
Abstract
Aims:
Nuclear receptor binding protein 2 is ubiquitously expressed in all tissues in humans. However, few studies have reported the function of nuclear receptor binding protein 2 in human cancers.
Methods:
Immunohistochemistry and Reverse Transcription-PCR (RT-PCR) were used to detect nuclear receptor binding protein 2 expression in intrahepatic cholangiocarcinoma tissues. Cell Counting Kit-8 assay, flow cytometry, Transwell assay, wound healing assay, and Western blotting were used for the functional study of nuclear receptor binding protein 2. All statistical analyses were performed using SPSS 19.0.
Results:
Survival analysis showed that high expression of nuclear receptor binding protein 2 led to better prognosis. Overexpressed nuclear receptor binding protein 2 can inhibit the proliferation rate of cholangiocarcinoma cells while having a slight effect on cell apoptosis. Gain-of-function experiments showed that overexpressed nuclear receptor binding protein 2 could lead to G1 phase arrest in RBE and CCLP cell lines. Furthermore, Transwell assay showed that overexpressed nuclear receptor binding protein 2 could inhibit the migration ability of RBE and CCLP cell lines. Western blot analysis showed that E-cadherin was upregulated, while N-cadherin and vimentin were downregulated. In addition, we observed that overexpressed nuclear receptor binding protein 2 can also increase the cisplatin sensitivity of cholangiocarcinoma cells by regulating the Mammalian Target of Rapamycin (mTOR) pathway.
Conclusions:
Our study observed that nuclear receptor binding protein 2 played a tumor suppressive role in intrahepatic cholangiocarcinoma, which may be attributable to the induction of G1 phase arrest and inhibition of progression of epithelial–mesenchymal transition, and overexpression of nuclear receptor binding protein 2 leads to improved efficiency of cisplatin treatment.
Keywords
Introduction
Human cholangiocarcinoma (CCA) is a highly malignant, generally fatal neoplasm and primarily occurs in Chile, South Korea, and Northeast Thailand, while a rare cancer (incidence of less than 6 cases per 100 000) in Western countries. 1 Although we have several methods for CCA diagnosis, including imaging studies, cytology and/or histology, and serum tumor markers, patients diagnosed in the advanced stage have few options for surgery. 2 Furthermore, those patients who are eligible for radical operations only survive 1 to 3 years. 3 Therefore, it is necessary to understand the molecular mechanism underlying tumor progression, by which tumor cells gain the properties of proliferation, drug resistance, invasiveness, and metastasis.
Nuclear receptor binding protein 2 (NRBP2) is a gene with unknown function that shows 59% amino acid similarity to the putative adaptor protein, nuclear receptor binding protein 1 (NRBP1). 4,5 A recent study revealed that NRBP2 was associated with neuronal differentiation and affects neuronal cell survival. 6 Zhang and his colleagues determined that NRBP2 overexpression can enhance sorafenib sensitivity of the hepatocellular carcinoma (HCC) cell line by inhibiting annexin A2 (ANXA2) expression and activity of the AKT/PKB (Protein Kinase B) signaling pathway. 7 However, the function of NRBP2 in CCA is unclear, especially in intrahepatic cholangiocarcinoma (ICC). In this study, we aimed to preliminarily analyze the role of NRBP2 in CCA cells and the relationship between the expression of NRBP2 and the prognosis of patients with ICC.
Materials and Methods
Patients and Cancer Tissue Sample Collection
Samples were obtained from 29 patients with ICC who underwent surgery at the Second Affiliated Hospital of Xi’an Jiaotong University. All patients were diagnosed with ICC in our hospital and accepted surgery without radiation and chemotherapy. The R0 (resection margin negative) was used as a standard of successful operation. All patients accepted adjuvant therapy with gemcitabine and cisplatin after the operation. Fresh cancer tissues and adjacent matched normal tissues were collected and a part of them was stored at −80°C immediately after resection, and the other was fixed in formalin for paraffin blocks. Two pathologists examined the cancer tissues and the matched normal tissues. The medical ethics committee of the Second Affiliated Hospital of Xi’an Jiaotong University approved the protocol, and written informed consent was obtained from all participants. Next, clinicopathological features were collected, including age, gender, size of tumor, number of tumors, vessel invasion, and tumor grade.
Follow-Up
All of the patients were regularly examined every 3 months after the operation during the follow-up period. All of the patients were followed during a period of time (from May 1, 2012, to July 31, 2015). Overall survival was calculated in months from diagnosis until the date of death, last time known to be alive, or date of study closing. The median follow-up time in this study was 32.5 months (range: 5-60 months).
Cell Culture
Cholangiocarcinoma cell lines, RBE and CCLP, were purchased from the Chinese Academy of Science Cell Bank (Shanghai, China). RBE and CCLP cells were maintained in RPMI 1640 (Royal Park Memorial Institute 1640) and supplemented with 10% FBS (Fetal Bovine Serum) at 37°C in a humidified atmosphere of 5% CO2.
Construction of NRBP2 Overexpression and mTOR Suppression in CCA Cell Line
To generate NRBP2 overexpression in RBE and CCLP cell lines, NRBP2 complementary DNA clone was purchased from Origene (Rockville, USA) (Cat No SC310591), and we constructed the transient overexpression of NRBP2 in RBE and CCLP cell lines according to the product manual. The efficiency of transfection was verified by Western blot analysis. Human-specific Mammalian Target of Rapamycin (mTOR) siRNA small interfering RNA (siRNA) was designed, constructed, and purified by Jima Biotech Co (Shanghai, China). siRNA targeting mTOR was constructed with the following annealed duplex: mTOR siRNA, 5′-GAACTCGCTGATCCAGATG-3′ and control siRNA, 5′-TTCTCCGAACGTGTCACGT-3′. The transfection was conducted using Lipofectamine 2000 (Invitrogen Co, Carlsbad, CA, USA), according to the manufacturer’s instructions.
Immunohistochemistry
The paraffin slides were deparaffinized and placed in a solution of absolute methanol and 0.3% hydrogen peroxide for 30 minutes. Next, antigen retrieval was performed by heating the slides in citrate buffer (pH 6.2) in the microwave oven for 20 minutes and washed in PBS (phosphate buffer saline) 3 times before staining with immunoperoxidase. Slides were incubated in a humidified chamber with blocking agent (5% FBS) for 60 minutes at room temperature. Next, slides were incubated overnight with anti-NRBP2 antibody (ab172866; 1:100 dilution; Abcam Biotechnology, Cambridge, United Kingdom) in 5% FBS overnight at 4°C. After PBS wash, they were incubated with horseradish peroxidase–conjugated goat anti-rabbit immunoglobulin for 40 minutes at room temperature. The results were visualized by reaction with diaminobenzidine (3,30-diaminobenzidine tetrahydrochloride) and counterstained with hematoxylin. For each sample, we imaged with a high-power objective (20×) under the same conditions. Next, the tissues were scored according to the intensity of the dye color and the number of positive cells. The intensity of the dye color was graded as 0 (no color), 1 (light yellow), 2 (light brown), or 3 (brown), and the number of positive cells was graded as 0 (<10%), 1 (10%-30%), 2 (31%-50%), 3 (51%-75%), or 4 (>75%). The 2 grades were multiplied together. Next, we assigned the score to 2 levels: <6 was low expression and ≥6 was high expression.
Total RNA Extraction and RT-PCR
A TRIzol total RNA extraction kit (Invitrogen Co, Carlsbad, CA, USA) was used for total RNA extraction from ICC patient tissues. Complementary DNA was synthesized using RETROscript reverse transcription kit (Invitrogen Co, Carlsbad, CA, USA). For quantitative real-time Reverse Transcription-PCR (RT-PCR) analysis, the Roche LightCycler (Basel, Switzerland) was used with Takara SYBR Premix Ex Taq system (Tokyo, Japan). All procedures were performed following the instructions from the kits. Primers were synthesized by Shanghai Sangon Biological Engineering Technology Services Co, Ltd, China. The nucleotide sequences of the primers were as follows: GAPDH, 5′-ATGGGGAAGGTGAAGGTCG-3′ and 5′-GGGGTCATTGATGGCAACAATA-3; NRBP2, 5′-AAGACCAAGAAGAACCACAAGG-3′ and 5′-CTGAATGAAGATGGTGTCGCT-3′. Each sample was performed in triplicate. GAPDH (glyceraldehyde-3-phosphate dehydrogenase) was used as an internal reference, and the 2−ΔΔCT method was used to analyze PCR results.
Western Blot Analysis
Western blot analysis was based on RBE and CCLP cell lysis. Total proteins were extracted from harvested cells by a protein extract kit (Beyontime, Jiangsu, China). All proteins were denatured by boiling, separated by SDS-PAGE (Sodium dodecyl sulfate-polyacrylamide gel electrophoresis), and transferred onto PVDF (Polyvinylidene Fluoride) membranes. Then, membranes were blocked with 5% milk. Next, the membranes were incubated with the primary antibodies overnight at 4°C. After that step, membranes were washed 3 times with TBST (Tris buffered saline with Tween-20) and incubated with the secondary antibody (goat anti-rabbit) for 2 hours in the 37°C incubator. Finally, membranes were visualized by a chemiluminescence kit (Beyontime) on a Bio-Rad (Hercules, CA, USA) imaging system. Primary antibodies used in this study are as follows: NRBP2 (ab172866; 1:1000 dilution; Abcam Biotechnology), anti-caspase3, and anti-cle-caspase3 (1:1000; Cell Signaling Technology Inc, Danvers, Massachusetts); E-cadherin, N-cadherin, and vimentin (1:1000 dilution [epithelial–mesenchymal transition, EMT] Antibody Sampler Kit #9782; Cell Signaling Technology); MMP2 (matrix metalloproteinase-2) and β-catenin (1:1000; Proteintech, Chicago, USA), CDK2 (Cyclin-dependent kinase 2), CDK4 (Cyclin-dependent kinase 4), CDK6 (Cyclin-dependent kinase 6), CyclinA2, and CyclinD (1:1000; Abcam Biotechnology); mTOR (1:400; Cell Signaling, Natick, Massachusetts); p-mTOR (2481 and 2448, 1:1000; Cell Signaling, Natick, Massachusetts); and GAPDH and β-actin (1:1000 dilution; Abcam Biotechnology).
Cell Viability Assays
To detect relative cell viability, RBE and CCLP cells transfected with the NRBP2 overexpression plasmid or control plasmid were seeded into 96-well microplates at a density of 5000 cells per well with or without the treatment of cisplatin. Next, the Cell Counting Kit-8 (CCK-8) assay (Dojindo, Kumamoto, Japan) was performed according to the manufacturer’s instructions at 24, 48, and 72 hours. Briefly, 10 μL of CCK-8 working solution per 100 μL of medium was added into the microplates, and the cells were incubated for 2 hours. The OD (optical density) 450 value was determined using an MRX II microplate reader (Dynex, Chantilly, Virginia).
Cell Cycle and Apoptosis Analysis
Both RBE and CCLP cells transfected with the NRBP2 overexpression plasmid or control plasmid were trypsinized and washed 3 times with prechilled PBS buffer and resuspended in 100 μL PBS at 1 × 106 cells/mL after 48 hours of transfection. For cell cycle analysis, samples of cells were fixed in 75% ethanol overnight, and DNA was stained for cell cycle analysis. DNA was stained and RNA was removed by DNA Prep Stain containing RNase (Coulter DNA-Prep Reagents kit; Beckman Coulter (CA, USA)) in the dark at room temperature for 30 minutes. The DNA content of stained cells was measured with BD LSR II (BD Biosciences, Bedford, Massachusetts). Each histogram was constructed with data from at least 10 000 events. The percentage of a cell population in each phase from the experimental data was calculated using ModFit LT 3.2 software. Apoptosis was measured with FITC (fluorescein isothiocyanate)-conjugated Annexin-V and a PI (propidium iodide) kit according to the manufacturer’s instructions and was analyzed with the same flow cytometer and FlowJo 7.6 software.
Cell Migration Assay
Migration assays were performed using Transwell plates (Corning, New York). After 48 hours of transfection, RBE and CCLP cells transfected with the NRBP2 overexpression plasmid or control plasmid were trypsinized and collected. Next, 1 × 105 cells were cultured in serum-free RPMI 1640 on an insert coated without Matrigel (migration assay; BD Biosciences) for 24 hours. In the lower compartment, medium was changed with RPMI 1640 complete medium. After fixation and staining, cells on the bottom surface that invaded across the membranes were counted and imaged. All experiments were performed in triplicate.
Statistical Analysis
Data are presented as the means (standard deviation). For comparisons, Student t test, paired samples t test, and Fisher exact test were performed as appropriate. Cumulative recurrence and survival probabilities were evaluated using the Kaplan-Meier method, and differences were assessed using the log-rank test. Univariate and multiple variable analyses were conducted by Cox regression. All analyses were performed with SPSS 18.0 software (SPSS Inc, Chicago, Illinois). Differences were considered to be significant at P < .05.
Results
Nuclear Receptor Binding Protein 2 Was Downregulated in Human ICC Tissues
To investigate the function of NRBP2 in the progression of ICC, the NRBP2 expression level was detected by immunohistochemistry (IHC) in 29 paired ICC tissues and adjacent neighbor tissues. The results showed that NRBP2 was primarily located in the cytoplasm and downregulated in ICC tissues, and 24 paired ICC tissues had lower expression than adjacent noncancer tissues. Only one paired was upregulated, while the others had no change (Figure 1A, B). Next, we used RT-PCR to detect the messenger RNA (mRNA) level of NRBP2 in another 24 paired ICC tissues and adjacent neighbor tissues, and the results were consistent with the IHC results (Figure 1C).

Comparison of expression of NRBP2 at the protein and mRNA levels between ICC tissues and neighbor tissues. A, Different NRBP2 levels of IHC results for cancer tissue and neighbor tissues are shown. B, Percentage of NRBP2 expression in 29 paired cancer and adjacent tissues was analyzed. C, The mRNA level of NRBP2 in 24 paired ICC cancer tissues and adjacent tissues were analyzed. P < .05 demonstrates significant difference. ICC indicates intrahepatic cholangiocarcinoma; IHC, immunohistochemistry; mRNA, messenger RNA; NRBP2, nuclear receptor binding protein 2.
Overexpression of NRBP2 Was Associated With Better Prognosis of Patients With ICC
To further study the relationship between expression of NRBP2, clinicopathological features, and patient prognosis, we divided these 29 patients into 2 groups according to NRBP2 expression: those with IHC score ≥6, the high expression group, and those with IHC score <6, who comprised the low expression group. Next, we used χ2 tests to analyze the correlation between NRBP2 expression and clinical features, and we observed that the expression of NRBP2 was associated with tumor size and tumor grade; those who had low expression of NRBP2 was always along with large tumor size and poor tumor grade (P < .05; Table 1). However, there was no significant difference in univariate and multiple variable analyses (Supplement Table 1). To determine whether expression of NRBP2 was correlated with prognosis of patients with ICC, we used Kaplan-Meier survival analysis and observed that patients with high expression of NRBP2 may have better prognosis than patients with low expression (Figure 2).
Relationship Between NRBP2 Expression and Clinicopathologic Features.
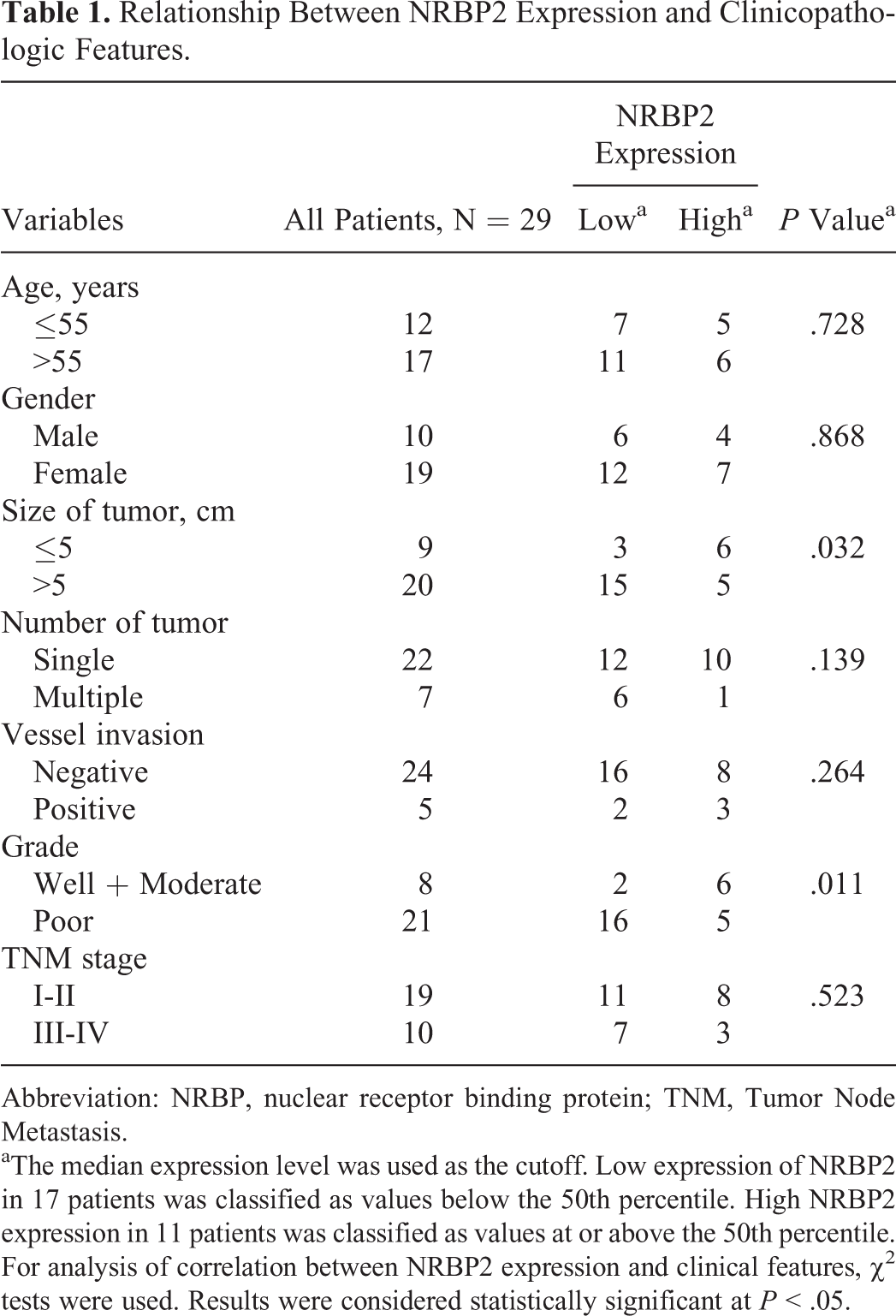
Abbreviation: NRBP, nuclear receptor binding protein; TNM, Tumor Node Metastasis.
aThe median expression level was used as the cutoff. Low expression of NRBP2 in 17 patients was classified as values below the 50th percentile. High NRBP2 expression in 11 patients was classified as values at or above the 50th percentile. For analysis of correlation between NRBP2 expression and clinical features, χ2 tests were used. Results were considered statistically significant at P < .05.

Results of the Kaplan-Meier survival analysis between the NRBP2 low-expression group and the NRBP2 high-expression group in 29 patients with ICC. NRBP2 indicates nuclear receptor binding protein 2.
Overexpression of NRBP2 Inhibits Proliferation of CCA Cells by Inducing G1 Arrest
To investigate the function of NRBP2 in a CCA cell line, we constructed NRBP2 overexpression in RBE and CCLP cell lines, and the transfection efficiency was verified by Western blot analysis and RT-PCR (Figure 3A, B). Next, we used the CCK-8 assay to compare cell viability between NRBP2 overexpression in cells and negative control cells. The results showed that cells with NRBP2 overexpression reflected lower viability than normal cells (Figure 3C). To confirm whether such a situation was affected by increasing cell apoptosis or decreasing cell proliferation, we detected cell apoptosis by flow cytometry and observed that overexpression of NRBP2 can slightly induce cell apoptosis; the expression of caspase3 and cle-caspase3 had no change (Figure 3D). However, such apoptosis changes cannot imply the substantial change in cell viability. Therefore, we suppose that overexpression of NRBP2 can decrease cell viability by decreasing the cell proliferation rate. Thus, we compared the cell cycles between NRBP2 overexpressed cells and negative control cells by flow cytometry, and we observed that overexpression of NRBP2 can decrease the cell proliferation rate by inducing G1 phase arrest in the cells (Figure 4A). In addition, such results were also verified by Western blotting with overexpression of NRBP2, and the protein levels of CDK2, CDK4, and cyclinA2 were decreased, which had a core role in the progression of cell G1 phase; however, the expression of CDK6 and CyclinD showed no change (Figure 4B).

Overexpressed NRBP2 in CCA cells was associated with a decrease in the cell proliferation rate. A and B, Results for efficiency of NRBP2 transfection in RBE and CCLP cell lines; GAPDH was used as internal control. C, The CCK-8 results between NRBP2 overexpression and negative control. ***P < .001. D, Apoptosis results by flow cytometry are shown. Cell percentage of each apoptosis phase was analyzed, and the expression of pro-caspase-3 and cle-caspase-3 was detected. CCA indicates cholangiocarcinoma; CCK-8, Cell Counting Kit-8; NC, negative control; NRBP2, nuclear receptor binding protein 2; NRBP2-OE, NRBP2 overexpression.

Overexpressed NRBP2 in CCA cells can lead to G1 phase arrest. A, Cell cycle results by flow cytometry are shown. Cell percentage of G1/S/G2 phase was analyzed. *P < .01. B, Western blotting results for expression of CDK2, CDK4, CDK6, CyclinD, and CyclinA2. GAPDH was used as internal control. CCA indicates cholangiocarcinoma; NRBP2, nuclear receptor binding protein 2
Overexpression of NRBP2 Can Inhibit Cell Migration by Suppressing CCA Cell EMT
Since overexpression of NRBP2 can decrease the cell proliferation rate in CCA, we suppose whether it can regulate cell migration. To confirm our hypothesis, we detected cell migration by Transwell assay in the NRBP2 overexpression cell line and negative control cell line. The results showed that the NRBP2 overexpression cell line had lower migration ability than the negative control (Figure 5A). Next, further study was conducted for the internal mechanism. We detected EMT-associated proteins by Western blotting and observed that overexpression of NRBP2 can induce the upregulation of E-cadherin and downregulation of N-cadherin, vimentin, and β-catenin, but the expression of MMP2 showed no change (Figure 5B). Such results showed that overexpression of NRBP2 can inhibit RBE and CCLP cell migration by suppressing the cell EMT.

Overexpressed NRBP2 in CCA cells was associated with a decrease in cell migration ability. A, Results of the Transwell assay are shown. Cell migration was analyzed and compared. ***P < .001. B, Results of the wound healing scratch assay at 0 and 48 hours from NRBP2 overexpression and negative control in CCA cells. C, Western blot results for expression of E-cadherin, N-cadherin, vimentin, β-catenin, and MMP2. β-actin was used as internal control. CCA indicates cholangiocarcinoma; NRBP2, nuclear receptor binding protein 2.
Overexpression of NRBP2 Can Increase Cisplatin Sensitivity in CCA Cells
To investigate whether NRBP2 was associated with drug sensitivity in CCA cells, we compared cell viability of RBE cells with NRBP2 overexpression and negative control under different concentrations of cisplatin (0, 0.25, 0.5, 1.0, 1.5, and 2.0 μg/mL). As Figure 6A showed, overexpression of NRBP2 can increase cisplatin sensitivity of RBE cells. Considering mTOR signal was associated with cell drug resistance, we detected expression of mTOR, p-mTORser2481, and p-mTORser2448 and determined that overexpression of NRBP2 can decrease the expression of these proteins (Figure 6B). Thus, we preliminarily showed that NRBP2 could affect cisplatin sensitivity by regulating the activity of mTOR signaling. Next, we used mTOR siRNA to conduct a rescue experiment and observed that the effect of suppression of mTOR in cisplatin sensitivity of RBE cells was the same as the NRBP2 overexpression group or both NRBP2 overexpression and mTOR siRNA groups (Figure 6C). Software analysis showed that both NRBP2 overexpression and mTOR siRNA can decrease the IC50 (half maximal (50%) inhibitory concentration (IC) of a substance) values of cisplatin (Supplement Table 2). The efficiency of mTOR siRNA is shown in Figure 6D.

Overexpressed NRBP2 in CCA cells was associated with increase in cisplatin sensitivity. A, Cell viability of RBE-NRBP2 overexpression and RBE-NRBP2-NC was detected under different concentrations of cisplatin (µg/mL); *P < .05, **P < .001. B, Protein levels of mTOR, p-mTORser2481, and p-mTORser2448 in RBE cells with NRBP2 overexpression (NRBP2-OE) and NRBP2 negative control (NRBP2-NC). C, Cell viability of NRBP2-OE, mTOR-siRNA, NRBP2-OE + mTOR-siRNA, and negative control was detected under different concentrations of cisplatin (µg/mL). *P < .05, **P < .001. D, Transfection efficiency of siRNA-mTOR was verified by Western blot analysis. CCA indicates cholangiocarcinoma; NRBP2, nuclear receptor binding protein 2.
Discussion
Cholangiocarcinoma accounts for 3% of all gastrointestinal cancers, and it is the second most common primary hepatic tumor after HCC. 8,9 Even the prognosis of CCA is worse than HCC, while a correlated study for CCA was less than HCC. Thus, more studies are warranted to investigate the initial diagnosis and progression of CCA. As CCA was stratified according to surgical criteria (eg, extrahepatic, intrahepatic, and hilar), our study primarily investigated the function of NRBP2 in the progression of ICC.
A recent study by Zhang and his colleagues showed that overexpression of NRBP2 can increase chemosensitivity of HCC cells by regulating the AKT signaling pathway. 7 Nuclear receptor binding protein 2 is a gene with unknown function and has a similar amino acid sequence to NRBP1. 4,5 Nuclear receptor binding protein1 has been reported as a tumor suppression gene in many cancers, including breast cancer 10 and intestinal tumors. 11 As homologous protein function may be similar, we proposed that NRBP2 may play a tumor suppression role in ICC. We first detected the NRBP2 expression level in ICC patient tissues and found that NRBP2 was almost downregulated in ICC tissues compared to neighbor noncancer tissues. This result was repeated at the mRNA level in 24 paired ICC tissues. Single factor analysis showed that expression of NRBP2 was correlated with ICC tumor size and tumor grade. Patients with low expression of NRBP2 were associated with large tumor size and poor tumor grade. Next, we used Kaplan-Meier survival analysis to study whether expression of NRBP2 was correlated with prognosis of patients with ICC. The results showed that overexpression of NRBP2 reflected a better prognosis for patients with ICC. Although the results of Cox’s regression analysis showed no significant difference, the primary reason was the small sample size for this study. Based on these results, we preliminarily demonstrated that downregulated NRBP2 played an important role in the progression of ICC.
To investigate the function of NRBP2 in the CCA cell line, we constructed an NRBP2 overexpression plasmid and negative control and transfected them into RBE and CCLP cell lines to detect the change of cell proliferation and migration. We found that overexpression of NRBP2 led to a decrease in the cell proliferation rate, and such function was affected slightly by cell apoptosis. Cell cycle phase was important for cell proliferation, as each phase had its own checkpoint, and only after passing through the detection of checkpoint can the cell proliferate for the next generation. 12,13 Therefore, we used flow cytometry to detect whether something was different in the cell cycle. As expected, we observed that overexpression of NRBP2 induced G1 phase arrest. Considering CDK2, CDK4, CDK6, CyclinD, and CyclinA2 have an important role in regulating cell G1 phase, 14,15 we detected these proteins by Western blot analysis and observed that CDK2, CDK4, and CyclinA2 were decreased under the conditions of NRBP2 overexpression in RBE and CCLP cell lines.
Most patients with CCA are ineligible for curative surgery because of the presence of metastasis at the time of diagnosis. 16 During the past several years, EMT, which is a reversible dynamic process during which epithelial cells gradually adopt structural and functional characteristics of mesenchymal cells, has garnered considerable attention regarding metastatic dissemination. 17 –19 Therefore, we investigated whether NRBP2 played an important role in the regulation of migration of CCA cells. We used a Transwell assay to detect cell migration, and we observed that the migration ability of RBE and CCLP cell lines with overexpression of NRBP2 was weaker than the negative control. We also detected some EMT proteins, including E-cadherin, N-cadherin, vimentin, and β-catenin, and observed that E-cadherin was upregulated while N-cadherin, vimentin, and β-catenin were downregulated under the condition of NRBP2 overexpression. Combined with the above results, we demonstrated overexpression of NRBP2 could inhibit β-catenin-associated cell EMT process in the CCA cell line.
Recent studies revealed that inhibition of mTOR signaling using rapamycin can enhance sensitivity of cancer cells to cisplatin and doxorubicin. 20,21 Our study observed that overexpression of NRBP2 can decrease activity of mTOR signaling and enhance cisplatin sensitivity of CCA cells; combining that NRBP2 was associated with chemoresistance in HCC, we imagined NRBP2 may be an important target for improving efficiency of clinical chemotherapeutics for HCC and CCA.
However, as we only collected 29 paired patient tissues for this study, a larger sample size is needed for repetition of results. Meanwhile, further research needs to be conducted to illustrate the mechanism of NRBP2 on proliferation and migration of CCA cells. Overall, our study observed that NRBP2 was downregulated in ICC tissues, and overexpression of NRBP2 was associated with better prognosis of patients with ICC. In addition, overexpression of NRBP2 can affect proliferation, migration, and cisplatin sensitivity of CCA cells by inducing G1 phase arrest, inhibiting the EMT process, and regulating mTOR signaling activity.
Footnotes
Abbreviations
Authors’ Note
The Second Affiliated Hospital, Xi’an Jiaotong University Ethics Committee approved this study. Informed consent was obtained from all individual participants included in the study. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.