
Abstract
Multiple myeloma is a monoclonal B-cell malignancy characterized by an accumulation of malignant plasma cells in the bone marrow, the presence of a monoclonal protein in the serum and/or urine, decreased normal immunoglobulin levels, and lytic bone disease. Patients with multiple myeloma benefit from combination therapy including novel therapeutic agents followed by autologous stem cell transplantation prolonged maintenance therapy. However, multiple myeloma remains incurable; most patients with multiple myeloma will eventually become resistant to chemotherapy, and progression or relapse of the disease is inevitable. Immunotherapy represents a novel therapeutic approach with few adverse effects and good targeting capability that might be a powerful pool to allow long-term control of minimal residual disease. This article reviews the literature evaluating 4 major immunotherapeutic approaches for multiple myeloma including cellular immunotherapy, humoral immunotherapy, radio immunotherapy, and immunomodulation.
Keywords
Introduction
Multiple myeloma (MM), also called plasma cell myeloma, is the second most common hematological malignancy after non-Hodgkin’s lymphoma. 1 Standard treatment of MM consists of an initial induction using immunomodulatory agents (thalidomide or lenalidomide) or the proteasome inhibitor bortezomib combined with dexamethasone or chemotherapy, followed by autologous stem cell transplantation (auto-SCT) for patients younger than 65 years and consolidation/maintenance therapy. Allogeneic hematopoietic stem cell transplantation (allo-SCT) is a potentially curative option for patients with MM that offers several advantages, including a tumor-free graft and the potential for sustained immune-mediated disease control. However, historically high treatment-related mortality and conflicting reports from prospective studies in the United States and the European Union have limited the utilization of this method. One of the clinically available types of immunotherapy for MM is allo-SCT, where there is evidence that graft versus MM can produce responses and even cures in a small subset of patients. Despite gratifying results with current drug therapies and auto-SCT, the majority of patients relapse because of the persistence or appearance of multidrug-resistant plasma cell clones. 2 MM remains incurable, highlighting the need for new approaches.
Immunotherapy is a promising approach in MM, because many tumor-associated antigens (TAAs) have been identified in MM cells, and tumors develop immunosuppression. Different forms of immunotherapy have been investigated and validated in preclinical in vitro and in vivo models. Immunotherapy can focus on the recovery of immune surveillance and can block tumor development, which is not different from direct tumor cytotoxicity by traditional chemotherapy. 3 Although the pembrolizumab trials in myeloma were recently halted by the US Food and Drug Administration (FDA) because of safety, immunotherapy, on the whole, also showed small adverse effects and satisfactory results, especially for patients with refractory and recurrent disease. However, many challenges have to be addressed before immunotherapy can be used to treat patients with MM, such as the identification of a perfect target antigen for vaccination strategies, the occurrence of myeloma resistance, and the general immunosuppressed state of MM which hinders immune cell-based treatment approaches. In this review, we summarized the general immune alterations observed in patients with MM.
Cellular Immunotherapy
Allogeneic SCT is a form of cellular immunotherapy that employs the donor’s immune system to combat myeloma. Allogeneic SCT has been shown to produce durable responses in patients with MM who received grafts from HLA-matched sibling donors. Despite the development of a supportive treatment, allo-SCT is still not routinely employed due to the lack of survival advantage over auto-SCT. Its limited efficacy and associated toxicities have prevented its widespread use. Cellular immunotherapies aim to induce a more specific, reliable, and potent anti-MM response with less treatment-related risk than with allo-SCT. 4,5
Vaccines for Myeloma Based Upon Dendritic Cells
Dendritic cells (DCs) are a new type of immunocompetent cells initially purified from the mouse spleen. 6 Dendritic cells were eventually found in other tissues, and DC lines were established in vitro. The number of DCs accounts for less than 1% of peripheral blood mononuclear cells (PBMCs), but the surfaces of DCs are rich with antigen-presenting molecules, stimulatory factors, and adhesion factor. Therefore, DC is the only cell type to activate the initial model antigen-presenting cells, effectively presenting tumor antigen of MM cells to T cells, and then produce specific cytotoxic T lymphocytes (CTLs) that can kill MM cells. 7
Dendritic cell-based vaccines are modified by differentiation, maturation, and antigen uptake steps by monocytes of patients with MM. The vaccines demonstrated feasible, well-tolerated, and good antitumor response in patients with MM. 8 Currently, DCs are being used in phase I/IIa clinical trials in patients with refractory or relapsed MM (RRMM; eg, NCT02248402, NCT01472627, NCT02335983, NCT02559583, and NCT0255958). Among them, isolated idiotype (Id), MM cell lysates, dying MM cells, DC–myeloma hybrids, or DC transfected with tumor-derived RNA were used for immunotherapy with DCs. Although DC-based vaccines promise a new horizon for extending the survival of patients with MM, it also encountered numerous challenges: Although immune responses have been observed in many clinical trials, the response of clinical trials was rarely improved after DC vaccinations in patients with MM. There are many possible reasons for this result: Id protein is a weak antigen; DCs loaded with antigens derived from whole tumor cells can induce an autoimmune reaction; or immature DCs may have been used. Therefore, TAAs could be a major interest in MM immunotherapy. A variety of MM-associated antigens have been identified in patients with MM, which may provide an immune response by DC-based vaccines, including human telomere reverse transcriptase, polymorphic epithelial mucin, preferentially expressed antigen in melanoma (PRAME), HM1.24 (also known as bone marrow stromal cell antigen 2 (BST2) or CD317), Sperm protein 17 (SP17), Wilms tumor I, Dickkopf-1, or a member of the cancer germ-like family (melanoma-associated antigen [MAGE], G antigen [GAGE], B antigen [BAGE], L antigen [LAGE], New York esophageal squamous cell carcinoma 1 [NYESO-1]). 9 –14 For improving the outcomes of DC-based immunotherapy in patients with MM, we can focus on alternative approaches, such as enhancing DC function, inducing specific CTLs by activating effective tumor antigens, or modifying signal transcriptions. Experience in the DC research field has revealed several key points to improve DC vaccination in patients with MM. In general, the production of a DC vaccine has become promising in inducing immunotherapy against MM.
Natural Killer and Natural Killer T Cells
The inefficacy of natural killer (NK) cells is due to their inability to recognize and attack malignant plasma cells of the immune system in patients with MM. Natural killer cells can mediate the lysis of cells that express decreased major histocompatibility complex class I (MHC I) levels, such as virally infected or tumor cells. They also express attacking activating receptors, such as NKG2D, natural cytotoxicity receptors, and killing inhibitory receptors (KIRs). The ligands of NKG2D activating receptor are MHC I-like molecules MICA and MICB (MHC I chain-related protein A and B). Natural killer cell–mediated lysis is inhibited once the inhibitory signals are predominant through the binding of KIRs to their ligands on target cells, such as MHC I. However, when MHC I is absent or shows reduced expression, tumor cells can frequently use a strategy to evade lysis by CTLs, activating signals on NK cells that become predominant and lyse target cells. 15,16
Fauriat et al 17 demonstrated that NK cells in patients with MM showed a lower expression of CD16, which can mediate the antibody-dependent cell-mediated cytotoxicity (ADCC) function of NK cells. To activate and target NK cells to tumor cells in MM, von Strandmann et al 18 designed a recombinant bispecific protein (ULBP2-BB4, a novel bispecific protein targeting the NKG2D receptor), which binds to the activating NK receptor, NKG2D, while the BB4 moiety can bind CD138. ULBP2-BB4 can strongly activate primary NK cells after the increased secretion of interferon-γ (IFN-γ). The use of recombinant NK receptor ligands, which target NK cells to MM cells, might also offer new approaches for other tumors, provided that a tumor antigen-specific antibody is available. Moreover, NK cells in patients with MM express programmed death 1 (PD-1), whereas normal NK cells do not. Lenalidomide could downregulate programmed death-ligand 1 (PD-L1) expression on MM cells and act synergistically with the anti-PD-1 antibody. 19 Infusion of allogeneic NK-cells has shown promise as a means of inducing remission in patients with MM, and several clinical trials are ongoing. Allogeneic adoptive transfer of NK-cells has shown a consistently high safety profile with a low incidence of graft-versus-host disease (GVHD), while increasing the survival and, in some cases, resulting in complete remission (CR) in patients with cancer with a poor prognosis. However, multiple issues remain such as the low yield of allo reactive NK-cells, the loss of activating receptors, the cytotoxic potential in transferred NK-cells, and the failure of NK-cells to persist in vivo following transfer. Thus, the rapid expansion of MM-targeting NK-cells needs to be improved.
Studies of NK-cell functionality are also significant, considering that the novel monoclonal antibodies (mAbs) evaluated for MM therapy, such as elotuzumab, XmAb5592, and anti-CD137 mAbs, rely upon NK-cell-mediated ADCC. 20 –24 Elotuzumab is a first-in-class humanized IgG1 immunostimulatory mAb targeting SLAMF7 (signal lymphocyte activator family member 7 also known as CS1). The mechanisms of the antitumor effects of elotuzumab include disrupting MM cell adhesion to bone marrow stromal cells (BMSCs), enhancing NK cell cytotoxicity, and mediating ADCC, but not complement dependent cytotoxicity. Thus, these findings underscore the significance of heightening the sensitivity of MM cells to NK-cell lysis or the ability of NK cells to induce MM cell lysis.
Natural killer T cells (NKT) are characterized by CD1d-restricted T cells and display NK characteristics. Different subtypes of NKT cells have been described: type I or invariant NKT cells (Vα24+β11+) and type II NKT cells (Vα24−β11−). In patients with progressive MM, type I NKT cells are functionally imperfect due to a low expression of ligand-dependent IFN-γ production. 25 In addition, a distinct type II NKT cells, which can bind to inflammation-associated lysophospholipids and are present in the plasma of patients with MM, has been confirmed. 26 Many studies have demonstrated that therapy targeting NKT cells coupled with glycolipid-loaded DCs 27 or immunomodulatory drugs (IMiDs) 28 has achieved a satisfactory outcome. However, most of the current studies have been based on small number of patients and are in an early phase. Continued careful investigation of the biology of NKT cells may allow harnessing their properties for the benefit of patients with MM.
Chimeric Antigen Receptor T cells
In recent years, the development of genetically engineered technology to express tumor-specific chimeric antigen receptor (CAR) T cells (CAR T cells) has shown encouraging results in killing tumor cells and provides new solutions for adoptive immunotherapy. Chimeric antigen receptors T cells are autologous or allogeneic T cells genetically engineered to express a CAR specific for a cell-surface molecule, typically a protein or carbohydrate. 29 CD19 CAR T cells, engineered to express a CAR against CD19, were recently shown in small feasibility studies to provide clinical benefit to patients with chronic lymphocytic leukemia and B-cell acute lymphoblastic leukemia. 30
Chimeric antigen receptors T cell therapy has also shown great promise in treating MM. Many mAbs targeting MM surface antigens have been tested as therapeutic products (Table 1). There are also other potential MM surface antigens, such as lipid raft-associated protein, bone marrow stromal antigen 2, the neural cell adhesion molecule (CD56), and the HLA-DR antigen-associated invariant chain CD74. While multiple questions remain, including questions about the potential toxicities to patients with MM, which patients are suitable for CAR-T cells, and the role that CAR-T cells in the management of MM. 31 To date, the results of clinical trials have shown that CAR T cells directed against CD19, CD138, and κ-light chain. Despite the lack of CD19 expression on plasma cell clones, some studies have identified CD19 expression on a minor MM stem cell subset, making CD19 a promising target for eliminating recurrence following elimination of differentiated plasma cells. New research shows that bb2121 (anti-B cell mature antigen CAR T cells) shows promising efficacy in patients with RRMM: The overall response rate in the 6 evaluable patients was 100%. 32 These initial data support the potential application of CAR T cell therapy with bb2121 as a new treatment paradigm in MM.
Ongoing Clinical Studies of CAR-T Cells in MM.
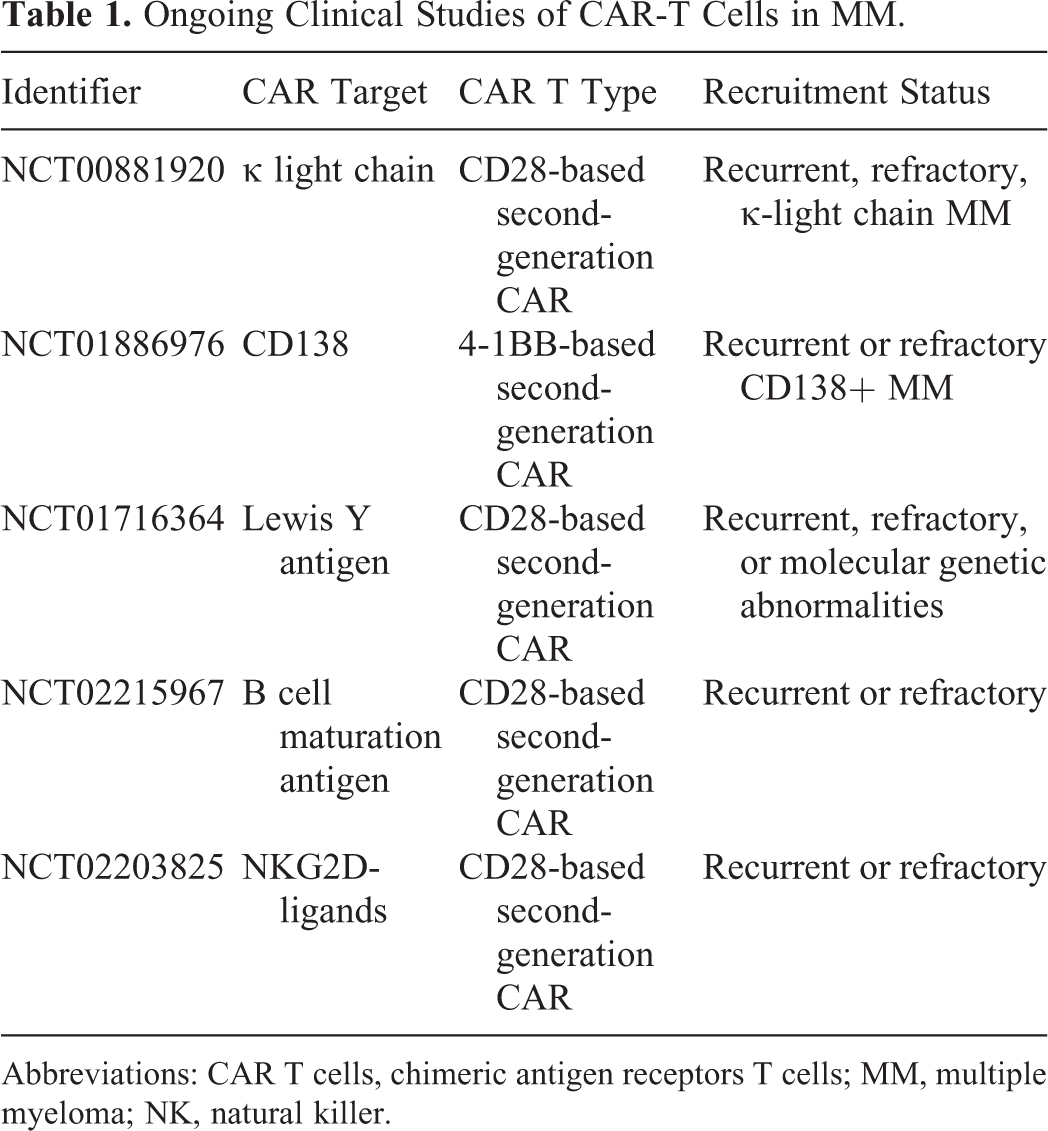
Abbreviations: CAR T cells, chimeric antigen receptors T cells; MM, multiple myeloma; NK, natural killer.
Detailed planning of clinical trials will be needed to bring this new technology from the bench to the bedside of patients with MM. The key elements of the clinical trials include discovering the MM patient population most likely to respond to CAR T-cell therapy and determining the timing of the multiple therapy options available, including the possible combination with other treatments such as autologous stem-cell transplantation (ASCT), immune checkpoint inhibitors, or immunomodulators and the cost of these combinations.
Humoral Immunotherapy
Monoclonal Antibody
Rituximab, a monoclonal antibody against the CD20 antigen expressed on B cells, was first approved by the US FDA in 1997 for the treatment of non-Hodgkin’s B-cell lymphoma, which opened the route to efficient mAb immunotherapy. 33,34 The antigens (Tables 2 and 3) targeted in MM therapy are involved in cell survival, antiapoptotic pathways, angiogenesis, cell-to-cell communication, and interactions between MM cells and BMSCs. 35,36 The results from studies of patients with RRMM have shown enhanced therapeutic efficacy with daratumumab (DARA) and elotuzumab. 37 Following the work developing functional antibodies, substantial efforts are underway to develop therapies that can use antibodies conjugated with traditional potent cytotoxic agents. Many highly cytotoxic compounds are being assessed for antibody-based delivery, such as IMGN90, which consists of a humanized mAb that binds with high affinity to CD56 conjugated with the cytotoxic maytansinoid DM1 (N(2’)-deacetyl-N(2’)-(3-mercapto-1-oxopropyl)-maytansine). 38 BT062 is a chimeric mAb conjugated to maytansinoid derivatives, and many studies on BT062 have reported significant antitumor activity. 39,40
Monoclonal Antibodies in MM: Ongoing Clinical and Preclinical Development.

Abbreviations: ADDC, antibody-dependent cell-mediated cytotoxicity; CDC, complement dependent cytotoxicity; DKK1, Dickkopf-1; IGR-1, insulin-like growth factor 1; IL-6, interleukin 6; mAb, monoclonal antibody; MM, multiple myeloma; NK, natural killer; PD-1, programmed death 1; VEGF, vascular endothelial growth factor; RANKL, Receptor Activator for Nuclear Factor-κ B Ligand; OB osteoblast.
Monoclonal Antibodies in MM: Completed Clinical Trials.

Abbreviations: B, bortezomib; BP, biochemical progression; CR, complete remission; IL-6, interleukin 6; KIR, killing inhibitory receptors; mAb, monoclonal antibody; MR, minimal response (>25% and <50% decrease in M-protein); OS, overall survival; PFS, progression-free survival; plc, placebo; SD, stable disease; S + VMP, siltuximab + bortezomib + melphalan + prednisone.
Daratumumab is a first-in-class, fully human IgG1 κ (IgG1κ) mAb against a unique CD38 epitope in plasma cells that has been recently been approved for patients with RRMM. Daratumumab single agent and in combination with protease inhibitor (PI) and IMiDs has shown outstanding clinical activity even in heavily treated patients with RRMM. 41 –45 Regarding the safety profile of this new drug, the results of clinical trials do not show significant increase in toxicity. The most relevant adverse effects are those associated with infusion of the drug, most of them observed during the first administration with a grade 1-2 intensity. These effects are more pronounced with prolonged administration times (up to 7-8 hours) especially during the first infusion. These effects could be minimized in the future with the development of the subcutaneous injection (SC) formulation of DARA currently under investigation. 46 –50
Some of the antibodies we discussed are under development or in preclinical phase I or phase II trials. These antibodies are generally well tolerated and show a safety profile that is distinct from current treatments. However, in the current monoclonal antibody drug research and development, many problems still exist, such as drug delivery mode optimization, biocompatibility improvement, traditional treatment versus reasonable combination, the high cost, and the body’s resistance. Data from future larger studies will reveal how much of an impact these agents will make on the long-term survival and the quality of life in patients with MM. 51
Immune Checkpoint Blockers
Therapeutic blockade of immune checkpoint pathways, in particular CTL-associated protein 4 and PD-1, has become a paradigm-shifting treatment in solid tumor oncology. Multiple myeloma was also included as an independent expansion arm in the phase 1 studies of nivolumab (anti-PD-1) and pembrolizumab (anti-PD-1). This inclusion was based on promising preclinical data that demonstrated the expression of PD-1 and PD-L1 on MM cells and in the MM microenvironment. 62,63 Furthermore, animal model data suggested that PD-1 blockade could enhance the effect of immunotherapy. 64 However, preliminary results suggest that the effect is not significant in MM.
Nivolumab (OPDIVO) is a fully human IgG4 mAb against the PD-1 receptor. A recently published phase 1 clinical trial evaluating nivolumab monotherapy in patients with MM revealed no objective responses. Based upon 27 patients with RRMM, 63% (17/27) reached stable disease (SD) as a best response. 65
Pembrolizumab (KEYTRUDA) is a highly selective, humanized IgG4 mAb against the PD-1 receptor. Preliminary results of the phase 1 study of pembrolizumab and lenalidomide plus low-dose dexamethasone in patients with RRMM showed that 48% (19/40) of patients had SD resulting in a disease control rate of 98%. Its safety profile was acceptable with a low rate of immune-mediated adverse events (AEs) and no reported pneumonitis or colitis. 66 It is becoming evident that the results of monotherapy treatment with PD-1/PD-L1 inhibitors in MM are unsatisfactory and that a combination approach is needed. The most logical partners are immunomodulatory agents as they possess many synergistic effects. However, the potential toxicity of IMiDs in combination with pembrolizumab has resulted in the FDA halting all IMiD/pembro combinations (eg, NCT02576977, NCT02579863).
Immunotherapy is revolutionizing oncology and the perspectives of immune checkpoint blockers in hematologic malignancies are vast and enticing. However, immune checkpoint blockers are unlikely to be a panacea in patients with MM, and much remains to be done in a coordinated and judicious fashion to maximize its therapeutic potential.
Radioimmunotherapy
Many new therapeutic methods have led to an increase in the survival of patients with MM. Therefore, maintaining their CR status by improving the elimination of minimal residual disease (MRD) after induction therapy is the primary goal of MM therapy. Radioimmunotherapy (RIT) selectively delivers radiation to target cells at multiple disease sites and facilitates the escalation to radiation doses not achievable through external beam therapy. Indeed, the use of mAbs has shown to be a realistic strategy for targeted delivery of therapeutic radionuclides to tumor cells in various B-cell malignancies. Therefore, whether RIT can become a standard therapeutic modality depends on the selection of a radionuclide antibody. 67,68
Cherel et al 69 demonstrated promising therapeutic efficacy of 213Bi-labeled anti-mCD138 for the treatment of residual disease in MM with only moderate and transient toxicity in an MM mouse model. Green et al 70 demonstrated that, compared with conventional RIT (directly radio-labeled antibody), streptavidin-biotin pretargeted RIT directed against CD38 antigen can greatly improve the intensity of radiation within the organism; a dose of up to 800 to 1200 Ci, up to the 23rd day of treatment, showed a 100% CR in an MM mouse model.
Several radiolabeled compounds have been shown to be effective in early-phase clinical trials as well as in preclinical studies. The preliminary results are also confirmed. To date, mAb is a common delivery vehicle, but antibodies are large molecules. Smaller molecules travel better, penetrate the tumor tissue better, and are excreted much more swiftly when released into circulation.
Research efforts are now shifting to these smaller molecules to better exploit the effects of radioisotopes. 71 With the development of engineering technical support, more new RIT drugs will be developed. The use of RIT represents an important area for future research and could provide substantial benefit to patients.
In summary, MM offers several promising targets for the CAR-based immunotherapies with many potential issues of integration with current treatment paradigms. It will be an impactful advance in the treatment of patients with MM to develop an active antimyeloma CAR.
Immunomodulation
Thalidomide, as the first generation of the IMiD class, was introduced as a sedative for preventing nausea during pregnancy in the late 1950s and was found to be effective against MM by Singhal in 1999. 72 Thalidomide can significantly improve the response rate and survival of patients with MM. 73 –76 Lenalidomide and pomalidomid, which were the second generation of IMiDs, had a greater potential in anti-MM, anti-inflammatory, and immune modulatory activities than thalidomide. 77,78 The molecular mode of action of IMiDs in MM includes direct and indirect mechanisms. 79,80 With regard to the direct mechanisms, previous studies had shown several downstream changes after treatment with IMiDs, which may be of great significance in the direct antimyeloma activity of IMiDs, such as upregulation of P21wafl expression, 81 inactivation of nuclear factor-κB, 82 downregulation of C/EBPβ (enhancer binding protein), 83 and activation of caspase 8. 84 With regard to the indirect mechanisms, IMiDs can downregulate the expression of surface adhesion molecules on both MM cells and BMSCs, such as interleukin-6 (IL-6), insulin-like growth factor 1, and vascular endothelial growth factor, and interfere with the interaction of MM cells and BMSCs. 85 Moreover, IMiDs can also induce T-cell proliferation and enhance IL-2 and IFNγ production. They can also enhance both NK cell-mediated cytotoxicity and ADCC induced by triggering IL-2 production by T cells. 86 Finally, IMiDs negatively regulate the production of pro-inflammatory cytokine tumor necrosis factor-α , IL-1, IL-6, and IL-12 by human PBMCs. 77
Although many mechanisms have been put forward to account for the effects of thalidomide, lenalidomide, and pomalidomide in MM, including demonstrable antiangiogenic, antiproliferative, and immunomodulatory effects, the precise cellular targets and molecular mechanisms have only recently become clear. A recent study suggests that IMiDs can combine with cereblon (CRBN), a protein previously reported to associate with autosomal recessive nonsyndromic mental retardation. 87 CRBN could activate the enzyme activity of CRBN E3 ubiquitin ligase complex and promote the proteolysis of transcription factor IKZF1 and IKZF3, leading to toxic effects on MM cells. Therefore, CRBN was identified as a potential target of the treatment efficacy of IMiDs.
The emergence of immune modulation is a major breakthrough in the history of MM treatment. Thalidomide and lenalidomide have established roles in the treatment of newly diagnosed patients with RRMM. Pomalidomide has been evaluated in clinical trials, and clinical data suggest that it is active in patients with MM refractory to bortezomib and lenalidomide treatment. 88 With continuous improvement, IMiDs will likely have a significant impact on patients with MM, through their potential role in MM consolidation or maintenance therapy and through their prophylactic use by asymptomatic patients to prevent the development of active MM. Studies also indicate that macrophage reprogramming strategies may provide significant clinical benefit for patients with MM. Tumor-associated macrophages are important components of the MM microenvironment that support malignant plasma cell survival and resistance to therapy. Thus, IMiDs may show a great potential benefit. 89
Conclusions
Multiple myeloma continues to be an incurable disease and is fatal for a majority of patients at advanced stages. Exploring of novel therapeutic should be pursued. The introduction of bortezomib, thalidomide, and lenalidomide has prolonged the survival of patients with MM. The major concern may be the drug resistance or relapse of disease. Growing knowledge of the complexities of the immune system has led to a better understanding of how it can be harnessed for the purpose of anticancer therapy. Over the last few years, the idea of blocking cancer progression through immunological means has slowly become a reality. Recent studies have shown the great significance of immunotherapy in the treatment of patients with recurrent and refractory MM.
Immunotherapy is promising and may be effective in eradicating the malignant stem cell pool that is nonproliferating and generally resistant to chemotherapy. New methods of identifying tumor antigens, molecular and genetic manipulation of the immune system, and fundamental understanding of immunobiology have led to new breakthroughs and renewed interest by the pharmaceutical industry. The majority of immunotherapy is still in the experimental exploration stage, and the body’s immune system is a complex regulatory network. Thus, immunotherapy for MM has had the same challenges that the whole field of immunotherapy has been facing, but these new techniques may allow us to develop a cure for MM in the near future.
Footnotes
Abbreviations
Authors’ Note
Jing Ma and Qian Li contributed equally to this work. This article does not contain any studies with human or animal subjects performed by any of the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by key technologies R&D program of Tianjin (13ZCZCSY20300) and Science and Technology Project Affiliated to the Education Department of Tianjin (20140112).