTD) organized a 7-person Task Force on Families With Children to explore the concerns of families when a parent of young children or teens is diagnosed with FTD. This report summarizes the findings of the task force and highlights the need for additional attention to this topic. The task force conducted a review of related literature and existing resources and compiled issues identified by spouses/partners, teens, and adult children within an affected family. The project confirmed a significant lack of information and support for parents caring for a spouse with FTD and for their children. Recommendations include developing resources and strategies that promote comprehensive family support, including those that build resiliency in the well parent and the children, and strengthen the changing family unit. Avenues for additional research in this area of need in the FTD community are suggested.
Keywords
Introduction
Frontotemporal degeneration (FTD) is a disease process that affects the frontal and temporal lobes of the brain. It causes a group of progressive disorders that share many clinical features including changes in behavior, personality, language, and/or movement, and deterioration in a person’s ability to function. Currently, there are no medical treatments and no cure for FTD.
Most reliable estimates indicate approximately 50 000 to 60 000 people in the United States have an FTD disorder. 1,2 Life expectancy averages 8 years from the start of symptoms. Most cases of FTD (50%-70%) are sporadic, which means the risk of occurrence in family members is the same as in the general population. In approximately 10% of the patients with FTD, there is an autosomal-dominant pattern of inheritance where each child or sibling has a 50% chance of inheriting the gene that causes FTD; and in 20% to 40% of cases there is an increased but undetermined risk to family members of developing FTD or another neurodegenerative disorder. 3
Research has shown that the difficulty in obtaining a diagnosis of FTD, the early age of onset, and the presence of behavioral symptoms contribute to greater caregiver burden in FTD compared to Alzheimer’s disease. 4 –6 An increasing number of contacts by young families to The Association for Frontotemporal Degeneration (AFTD) highlight the added challenges faced when a parent is diagnosed with FTD and there are children or teens living at home. Anecdotal reports indicate that their experience is characterized by the stress of helping children understand and cope with the subtle and confusing early symptoms, the often lengthy course to diagnosis, and the demands and isolation of managing a poorly understood, progressive, and ultimately fatal disease.
These contacts and those of colleagues in the field indicate that families are confronted with 3 fundamental tasks when a parent is diagnosed with FTD: (1) to learn about FTD and how to plan and provide care for the affected spouse or partner, (2) to decide how to address the diagnosis and disease with their children, and (3) to help children cope in the midst of the parent’s own grief and often overwhelming stress. Some families must also consider the genetic aspects of the disease and the risk to children of heritability. Families report facing these challenges alone with no specific guidance or assistance. The stress of FTD on younger families—and the opportunity to positively impact their ability to cope—is significant. Information and resources for education, support, and coping are essential to ensure the health of the family and the adjustment and well-being of individual members.
Purpose of the Task Force
From 2003 (my fifth grade year) my mom was becoming a different person . . . I had no idea what was going on and thought that my parents were going to get a divorce because they always seemed to be fighting . . . I later found out this was not the case, my dad was trying to figure out what was going on with mom; he too was confused.—College freshman
The AFTD Task Force on Families With Children was organized in March 2010 to begin to address the challenges of families where a parent is diagnosed with FTD. The group’s mandate was to learn and to lead in the development of resources for families facing FTD who have children at home. Task force membership was multidisciplinary and included professionals and caregivers with relevant expertise: AFTD’s program director, 2 caregivers from the AFTD telephone support group for parents, and professionals from the fields of children’s bereavement, clinical social work/FTD research, family research in dementia and secondary education.
The purpose of the task force was not to conduct an empirical study but to respond to a plea from a growing number of constituents for resources. Task force members endorsed AFTD’s goals for the project which included (1) articulating issues faced by parents and their children and teens, (2) identifying existing resources, (3) prioritizing projects for AFTD to implement, and (4) stimulating additional research and resource development by health care and social service providers. The task force adopted several guiding principles to direct its work:
Bias for action—Efforts were designed to identify projects for AFTD to develop which were consistent with the Association’s mission and would provide direct assistance to parents and their children. Secondarily, the task force sought to share its findings to stimulate the attention of academic research, treatment, and community providers and to create additional resources.
Broad anecdotal input—The approach reflected AFTD’s extensive contact with families and their willingness to share experiences in order to benefit others. The committee utilized a descriptive approach to gather and assess information. It engaged others via multiple channels through AFTD and through the affiliations of other task force members.
Focus on FTD—Because FTD is a rare disease, families often must make do with services that approximate what they need. The impact of a parent losing his or her language ability or displaying disinhibited behavior present unique stresses on each part of the family unit. The task force sought to explore and address the specific and distinct experiences of families facing FTD.
Methods
The task force assessed prior research, existing resources, and needs of families through:
a literature review of studies in burden of care in young-onset dementia, children as caregivers across disability groups, anticipatory grief, parental illness; and bereavement;
an Internet search of support program models for children relating to parental illness, dementia, disability, and bereavement;
anecdotal data on concerns and needs of parents and their children compiled from parents in AFTD’s phone group, FTD caregiver support groups, and the AFTD HelpLine; and
a survey of young adults who were under age 18 and lived at home when a parent was diagnosed with FTD.
Literature Review
A computerized literature search for quantitative and qualitative studies was conducted. The search examined articles from 1997 to 2011 and utilized the following databases, TRIP, CINAHL, psychINFO, Cochrane Collaboration, PubMed, and Google Scholar. The search terms, which aimed to encapsulate broad definitions, were the young carers movement, young-onset dementia, dementia caregiving, parental illness and children, anticipatory grief, and child bereavement when a parent dies. A full review is included in The AFTD Task Force on Families With Children—Report of Findings. 7 Two areas of relevant findings are highlighted here, which show particular potential for additional research and consideration in service development.
Dementia Caregiving and Children
There has been extensive research on family caregiving for persons with dementia. Caring for a person with young-onset dementia can have negative and/or positive outcomes and is a complex process layered upon the contextual issues such as life cycle stage and symptom profile. 8 While the literature on younger onset dementia acknowledges the effects on the family as a whole, very few studies considered the specific impact of a diagnosis on children.
Svanberg, Stott, and Spector 9 systematically reviewed 26 studies on the impact of young-onset dementia on the family. One study described the necessity of a more flexible approach in working with children who are caregivers in order to help them with the unique challenges they face; for example, informing other supportive people (such as teachers) about dementia to help them best support the child. Five studies acknowledged the impact on children, highlighting the psychological and emotional effect on children in the role of caregiver and the exclusion of children from services.
In a separate study, Svanberg, Stott, and Spector 10 conducted semistructured interviews of 12 children of younger persons with dementia, including 3 parents who had FTD. The study aimed to explore the impact of the diagnosis on these children and understand their experiences.
Three stages of adapting to dementia were outlined. First, the child grieves for the loss of the previous parent–child relationship and the relationship they expected to have in the future. Second, the child learns to emotionally detach from the parent and develop a new relationship; that is, the parent is seen as a different person and the child can blame the disease rather than the parent. This allows for a process of “learning to live with it”; and lastly the child begins to act as an equal to the well parent in order to “go through it together,” becoming more autonomous and “responsible.”
Children and Anticipatory Grief
Recent attention in caregiving research has looked at the role of grief and bereavement in dementia caregiving 11 and additional work has begun to explore specifically anticipatory grief and ambiguous loss in dementia caregivers. 12 –15 As Frank15(p517)notes “the incongruence between physical and psychological presence creates high boundary ambiguity in the family system and keeps the caregiver and family in a highly stressful state.” However, to date, the focus of research has been on spouse and adult-child caregivers of people with Alzheimer’s disease.
A search of anticipatory grief and children largely yields research on the death of a child or on adult children of an elderly parent. Similar results occur in searches on parental illness. Again, the literature is largely concerned with adult children.
Research that addresses anticipatory grief in children tends to discuss factors that later affect child bereavement after the parent’s death rather than investigating children’s response to the terminal phase on its own. There is little available on the effects of a parent’s illness on a child or teen during the actual period of the illness and what it is like to “live with” the many stressors associated with an ill parent. The exception to this are earlier studies by Siegel et al finding that children of terminally ill parents had higher levels of stress and anxiety and were less well adjusted than a community sample. 16 It should be noted that these were studies of children of a parent with advanced cancer immediately prior to the parent’s death and not over a long period of time.
An additional exception on the topic of anticipatory grief and children is work by Saldinger, Cain, and Porterfield 17 at the University of Minnesota. The group studied 58 parentally bereaved school-aged children and their surviving parents to explore the challenges they had faced dealing with anticipatory death. The study focused on the child’s exposure to graphic physical, emotional, and mental deterioration of the dying parent. The length of parental illness averaged 2.8 years, with the lengthier illnesses including long periods where the parent was asymptomatic. The authors found 10 potential stressors for children with dying parents including graphic physical deterioration of their parent, frightening mental and emotional images, forced exposure to the dying parent, secondary traumatic stress from not being able to help, and separation anxiety relating to both the patient and the well parent. The authors conclude that parents should err on the side of assuming children will be overwhelmed by exposure to impending death no matter how well informed they are about the expected changes. Further, it is not enough to inform and offer choices to children as many will not understand the implication of choosing exposure to an ill parent. Children still need protection, limits, and reassurance to minimize traumatic stress. 17
In a literature search on the issues of children and bereavement, there is significantly more diversified material. It is widely held that some, but not all parentally bereaved children, will experience mental health problems and that some children are more vulnerable than others. 18 Factors determining a child’s vulnerability include preexisting mental health issues, other stressors, and socioeconomic status as well as the health of the surviving parent. 19 The first longitudinal study on child bereavement using a nonclinical sample was J. William Worden’s Child Bereavement Study. Worden’s book, published in 1996, Children and Grief: When a Parent Dies, presents his findings and makes recommendations for helping children. 20
More recently there are significant contributions from Sandler, Wolchik, and Ayers 21 from the University of Arizona. The researchers frame the bereavement process for children and families as a process of adaptation rather than recovery. They conclude that resilience (adaptability and finding new ways to satisfy needs) is the best outcome for parentally bereaved families. These outcomes are unusual in bereavement literature for their emphasis on positive outcomes rather than pathological reactions to grief. This is particularly hopeful for young children and teens faced with FTD.
Existing Program Models
The task force conducted a scan of the environment to see what services exist that may provide examples or inform the development of models for FTD-specific supports. A search for resources and clinical or support programs for children and teens was conducted via the Internet and through contact with professional colleagues in the United States, Canada, and the United Kingdom. The main search was conducted between June and September 2010. Key words were child(ren), youth/young caregivers, children and illness, bereavement, and dementia.
The concept of “young carers”—children providing care for a parent or grandparent with chronic illness or disability—was first formed in the United Kingdom in the early 1990s and has taken root in Australia and Canada. Barnardo’s Services in the United Kingdom is a program that promotes resilience in children who have suffered adversity. Barnardo’s runs projects across the United Kingdom, which work to support young carers and their families in a variety of ways including offering advice and emotional support, providing opportunities for young carers to take a break from their responsibilities, and helping young carers learn more about their parent’s illness or disability. 22 In 2008, the United Kingdom set out a 10-year plan for young carers called The Carer’s Strategy, which says that by 2018, “children and young people will be protected from inappropriate caring and have the support they need to learn, develop and thrive.” This strategy endorses a “whole family approach”; that is, children’s and adult services must have arrangements in place to ensure that no young person’s life is unnecessarily restricted because they are providing significant care to an adult. The “Whole Family Pathway” was developed in partnership with the Disabled Parents Network and the Princess Royal Trust for Carers and is an online resource for both families and agencies to follow so they can see what choices, responsibilities, and lines of accountability for services may be available. 23
In the United States, the young carers or caregivers movement has been fostered by the American Association of Caregiving Youth, a Florida based nonprofit organization. Their efforts seek to raise awareness of children who provide substantive care for an ill parent and address the need for appropriate support and services for the family. Proponents strive for heightened awareness of children in caregiving roles and to facilitate a coordinated approach to the families’ needs, connecting each family member with services that address their particular concerns. Each of these four countries has a central online source of information for young carers. Some specific resources were found for children of people with mental illness, amyotrophic lateral sclerosis (ALS) and dementia. Most young carers programs and resources are for people with diverse medical and physical disabilities.
Several resources help children understand dementia in a grandparent. Some young-onset Alzheimer's resources address the needs of children with a diagnosed parent. A support group for children and grandchildren of people with dementia or other neurodegenerative diseases was offered for 7 years by the Massachusetts Chapter of the Alzheimer’s Association in the 1990s. An educational video and booklet called “Someone I Love Has Dementia” resulted from the group. The Alzheimer’s Foundation of America offers the AFA Teens Web site (www.afateens.org) to raise awareness of Alzheimer's disease and to engage teenagers in the cause. In late 2011, the Alzheimer’s Association expanded the information available through the pages “Just for Kids and Teens” on their Web site (http://www.alz.org/living_with_alzheimers_just_for_kids_and_teens.asp).
Resources in the United States and Canada relevant for children whose parent is affected by FTD are extremely limited. The ALS Society of Canada offers an educational Web site for children and teens who have a parent with amyotrophic lateral sclerosis (www.als411.ca). Camp Building Bridges is a small 1-week summer camp program for children or grandchildren of people affected by Alzheimer’s or other dementias (http://www.freewebs.com/campbuildingbridges08). Started in 2008 by a woman diagnosed with FTD, the program is now offered through the Oklahoma/Arkansas Chapter of the Alzheimer’s Association. In late 2011, the Canadian Dementia Knowledge Transitions Network launched a Web site for teens and parents affected by young-onset dementia or FTD: “When Dementia is in the House” (http://www.lifeandminds.ca/whendementiaisinthehouse).
Assistance programs for grieving families with young children tend to be support group models utilizing professional staff with trained volunteers. These include programs in hospital and hospice settings, church-run support groups, free-standing grief centers, and schools. The Family Bereavement Program (FBP) is an intervention developed by Sandler et al, at Arizona state. The program is currently evaluating the efficacy of a psychoeducation-based intervention for youth who have lost a parent and their surviving parent/caregiver over a 6-year period. The program has shown promising results including reduced levels of problematic grief, improved self-esteem, and a higher quality of caregiver–youth relationships. 21
For children who are bereaved there are also camps such as Camp Comfort Zone, a weekend camp that operates in California, Massachusetts, New Jersey, and Virginia. Camp Erin is a nationwide network of bereavement camps in the United States for children and teens aged 6 to 17 who have experienced the death of a loved one. There are smaller, localized camp programs at hospices around the country as well.
Input From Families
The task force employed several methods to explore the support and education needs of families with children. It compiled a descriptive understanding of the needs of the well parent and children through the resources of AFTD and task force members. The goal was to provide a broad understanding of the need to guide AFTD and to stimulate further academic research in the field. The task force obtained anecdotal input in several ways:
First-person experiences with spouses or partners of a person diagnosed with FTD who have children at home as reported to task force members. The input reflected contact with AFTD’s HelpLine, medical center clinic patients, family research study participants, FTD support group facilitators, and AFTD’s parents’ phone support group members. Task force discussions took place over 4 monthly meetings and were documented.
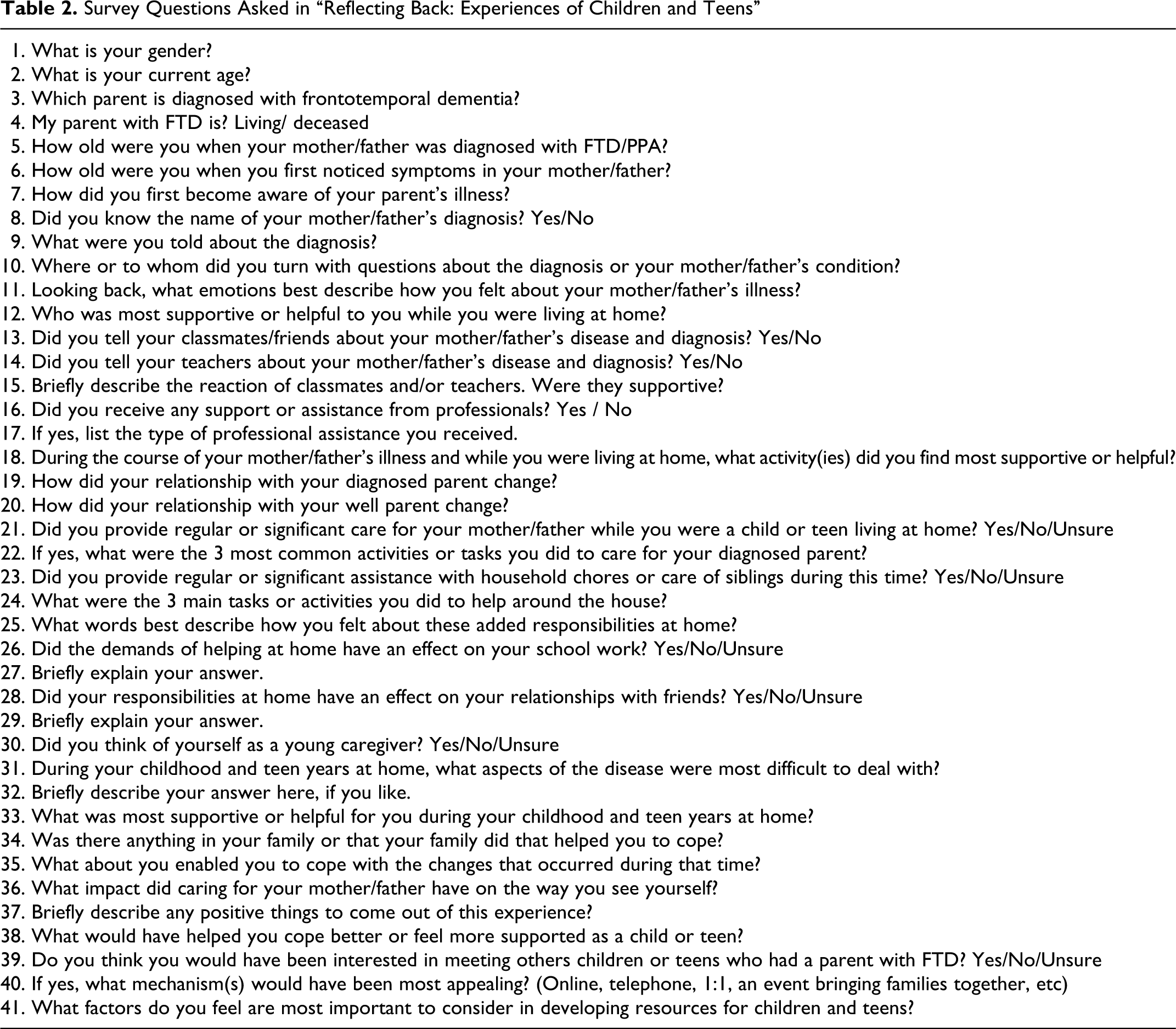
A survey of young adults who were under 18 and living at home at the time a parent developed FTD. “Reflecting Back: Experiences of Children and Teens,” was a 41-question survey that elicited information about their experiences and the impact of their parent’s illness. It asked about their understanding of the disease, emotional support, caregiving activities, coping, and suggestions for others. The survey was available online for 3 weeks in September 2010. It was posted on AFTD’s Web site, forwarded to FTD support group leaders and shared through task force members. Responses were anonymous and were compiled and reviewed by the task force to identify themes.
Participants in AFTD’s parent phone support group (N = 10) invited input from their children in 3 areas of interest to the task force: their desire to interact with other children/teens, the most beneficial activities to help cope with the disease, and their most difficult challenges.
Results
Concerns of Parents and Children
Why does Daddy fight us over the remote? Why does he take my things without asking? Why it is OK for him to do things you tell us are not polite? What do I tell people? He doesn’t look sick so do people think he’s just weird? The kids have so many questions and only me to answer them.—Parent in AFTD phone group.
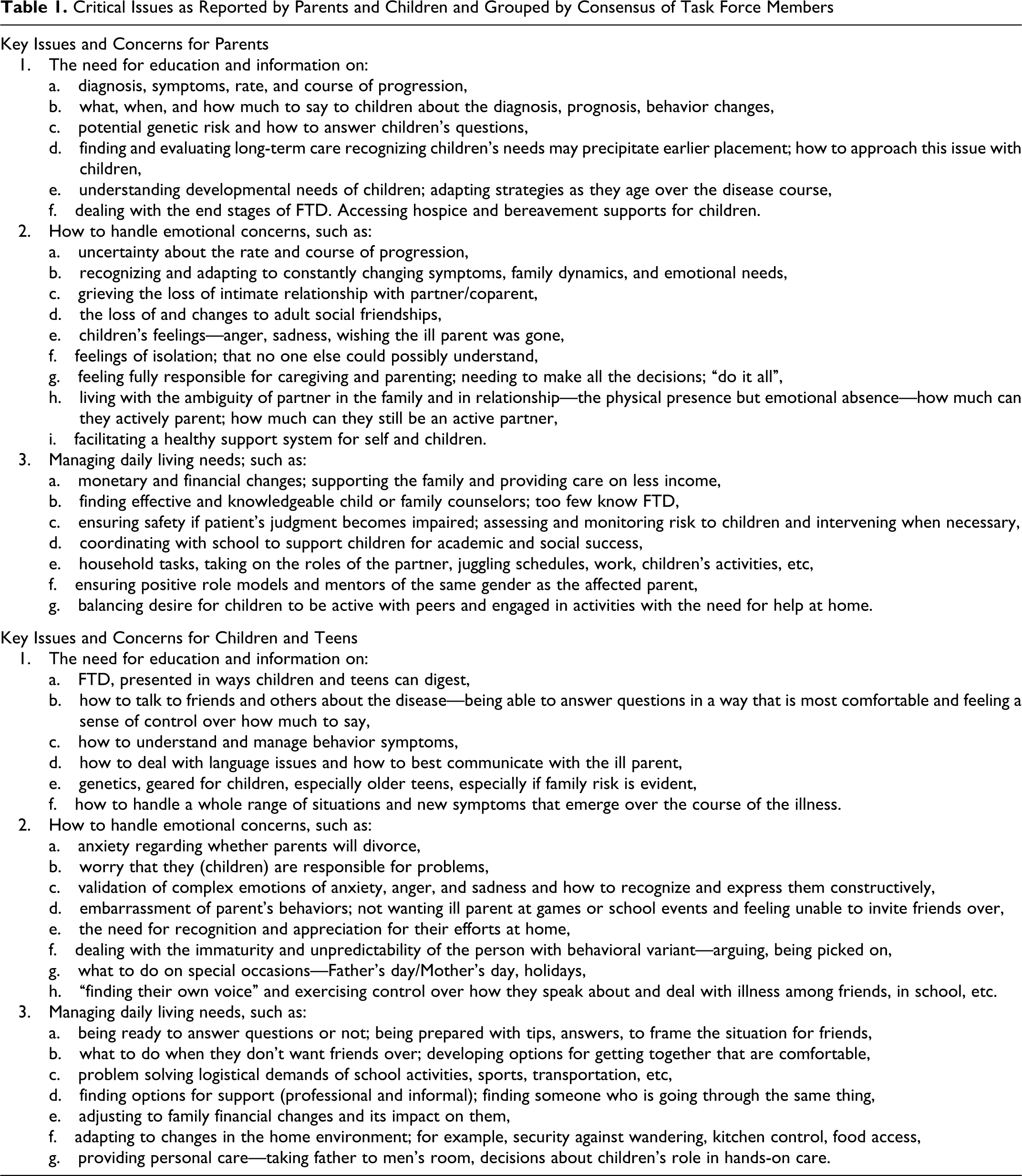
Two lists were generated by the task force, one reflecting key issues and concerns of parents and one reflecting concerns of children/teens. They were generated through discussion by task force members over 4 months and tested with the parent support group. The lists were grouped into 3 areas: the need for education/ information, managing daily living needs. These categories were established by consensus of task force members to reflect potential points of intervention (Table 1).
Critical Issues as Reported by Parents and Children and Grouped by Consensus of Task Force Members
Survey of Young Adults
Additional input was obtained from 24 young adults who reported being less than 18 years old at the time a parent developed FTD. They completed the Reflecting Back online survey over a 3-week period in September 2010. A majority of the respondents were female (70.8% [17] to 29.2% [7] male) and between 18 and 25 years old (54.5%; range 18 to over 35). The diagnosed parent was the father in 56.5% (13) of cases, mother in 34.8% (8), stepfather in 4.2% (1), and stepmother in 4.2% (1); 65.2% (15) were 16 to 18 years old when the parent was diagnosed with FTD and another 21.7% (5) were 13 to 15 years old.
Questions were open ended and asked about illness education (how and what they learned about their parent’s diagnosis), emotional support, caregiving activities, coping skills, and suggestions for others (Table 2). Roughly half the people answering, 47.6% (10), indicated they had been told the name of their parent’s diagnosis; 52.4% (11) had not. When asked “Where or to whom did you turn with questions about the diagnosis or your mother/father’s condition?” the answers given most frequently among 21 responses included the well parent (23.8%, 5 responses), the parent and Internet (23.8%, 5 responses), and the Internet alone (19.0%, 4 responses). Five people (23.8%) responded they had no one to turn to or did not want to talk about it.
Survey Questions Asked in “Reflecting Back: Experiences of Children and Teens”
People were asked what emotions best describe how they felt about their parent’s diagnosis. They could enter responses into as many as 5 text fields. Eighteen people responded; of them “sad” (12), “angry” (11), “scared” (6), and “confused” (6) were the most frequent answers. The majority of those responding indicated the well parent and family, especially siblings were the most supportive people to them. The activities people found to be most supportive while at home during a parent’s illness included being with friends, participating in sports and physical exercise, listening to music, staying busy, escaping into video games, and staying away from the house. This sample was evenly split between those who told their classmates and friends about their parent's diagnosis (47.4% [9]) and those who did not (52.6% [10]).
Survey participants also considered how their role and activities at home changed as a result of a parent’s illness with FTD. Of the 19 respondents, 57.9% (11) provided regular or significant care for the parent while they were a child or teen living at home; 26.3% (5) did not; and 15.8% (3) were unsure. The most commonly mentioned types of care included companionship, entertainment, and driving for errands. Five of those who answered indicated they helped their parent with significant personal care tasks, such as toileting, bathing, eating, and maintaining a feeding tube. When asked to describe how they felt about additional responsibilities at home, respondents said they felt “stressed,” “annoyed,” “angry,” “like it was [their] duty,” and that it was “unfair.” Some however, responded differently, indicating they felt “responsible,” “helpful,” “caring,” “happy,” and “more grown up.”
Participants were asked what aspects of the disease were the most difficult for them. They could enter up to 3 text responses with brief explanations of those responses. Answers fell into several categories (1) behavior symptoms, (2) loss of established relationship, (3) cognitive and communication symptoms, and (4) caregiving responsibilities. Among the most frequently mentioned was dealing with behaviors seen as intrusive, embarrassing, or inconsistent with the parent role. Examples of individual comments include:
Not listening when we tell him something like go watch TV and he says ok, but doesn’t move. Plus he is constantly making some type of noise that gets annoying.
Erratic behavior. Getting lost while walking home or saying inappropriate things in public. Having locks on the inside of doors so she wouldn’t escape was an adjustment. She was like an infant and that was very weird for me to see.
Hoarding, shop-lifting, never knowing what to expect. Poor hygiene. All the changes without understanding the underlying cause led to a lot of social embarrassment.
Aggression. She never hit us, but . . . it was just scary and unsettling because we did not know if she was going to get abusive or just yell at us.
The first thing she lost was her voice. It was hard not to ever hear her speak again.
Apathy. Knowing I no longer had an involved mother.
Watching him struggle at things he once did without fail.
Additional areas of difficulty mentioned included handling the parent moving out of the home to a care facility, dealing with the well parent’s emotions, and fear of what happens if the well parent gets sick.
Thirteen people answered the question “What impact did caring for your mother/father have on the way you see yourself?” Common responses included appreciating and fostering the closeness of family relationships, and growth in strength and confidence to handle life’s challenges. “It made me grow up a lot faster than a young adult is supposed to. It made me strong. It taught me how to take care of family.”
I am very patient and I am great at explaining things to people. I am appreciative of things in my life and often aware (more than others) that nothing lasts forever.
It helped me mature and take on responsibility.
It made me realize that you can’t waste any time in your life. Life is so short. I do not worry about the small things, I never have.
It is everything and every part of me. It is how I decide if someone is going to be there and be a friend or if they will be an acquaintance. . . . Also, I know that if I can get through losing my mother, I can get through anything.
One person expressed tension from divided loyalties.
I see myself as more selfish because when I’m with my friends, I feel guilty like I should be spending this time with my Dad. I might be missing out on opportunities I could have now with him and not later.
Of the 14 people, 3 responding to the question “Briefly describe any positive things to come out of the experience” commented that they could find none.
No nothing really.
I wish I could say it made me stronger, but I am fearful of what the future holds with regard to my mother’s health, my own health, financial ruin, etc.
I don’t know if there are any positives, because now my sister is affected by the same sickness.
In terms of suggestions for coping and support, 72.2% (13) of respondents said they would have been interested in meeting other children or teens who had a parent with FTD; 11.1% (2) said they would not; and 16.7% (3) were unsure. When asked what mechanism/mechanisms would have been most appealing (online, telephone, one-on-one, an event bringing families together, etc), 61.5% (8) people listed an in-person family event first, followed by phone or support groups; 38.5% (5) people mentioned online supports first, followed by group events or support groups for children/teens. A full exploration of the survey responses is available in the AFTD Task Force Report of Findings available on AFTD’s Web site www.theaftd.org.
The task force did not plan to solicit input directly from children or conduct outreach to minors. Because parents in AFTD’s phone support group wanted to invite their children to provide informal input to the task force, a brief 3-question survey was developed. Children were asked about (1) their desire to interact with other children/teens who have a parent with FTD, (2) the most beneficial activities to help cope with the disease, and (3) their most difficult challenges.
Responses were received from 12 children in 4 families. They were compiled by the parent and forwarded to the task force through the support group. Five (41.7%) said they wanted to talk to others about their situation but did not know the best way to arrange that. Social networking and online resources are common tools today, but many in this sample did not think that connecting via a social network, such as Facebook, would appeal to them. They said their most effective coping and support came through involvement with friends, activities, sports, and professional therapists. The most difficult aspects included dealing with changing behaviors, such as when they think the affected parent is lying or acting more like a child than adult. Also mentioned were the challenge of the parent moving to a care facility, dealing with the well parent’s emotions, and fear of what happens if the well parent gets sick.
Discussion
I needed my well-parent to be seeking better emotional support. I also needed emotional support and would have benefited from knowing other kids who were experiencing similar family stresses, and having others whom I could relate to. Even having an adult who knew about the disease to talk with would have been helpful. —Young adult in her teen years
The task force literature review and search for programs and services confirmed that extremely limited attention has been paid to the specific needs of families with a parent diagnosed with FTD who have children at home. Anecdotal input highlights the combined stress on a family from the lack of awareness of FTD, characteristic behavior and language symptoms, and increased care management and financial burden. The constantly changing symptoms and needs are also noted as particularly challenging for a young family. The patient’s needs grow as the disease affects more areas of functioning. Simultaneously, children grow, develop, and must navigate their own milestones. Siblings within a family are at different developmental and emotional stages, and each person understands the disease and processes loss differently as they grow. The well parent is left to juggle these shifting sands, attempting to provide physical and emotional support for all.
The presence of behavior symptoms and loss of the parent–child relationship are defining aspects of the experience for many FTD families. Erratic or inappropriate social behavior in a parent is frequently cited as a source of embarrassment and social isolation for children and teens. In the survey, young adults most often described feeling sad, angry, scared, and confused by their parent’s illness. Roughly half of those responding told friends and classmates about the parent’s diagnosis. Fewer told their teachers (31.6%, 6 respondents) compared to 68.4% (13) who did not. Only 22.2% (4) of this sample received support from a social worker, psychologist, or other professional. Young adults noted the well parent and other family as their primary source of support. Parents, in turn, report feeling that they face FTD alone and are poorly equipped to guide their children.
In order to assist their children effectively, the well parent needs particular resources and support. Reliable information on FTD is increasingly available; however, guidance on developmentally appropriate approaches to talking with children about FTD, understanding how children approach and process grief, and practical suggestions for daily coping and communication with other people in a child’s life—teachers, friends, friends’ parents—are lacking. Parents struggle to understand the genetics of FTD, which makes the prospect of children asking about heritability very stressful. People regularly report the positive value of the emotional and problem-solving support found with other FTD caregivers; the desire for access to peer support by people with children and teens is significant.
Svanberg 10 posit a process of children adapting to young-onset dementia in a parent that involves grieving the previous parent–child relationship, emotionally detaching from the ill parent and joining the well parent in order to contend with caregiving. This led some children to feel more autonomous and capable. Young adults were asked in the task force survey, “What impact did caring for your mother/father have on the way you see yourself?” Responses included appreciation and development of the closeness of family relationships and growth in strength and confidence to handle life’s challenges.
The importance of helping children manage their grief resonated with caregivers on the task force. Sandler, Wolchik, and Ayers 21 studied the management of grief as a process of adaptation that recognizes both risk and protective factors within an individual and his or her environment. The overall outcome is shaped by the cumulative effect of individual and environmental risk and protective factors, rather than any single one. In FTD, the well parent and children may rely extensively on each other for assistance. Understanding the individual strengths and vulnerabilities of each family member and for the environment as a whole may inform an approach to services that would strengthen individuals and the changing family unit.
Each individual will experience grief through his or her own lens, which includes looking at how his or her environment and relationships change. Supporting each member of the family within the context of the entire unit is critical, especially given the prolonged and changing nature of FTD progression. Supports must address a range of needs, from providing accurate, age-appropriate disease information and promoting positive emotional relationships to assisting with practical daily management and successful engagement in school and work. Families with children tend to consider assisted living and long-term care facilities earlier than those without. Efforts must focus on assisting the entire family system to adapt and build resilience over time.
[At the time of my mother’s diagnosis] I had no idea the impact this event would have on my life or how long it may last. I was scared and worried . . . I had no idea what to do or how to handle the situation. I worried that my family was going to fall apart, my parents would divorce and that I would be separated from my brother. Well what happened . . . was the exact opposite. So many wonderful people in my life . . . stepped up and offered support and encouragement.
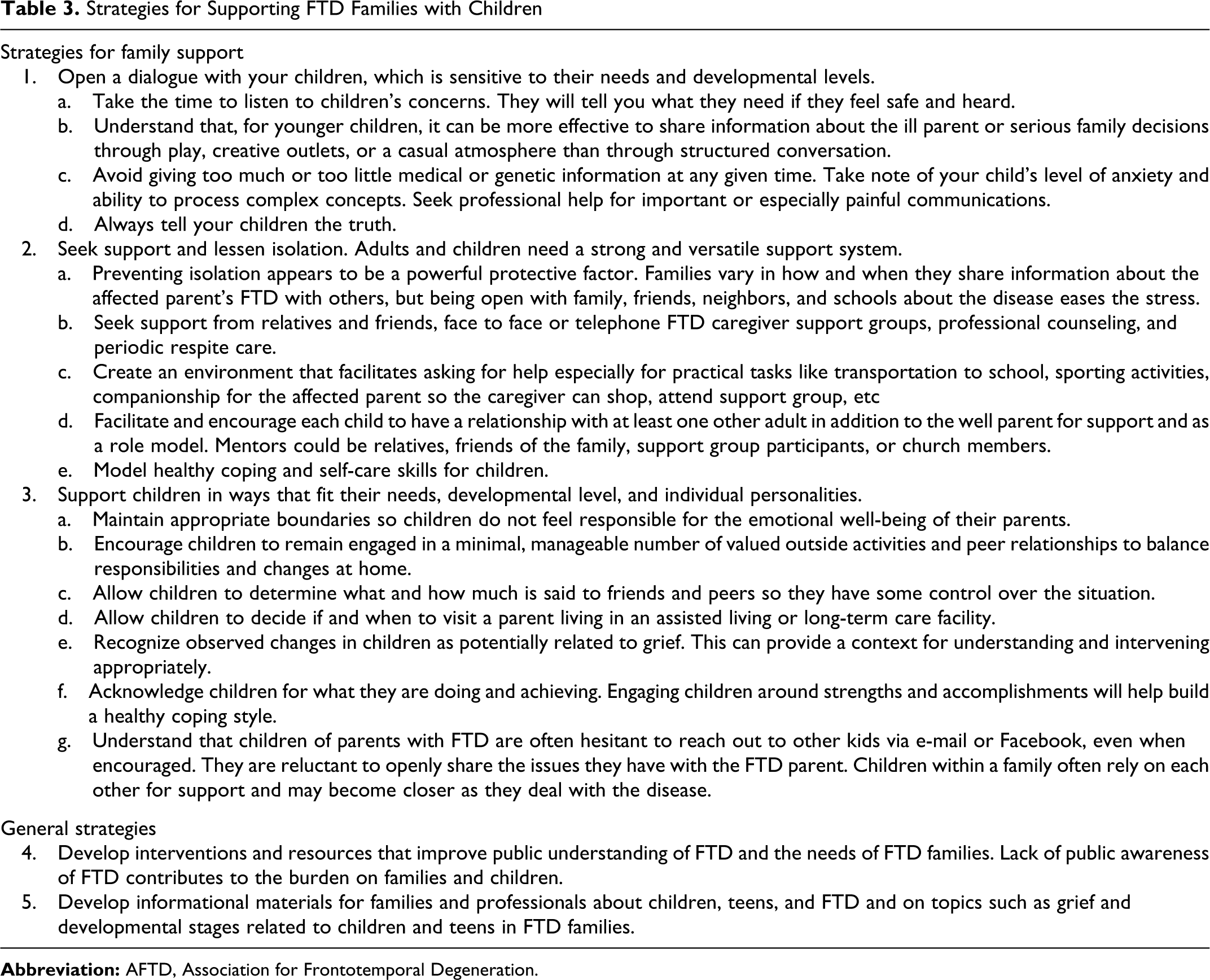
A compilation of the input gathered from all contributors to the task force resulted in endorsement of the strategies for supporting FTD families with children (Table 3).
Strategies for Supporting FTD Families with Children
Limitations
This work is based on communication with extensive numbers of people affected by FTD, professional observation, and broad surveys of published research in related disciplines and programs for caregiving children around the world. We utilized the capacity of AFTD as advocates within the FTD community. The objective of the task force was to identify the initial and fundamental resources needed and to stimulate further attention to this portion of the FTD community among academic, medical, and community providers. The information may be influenced by a self-selection bias as input was received from individuals who engaged with professionals, AFTD, or other FTD families. Further study is needed to develop and evaluate specific interventions.
Conclusions and Future Directions
The need for improved information and support for both parents and children in families affected by FTD is demonstrated. Principal concerns of the well parent and children include dealing with changing family structures and relationships, helping children find their own way to speak about their grief and loss, and answering questions about genetics. Areas warranting further exploration include the experience of grief, bereavement and coping over the progression of FTD, a better understanding of specific risk and protective factors in FTD families, and the design and establishment of a framework for holistic services and supports to affected families.
As a result of the work of the task force, AFTD published a brochure for parents, “What About the Kids—Frontotemporal Degeneration: Information for Parents with Young Children and Teens,” available on http://www.theaftd.org. A Web site designed for children and teens is in development. With effective supports, both parents and children will be better equipped to cope with the demands of having a parent with FTD.
Footnotes
Acknowledgements
The authors would like to thank the members of the AFTD Parents Support Group and facilitator Catherine Pace-Savitsky for inspiring this project and for their generous assistance throughout. They would also like to thank the young adults who responded to the “Reflecting Back” survey and all the caregivers and family members who experience and insight.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.