
Abstract
Background and Objective:
Pulmonary embolism is potentially life-threatening in patients with lung cancer, but the clinical studies on patients with lung cancer having asymptomatic pulmonary embolism were barely reported.
Methods:
Clinical data of patients with lung cancer were obtained from the Department of Respiratory and Critical Care Medicine of Tianjin Chest Hospital during July 2012 and June 2015 and were reviewed retrospectively. A total of 28 patients with lung cancer having pulmonary embolism (LP group) were enrolled, and another 56 cases with lung cancer alone (LC group) were enrolled as controls.
Results:
Seventeen (60.7%) of 28 patients in the LP group developed adenocarcinoma, which was more frequent than that in the LC group (P < .01); the LP group displayed lower counts of hemoglobin and albumin than the LC group (P < .05); the counts of leukocyte (white blood cell) and
Conclusion:
Lung adenocarcinoma, chemotherapy, hyperleukocytosis, and
Introduction
There was a potential correlation between malignant tumor and venous thromboembolism (VTE) in 1865. Venous thromboembolism contains pulmonary embolism (PE) and deep vein thrombosis, which are the common complications in tumor disease progression and antitumor treatment, contributing to the massive deaths of patients with malignant tumor. 1 –3 It has been reported that the occurrence rate of VTE was 4% to 20% in patients with malignant tumor, 4 and VTE is commonly detected with complication of lung carcinoma clinically. Despite belonging to VTE, PE and deep vein thrombosis showed the major difference, especially in prognosis: Case fatality rate of patients with lung cancer complicating with PE is higher than other patients with VTE, and their median survival duration is also shortened. However, the symptoms and signs of lung cancer complicating with PE do not show specificity with solo lung cancer clinically. The typical character of PE disappears because its occurrence time advances, giving rise to missed and delayed diagnosis. The extensive usage of computed tomography (CT) scanning enhances the accidental diagnosis of asymptomatic pulmonary embolism (APE), especially in subsegmental or segmental PE, which is reported for its high risk. Thus, it is suggested that the early detection, early diagnosis, and early treatment of lung cancer complicating with PE significantly improve the prognosis of patients with lung cancer.
In the present study, 28 cases of lung cancer complicating with PE were retrospectively analyzed; meanwhile, 56 cases of lung cancer without PE complication were served as negative control. In the same term, spiral CT pulmonary angiography indicated no distinct PE. The clinical characteristic, risk factor, imaging feature, and prognosis have been investigated.
Methods
Object and Criteria
This study consisted of 28 (4.1%) patients with PE of 682 patients with lung cancer admitted in Tianjin Chest Hospital, during the period of June 2012 to June 2015. Inclusive criteria are lung cancer diagnosed by histologic or cytological examination. The diagnosis criteria referred to PE diagnosis treatment guidelines established by the Chinese Thoracic Society. 22 Acute PE diagnosis criteria and risk stratification referred to guide for diagnosis and treatment of acute PE established by European Society of Cardiology at 2014. Clinical staging was performed according to lung cancer staging revised by Union for International Cancer Control in 2009. Exclusive criteria were PE anamnesis and solo patients with lung cancer diagnosed with no PE or thrombotic diseases detected.
Data Acquisition
The following clinical data and lab indicator of patients have been collected: gender, age, life pattern, underlying disease, blood tests indicators, pathological pattern, tumor stage, and systemic chemotherapy. Pulmonary embolism imaging features were diagnosed. Time between PE diagnosis and lung cancer diagnosis, the last follow-up time, and death time were recorded. Follow-up visit was suspended until the death of patients or June 30, 2015. Survival time was recorded in unit of month.
Statistical Analysis
Statistical analyses were performed using SPSS software, version 17.0 (SPSS Inc, Chicago, Illinois). The data are expressed as means (standard deviations) or medians with range (minimum to maximum) if the data were skewed for continuous variables and as percentages for categorical variables. Between the 2 groups, the continuous variables were compared by χ2 test. Analysis of risk factors for lung cancer complicated with PE was done by logistic regression. To summarize the survival of the patients, we used the Kaplan-Meier test to construct survival curves, which were then compared with the results of log-rank tests. A P value <.05 was considered statistically significant.
Results
Demographics
The demographic data are summarized in Table 1. The average age of patients (n = 28, male/female = 18/10) with lung cancer combined with PE (LP group) was 66.25 (8.34) years. Adenocarcinoma (60.7%, n = 17) was the most common histological type of lung cancer, followed by squamous cell carcinoma (21.4%, n = 6), small cell carcinoma (14.3%, n = 4), and large cell carcinoma (3.6%, n = 1). According to Tumor Lymph Nude Metastasis (TNM) staging, 5 when PE was diagnosed, most of the patients with lung cancer were in stages III and IV (92.9%), followed by stages I and II (7.1%).
Comparison Between Patients With Lung Cancer Complicated With or Without PE.

Abbreviations: COPD, chronic obstructive pulmonary disease; LC, lung cancer alone setting as controls; LP, lung cancer combining with PE; PE, pulmonary embolism.
The average age of patients (n = 56, M/F = 38/18) in lung cancer alone, set as controls (LC group), was 63.45 (7.34) years. Among them, the number of patients with adenocarcinoma was 14 (25%), followed by squamous cell carcinoma, 20 (35.7%); small cell carcinoma, 19 (33.9%); and large cell carcinoma, 3 (5.4%). The number of patients with stages I and II lung cancer was 19 (33.9%), while those in stages III and IV were 37 (66.1%).
Clinical Characteristics
Among the 28 cases in the LP group, main clinical symptoms are cough and expiratory dyspnea, followed by stethalgia, palpitation, and hemoptysis. Occurrence of triad syndrome of PE was lower but expiratory dyspnea was higher than that in the group with lung cancer. These clinical symptoms increased in 11 patients with lung cancer after developing PE complication, while the exacerbation was not reported in the other 17 cases (Table 2). Hence, the LP group could be divided into 2 subgroups: 1 subgroup having lung cancer with APE (APE subgroup) and another having symptomatic PE (SPE subgroup), especially in the condition of Sa
Clinical Manifestation of Patients With Lung Cancer Complicated With or Without PE.
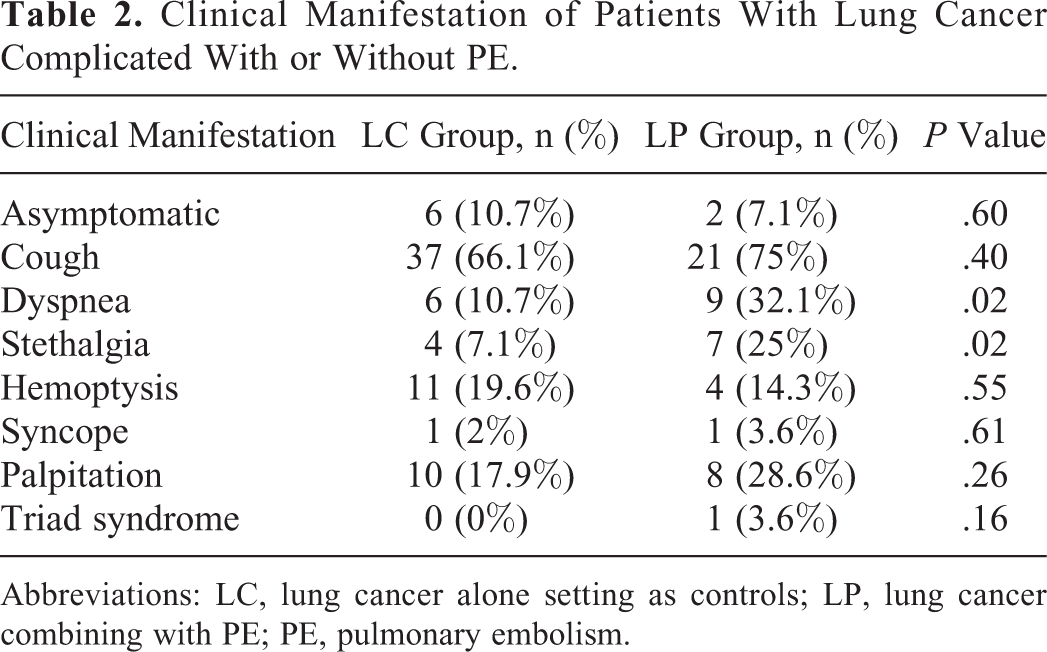
Abbreviations: LC, lung cancer alone setting as controls; LP, lung cancer combining with PE; PE, pulmonary embolism.
Blood pressure, heart rate, and oxyhemoglobin saturation of patients in the APE subgroup were monitored and all these indexes were in normal range; patients in the APE subgroup already had several nonspecific symptoms before the diagnosis of lung cancer.
Imaging Studies
Laboratory findings
Hemoglobin (Hb) and albumin (ALB) in the LP group were less than that in the LC group, while the white blood cell (WBC) count and
Image manifestation is filling-defect within the pulmonary artery detected by chest CT. In the SPE subgroup (n = 17), the most commonly used imaging modality in the diagnosis and position of PE was CT scanning. The frequency of the PE-involved pulmonary arteries was as follows: bilateral PE (n = 1), bilateral leaf artery PE (n = 3), bilateral segmental artery PE (n = 1), and unilateral segmental artery PE (n = 12). Multileaf artery or segmental artery could be involved in PE. In the APE subgroup, only 1 patient had large-sized PE, while in the SPE subgroup, there was no difference in PE position and morphology (Figure 1).

A, Pulmonary artery embolism in left lower lobe basal segment. B, Left lung ligule and lower lobe basal segment PE. C, Apical upper lobe, anterior segmental of right lung PE. PE indicates pulmonary embolism.
Single-Factor Analysis of Risk Factor in Lung Cancer Complicated With PE
The risk factors for lung cancer complicated with PE were underlying disease, life pattern, pathological pattern, neoplasm staging, and therapy. Discrepant risk factors between the LP and LC groups analyzed by single-factor analysis were adenocarcinoma, stages III and IV, systemic chemotherapy, and laboratory findings such as WBC count, DD, Hb, and ALB (as shown in Tables 1, 3, and 4). These factors were taken into account by logistic regression analysis; we found that adenocarcinoma, chemotherapy, hyperleukocytosis, and DD increment were the risk factors for lung cancer combined with PE (P < .05; Table 5).
Comparison of Lab Index.

Abbreviations: ALB, albumin; Hb, hemoglobin; LC, lung cancer alone setting as controls; LP, lung cancer combining with pulmonary embolism; PLT, platelet; SD, standard deviation.
Comparison of Lab Index.
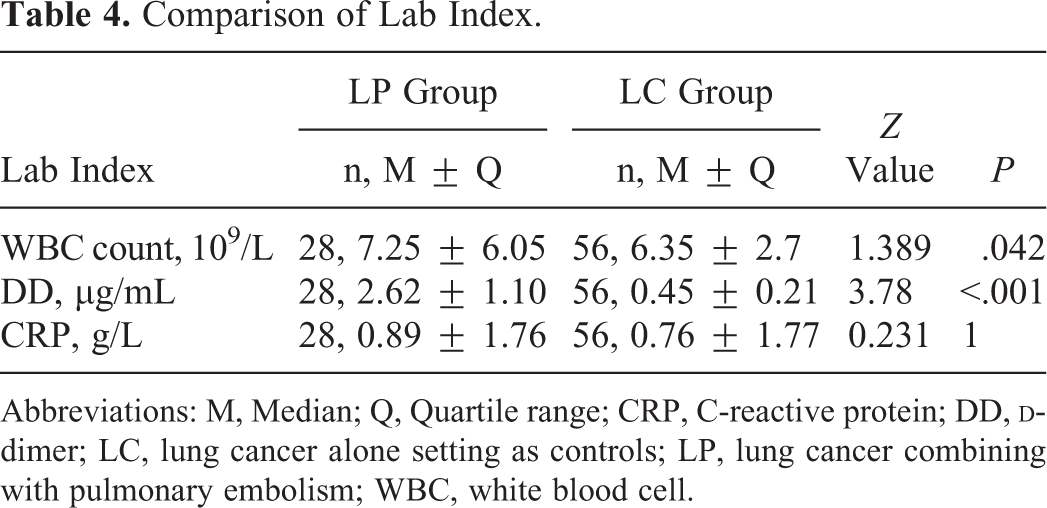
Abbreviations: M, Median; Q, Quartile range; CRP, C-reactive protein; DD,
Logistic regression analysis data of lung cancer patients complicated with PE

Abbreviations: ALB, albumin; CI, confidence interval; DD,
Confirmed Diagnosis Time of PE and Lung Cancer
In 27 patients of the LP group, PE occurred after the diagnosis of lung cancer (the longest interval was 46 months), while only 1 patient developed PE before the diagnosis of lung carcinoma. Median survival duration of those in the SPE subgroup was 3.6 months (95% confidence interval [CI], 3.2-4.0), while that in the APE subgroup was 10.5 months (95% CI, 8.88-12.12). There was no significant difference in the median survival time between these 2 subgroups.
Survival Analysis Between the LP and LC Groups
According to Kaplan-Meier analysis of survival period of the LP and LC groups, the median survival duration of the APE subgroup was 7.2 months (95% CI, 5.86-8.56) and that of the SPE subgroup was 2.8 months (95% CI, 2.48-3.12). Log-rank analysis examined the survival rate of these 2 subgroups, and it was found that the survival time of the SPE subgroup was obviously lower than that of the APE subgroup (P < .01; Figure 2).
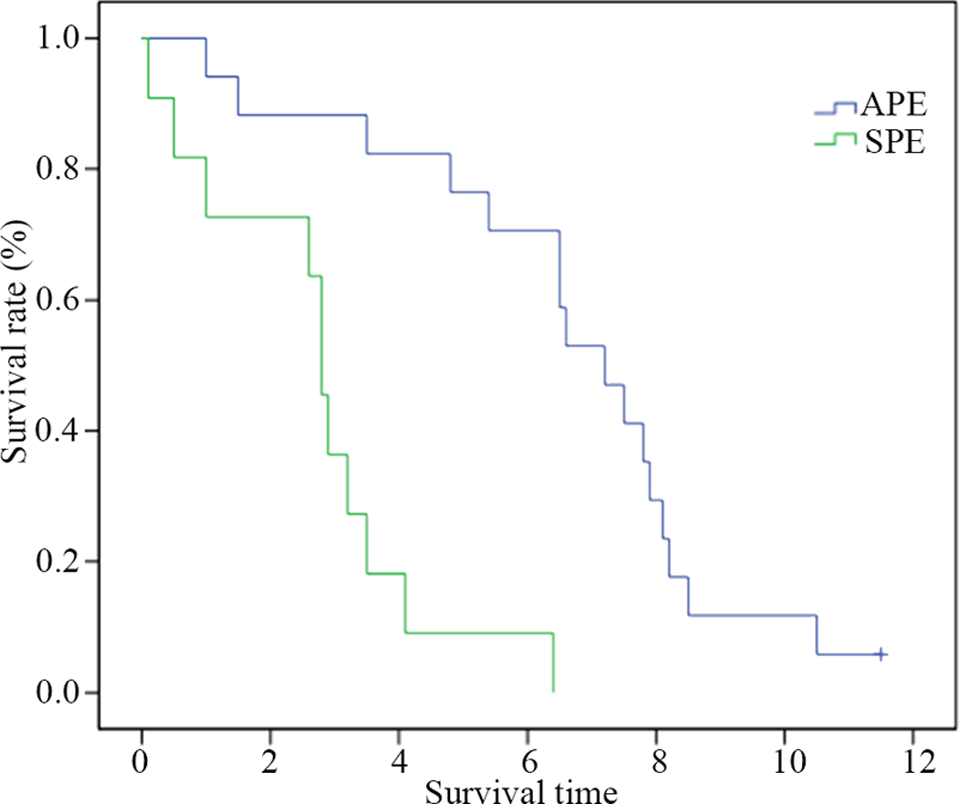
Prognosis of APE subgroup and SPE subgroup. Median survival duration of APE subgroup was 7.2 months (95% CI, 5.86-8.56); median survival duration of SPE subgroup was 2.8 months (95% CI, 2.48-3.12). Log-rank analysis was used to examine the survival rate of these 2 subgroups. APE indicates asymptomatic pulmonary embolism; CI, confidence interval; SPE, symptomatic pulmonary embolism.
Treatment and Prognosis
Twenty-seven patients in the LP group were given low-molecular-weight heparin and warfarin sequential anticoagulant therapy and 1 patient was given urokinase thrombolysis. After treatment, 1 death was reported in high-risk patients, 3 deaths in medium/low-risk patients, and 2 ceased anticoagulant therapy due to hemoptysis, while the other cases showed improvement or got cured (78.6%). (Criteria for healing and improvement: PE at same location disappeared after anticoagulant therapy inspected by spiral CT pulmonary arteriography.)
Discussion
Pulmonary embolism was the most common complication of unfavorable prognosis in tumor disease progression and antitumor treatment. Lung cancer complicated with PE increased the treatment difficulty, reducing the living quality, and shortening the survival time of patients. 6 A retrospective study showed that PE was 3.3% as assessed by chest CT in 435 patients with cancer. 7 In 1982, Williams et al found that SPE was 27% in 158 patients who underwent extremity and hip surgery. 8 A recent meta-analysis of CT scanning of 10 000 patients with cancer found a PE occurrence of 2% of >5 mm thickness (95% CI, 1.0-3.4), compared with 3% of <5 mm thickness (95% CI, 2.0-4.0). 9 Several studies found a high risk of unfavorable prognosis in patients with APE. The sudden death risk upregulated (odds ratio [OR] 1.79; 95% CI, 1.10-2.90) when anticoagulant therapy was not applied and resulted in a short survival duration. 10 In the present study, the occurrence rate of PE in patients with lung cancer was 4.1% with a large proportion of APE, which led to misdiagnosis and delayed treatment. Hence, the early detection, treatment, and imaging manifestation of lung cancer complicated with PE are most essential for the diagnosis and prognosis of patients.
In the present study, we found that the lung cancer complicated with PE was common in patients with adenocarcinoma and stage III and IV tumor; and hyperleukocytosis, DD increment, and hypoalbuminemia are the risk factors for this disease. In 17 patients of the LP group, it has been reported that the lung adenocarcinoma increased PE occurrence. Geerts et al found that adenocarcinoma cells secreted mucin to activate the thrombogenic mediator, followed by the allergic reaction, the regression of endangium and surrounding tissue, fibrinoid degeneration, and epithelial cell exfoliation, and finally leading to thrombogenesis; meanwhile, mucin directly activated blood platelets to cause blood coagulation, consequently resulting in Trousseau syndrome. 11 It has also been reported that tumor staging is highly relevant to VTE occurrence.
Venous thromboembolism, comprising PE, deep vein thrombosis, and thrombotic shallow phlebitis , is the most common complication in tumor disease progression and antitumor treatment and is also the second major cause of death in patients with tumor, especially PE which is common in lung cancer. Lung cancer complicated with PE resulted in increased treatment difficulty, reducing the living quality, and shortening the survival time of patients. In several cases, lung cancer complicated with PE did not show a typical clinical manifestation different from lung cancer symptom. In other conditions, PE was the principal manifestation of lung carcinoma.
It has been reported that the occurrence rate of VTE was 5.3% in 1921 patients receiving chemotherapy, while one-third of patients had PE complication.
12
It has also been reported that tumor staging is highly relevant to the VTE occurrence.
13,14
The PE occurrence increased in advanced lung cancer, which was related to high expression of procoagulant, thrombin, and cytokines and the hypercoagulable state caused by tumor metastasis.
15
In the present study, secondary PE risk in patients with lung cancer having hyperleukocytosis was doubly higher than that in other patients; this can be attributed to tissue factor and vascular endothelial growth factor secreted by platelet and vascular endothelial cells which were activated by leukocyte to promote thrombogenesis.
16
Previous study has showed that Hb concentration higher than 140 g/L was the risk factor for lung cancer complicated with PE, and anemia in patients with lung cancer reached up to 77%.
17
In the present study, we found that there was significant difference in Hb concentration (<100 g/L) between the LP and LC groups; however, the multifactor regression analysis showed that the P value was higher than .05, suggesting the role of Hb concentration as the risk factor for PE occurrence. This needs to be further investigated.
Cough, expectoration, stethalgia, and chest distress were the common clinical presentation in patients with lung cancer. In our study, the clinical symptoms of the LP group did not show any specificity of the LC group; among them, the primary uniformity of 17 patients diagnosed with PE did not aggravate, while that of the other 11 patients diagnosed with PE showed symptom aggravation, indicating there was no specific symptoms in lung cancer complicated with PE.
In the present study, 22 patients with lung cancer complicated with PE had been treated with platinum-based chemotherapy drugs, 6 cases treated with gemcitabine chemotherapy, 16 cases treated with pemetrexed disodium, and 2 cases treated with Tyrosine Kinase Inhibitors (TKI) targeted drug. We found that the risk of lung cancer complicated with PE in patients treated with systemic chemotherapy was 5.35 times higher than other patients, which is consistent with the previous report on the risk of thrombus enhanced by systemic chemotherapy. The reasons might be the activation of coagulation system in vivo by tissue factor releasing through traditional chemotherapy drug treatment, while novel molecular-targeted drug directly activated the platelet coagulation pathway. 19 Chemotherapy altered coagulation factor and natural anticoagulant level to downregulate the endogenous anticoagulant level and reduce the fibrinolytic activity, thereby promoting the VTE occurrence through the endotheliocyte damage. 3,4 A research in the large-scale population demonstrated that the relative risk of thrombus increased in patients receiving chemotherapy (OR = 9.90; 95% CI, 3.89-25.18), while the OR value of thrombus in other patients was 6.90 (95% CI, 3.92-12.17), 20 indicating that thrombus was related to chemotherapy treatment.
A number of research have shown that 1 year after diagnosis of lung cancer was the high-risk period of developing VTE complication (mean value, 185 days). 3,11 In our study, the mean duration from lung cancer diagnosis to PE development was 3.6 months (95% CI, 3.2-4.0) in 17 patients of the APE subgroups, while that of 11 cases in the SPE subgroups was 10.5 months (95% CI, 8.88-12.12), showing a significant difference between these 2 subgroups (P < .01).
Low-molecular-weight heparin and warfarin sequential anticoagulant therapies were administered for patients with lung cancer complicated with PE. The median survival time of the APE subgroup was 7.2 months (95% CI, 5.86-8.56), while that of the SPE subgroup was 2.8 months (95% CI, 2.48-3.12), showing obvious difference in both groups which was consistent with previous reports. 21
We found a high PE incidence in patients with lung cancer, and most of these patients did not show any specific clinical characteristic. Advanced adenocarcinoma, systemic chemotherapy, hyperleukocytosis, and DD increment were the risk factors for lung cancer complicated with PE. The present study indicated that (1) high risk of embolism in patients with lung cancer should be evaluated, and anticoagulant therapy could be administered to avoid PE occurrence; (2) early screening for PE should be performed in patients with lung cancer for diagnosis of PE and anticoagulant therapy; (3) the early detection of PE and timely anticoagulation symptomatic treatment helps in improving the clinical symptoms and survival time.
Conclusion
In this study, we found that lung adenocarcinoma, chemotherapy, hyperleukocytosis, and DD increment were the risk factors for lung cancer combined with PE, and PE in lung cancer was frequently asymptomatic. Comparing with those SPE cases, APE cases has earlier high incidence time and showed better prognosis. Our findings might help early detection of PE and timely anticoagulation symptomatic treatment, improving clinical symptoms and survival time.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.