
Abstract
Colorectal cancer is one of the most frequent causes of cancer-related deaths worldwide. Thus, there is a need for timely diagnosis and effective treatment. Our aim in the present study was to detect the serum level of trefoil factor 3 protein and evaluate the diagnostic accuracy of trefoil factor 3 in patients with colorectal cancer. We collected serum samples from 204 participants (127 patients with colorectal cancer, 35 patients with polyps, and 42 healthy controls). The levels of serum trefoil factor 3 and carcinoembryonic antigen expression were measured by enzyme-linked immunosorbent assay. Receiver operating characteristic curves were plotted to calculate the diagnostic accuracy of trefoil factor 3 in patients with colorectal cancer. The serum levels of trefoil factor 3 in patients with colorectal cancer (6.66 ± 2.4 ng/mL; P < .00l) and polyps (3.86 ± 1.3 ng/mL; P < .00l) were significantly increased compared to healthy controls (2.09 ± 1.0 ng/mL). Moreover, the area under the receiver operating characteristic curve for trefoil factor 3 was greater than carcinoembryonic antigen (0.889 vs 0.715). At a cutoff value of 5.591 ng/mL, the diagnostic sensitivity, specificity, and likelihood ratio of serum trefoil factor 3 for colorectal cancer was 74.2%, 94.8%, and 14.25, respectively. Furthermore, the serum trefoil factor 3 levels in early colorectal cancer (TNM stage I, 3.67 ± 1.27 ng/mL) were significantly increased compared to healthy controls (P < .001); however, there was no significant difference compared to patients with polyps (P = .576). We observed that the serum trefoil factor 3 levels decreased after surgery (6.66 ± 2.4 vs 4.48 ± 1.80 ng/mL; P < .001). In addition, high serum trefoil factor 3 levels were associated with poor tumor differentiation and clinical TNM stage (P < .05). In conclusion, serum trefoil factor 3 is a promising biomarker for the diagnosis of colorectal cancer and prognosis of patients.
Introduction
Colorectal cancer (CRC) is the fifth most frequent cause of cancer-related deaths in China. 1,2 Due to the lack of an effective method for timely diagnosis, most patients are detected at an advanced stage and have corresponding poor outcomes. At present, several screening methods, such as colonoscopy, fecal occult blood testing (FOBT), and serum biomarkers, are recommended for the detection of CRC. Limited by the cost and unpleasant perception, widespread colonoscopy screening is currently unavailable, and the sensitivity and specificity are unsatisfactory for FOBT and some biomarkers. 3 Therefore, the search for noninvasive, hypersensitive biomarkers has intensified. At present, carcinoembryonic antigen (CEA) is the most commonly used serum biomarker for CRC in clinical practice; however, recent studies have shown the sensitivity of CEA to be as low as 30% to 40% for early CRC. 4,5 Indeed, patient outcome and the survival and mortality rates directly depend on the timely and effective diagnosis of CRC. Therefore, novel and reliable serum biomarkers are needed to improve the diagnostic accuracy for CRC.
Trefoil factor 3 (TFF3) belongs to the TFF family, which consists of 3 stable secretory proteins that are expressed together with mucins from epithelial cells of the gastrointestinal tract. 6 Trefoil factor 1 is normally expressed in the gastroduodenal mucosa, whereas TFF2 is predominantly expressed in mucous neck cells in the body and antral glands of the stomach. 7 Trefoil factor 3 is expressed in goblet cells of the intestine and at lower levels in other organs, such as the breast, salivary glands, respiratory tract, and hypothalamus. 8 –12 Trefoil factor proteins have been shown to play an important role in promoting epithelial restitution after injury and discontinuity of the mucosal surface leads to a local increase in TFF expression. Recently, cumulative research indicates that TFF3 might also promote the invasion of tumor cells by acting directly on malignant cells and indirectly on the vasculature. Several studies have reported that serum levels of TFF are significantly increased in patients with cancer (mainly gastric cancer) and thus serve as a potential biomarker for cancer screening. 13 –16
Therefore, we conducted this study to determine the serum levels of TFF3 in patients with CRC and assess the diagnostic accuracy of serum TFF3. The diagnostic accuracy was further analyzed in comparison with the serum CEA level. Additionally, the correlation between the serum TFF3 level and clinical characteristics of patients with CRC was analyzed.
Materials and Methods
Participants
One hundred twenty-seven patients with CRC who underwent surgery between January 2011 and June 2014 were enrolled in this study, which was conducted in the Department of Surgery at the The First Affiliated Hospital of Sun Yat-sen University (Guangzhou, Guangdong). Forty-two patients who were considered to be healthy (without signs of disease or polyps) and 35 patients with polyps were also recruited. The polyps were diagnosed by pathohistologic evaluation of colonoscopic biopsy specimens. The diagnosis of CRC was confirmed pathologically, and there was no history of other tumors. No patients received preoperative treatment, such as radiotherapy or chemotherapy. The TNM stage of tumors and the histologic type were defined according to the American Joint Committee on Cancer and Union for International Cancer Control. Early CRC was defined as TNM stage I, and 26 patients were classified as early CRC. This study was approved by the Ethics Committee of The First Affiliated Hospital of Guangzhou Command, and written consent was obtained from all patients when recruited. All serum samples were collected in serum separator tubes at the time of initial presentation before treatment. The blood samples were allowed to clot for 30 minutes at room temperature then centrifuged for 15 minutes at 1000g. Serum samples were stored at −80°C until testing.
Enzyme-linked immunosorbent assay
Serum TFF3 levels were detected using commercially available enzyme-linked immunosorbent assay (ELISA) kits (SEB656Hu22; USCN Life Science, Wuhan, China) according to the manufacturer’s instructions. Briefly, purified monoclonal antibody to TFF3 was precoated onto 96-well microtiter plates. Then, 100 mL serum samples, dilutions of the appropriate human TFF3 standard, and controls were added to the respective wells, and the plates were incubated for 2 hours at 37°C. The plates were washed before diluted biotin-labeled TFF3 detection antibody was added to each well. After another 1-hour incubation at 37°C, the plates were washed, and diluted streptavidin conjugated to horseradish peroxidase was added to each well. Following a 30-minute incubation at 37°C, the plates were washed, and tetramethyl benzidine solution was added for a 20-minute incubation at 37°C. Then, 50 mL of stop solution was added to each well. Finally, the absorbance at 450 nm was measured. The concentration of human TFF3 in the samples was then calculated according to the working standard curve. All measurements were performed in duplicate. The assay sensitivity for TFF3 was 28.4 pg/mL. The intra-assay coefficient of variation (CV) and inter-assay CV were <8% and 10%, respectively. Serum CEA levels were measured using a commercially available ELISA kit (SEA150Hu; USCN Life Science).
Statistical Analysis
Statistical analysis was performed with SPSS version 19.9 (SPSS, Inc; Chicago, Illinois) and GraphPad Prism 5.01 (La Jolla, California). The results are expressed as the mean ± standard error of the mean or median for nonparametric data. Differences between 2 independent groups were tested by t tests for normal distributions or the Mann-Whitney U test for nonnormal distributions. Receiver operating characteristic (ROC) curves and the area under the curve (AUC) with 95% confidence intervals (CIs) were constructed to assess the diagnostic accuracy of each parameter, and the optimum cutoff value was selected according to the ROC curve. The correlation between the serum TFF3 concentration and clinical characteristics was analyzed with a Pearson’s χ2 test or Fisher exact test. A 2-sided P value <.05 was considered statistically significant.
Results
Baseline Characteristics of Patients and Controls
One hundred twenty-seven patients with CRC (male to female ratio, 58:69; mean age ± standard deviation [SD], 65.6 ± 17.2 years), 35 patients with polyps (male to female ratio, 23:12; mean age ± SD, 61.5 ± 18.6 years), and 42 healthy controls (male to female ratio, 17:25; mean age ± SD, 59.8 ± 14.8 years) were enrolled in the study. In the CRC group, 26 (20.5%) patients had early-stage CRC (TNM stage I), whereas 101 (79.5%) patients had advanced gastric cancer. The mean tumor size was 3.9 ± 1.7 cm. Of the CRC specimens, 22.8% (29/127) were well differentiated, and 43.3% (55/127) and 33.9% (43/127) were moderately and poorly differentiated, respectively.
Serum TFF3 Level in Patients With CRC Versus Controls
As shown in Figure 1, the serum levels of TFF3 in patients with CRC (6.66 ± 2.4 ng/mL; P < .00l) and polyps (3.86 ± 1.3 ng/mL; P < .00l) were significantly increased compared to healthy controls (2.09 ± 1.0 ng/mL). The serum TFF3 level in patients with CRC was significantly higher than that in patients with polyps (P < .00l). Furthermore, the serum TFF3 level in patients with early CRC (TNM stage I, 3.67 ± 1.27 ng/mL) was also significantly increased compared to healthy controls (Figure 1A; P < .001) but not significantly different compared to patients with polyps (Figure 1A; P = .576). Additionally, the serum TFF3 level was decreased after surgery (Figure 1B; 6.66 ± 2.4 vs 4.48 ± 1.80 ng/mL; P < .001).

Comparative analysis of serum TFF3 levels in patients with CRC and controls. A, The level of TFF3 expression in patients with CRC and polyps and healthy controls. The level of serum TFF3 expression on average was upregulated in patients with CRC compared with the patients with polyps and healthy controls (P < .001). The serum TFF3 level in patients with early CRC (TNM stage I) was significantly increased compared to healthy controls; however, there was no significant difference compared with patients with polyps (P ≥ .05). B, Changes in serum TFF3 levels before and after surgery. The expression of serum TFF3 was decreased after surgery (P < .001). C, The levels of TFF3 expression in patients with early CRC (TNM stage I) were increased compared to healthy controls (P < .001); however, there was no significant difference compared with patients with polyps (P ≥ .05). *P < .001 compared with control; **P > .05; CRC indicates colorectal cancer; HC, healthy control; TFF3, trefoil factor 3.
The serum levels of CEA in patients with CRC and polyps, and the healthy controls, are shown in Figure 1C. The serum CEA level in patients with CRC (252.63 ± 101.5 μg/L) was significantly increased compared to healthy controls (72.51 ± 38.7 μg/L, P < .001); however, there was no significant difference between the CEA levels in patients with polyps (113.36 ± 77.3 μg/L) and healthy controls (P = .056).
Diagnostic Accuracy of TFF3 for Patients With CRC
The ROC analysis was performed to calculate the diagnostic accuracy of serum levels of TFF3 and CEA for patients with CRC. Trefoil factor 3 was shown to be a promising serum marker to discriminate patients with CRC from patients with polyps and healthy controls, with an AUC of 0.889 (95% CI: 0.846-0.933; P < .001; Figure 2). At an optimal cutoff value of 5.591 ng/mL, the sensitivity, specificity, and likelihood ratio (LR) were 74.2%, 94.8%, and 14.25, respectively. The AUC for CEA was 0.715 (95% CI: 0.643-0.787), with an optimal sensitivity, specificity, and LR of 62.2%, 72.7%, and 2.28, respectively (Table 1 and Figure 2). Together, ROC analysis suggested that TFF3 has a higher diagnostic accuracy than CEA.
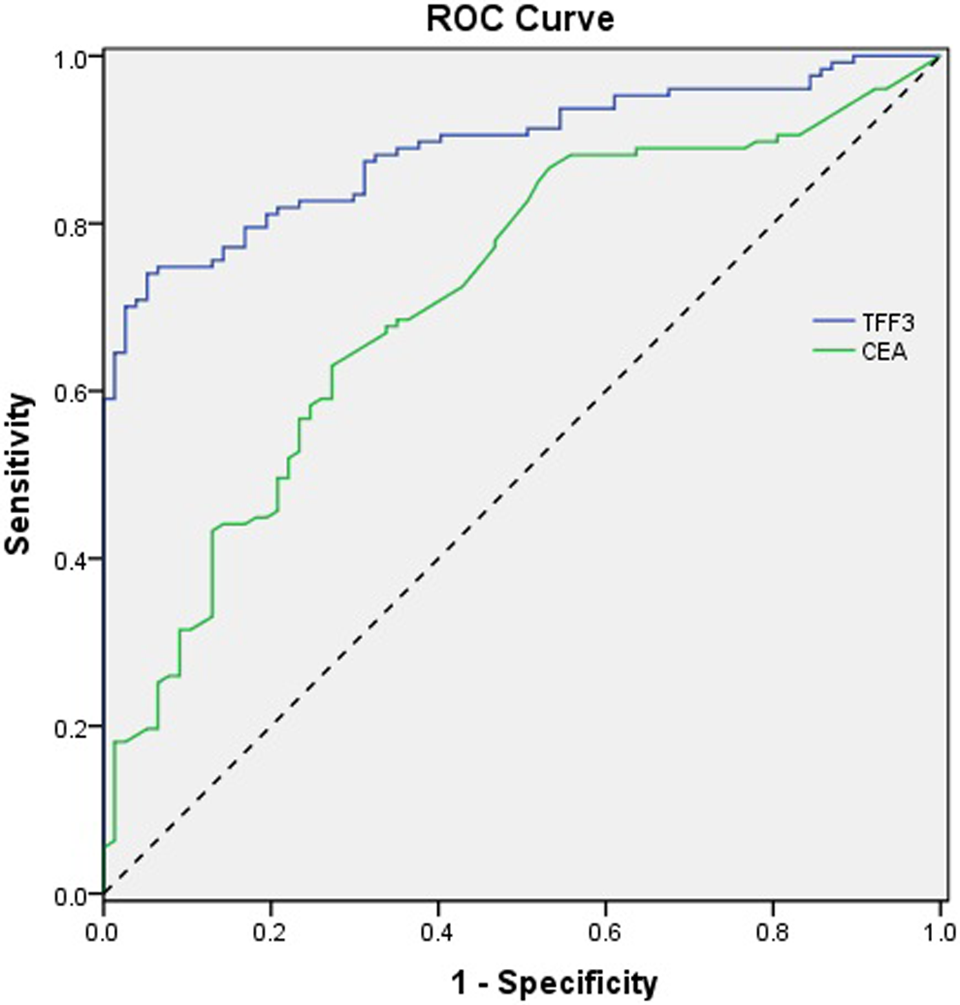
Receiver operating characteristic (ROC) curves for TFF3 and CEA. The area under the curve (AUC) of serum TFF3 and CEA was 0.889 (95% CI: 0.846-0.933) and 0.715 (95% CI: 0.643-0.787). The results showed that serum TFF3 has a greater predictive power for CRC than CEA. CEA indicates carcinoembryonic antigen; CI, confidence interval; CRC, colorectal cancer; TFF3, trefoil factor 3.
Diagnostic Accuracy (Sensitivity, Specificity, Likelihood Ratio [LR], and AUC) of Serum TFF3 and CEA.

Abbreviations: AUC, area under the curve; CEA, carcinoembryonic antigen; CI, confidence interval; TFF3, trefoil factor 3.
Relationship Between Serum TFF3 Level and Clinical Characteristics of Patients With CRC
To determine the association between serum TFF3 levels and clinical features, all patients with CRC were divided into 2 groups based on the cutoff value. Accordingly, there were 53 and 74 patients in the high- and low-expression groups, respectively. The correlations between the 2 groups and clinical features are shown in Table 1. No significant correlation was observed between the serum TFF3 level and patient age, gender, tumor size, tumor type, tumor location, lymph node metastases, and distant metastases (P > .05; Table 1); however, we found that a high level of serum TFF3 expression was significantly associated with poor tumor differentiation and clinical TNM stage (P < .05; Table 2). We were unable to demonstrate a similar association with CEA.
Correlation Between Serum TFF3 Levels and Clinical Characteristics of Patients With CRC.

Abbreviations: CRC, colorectal cancer; TFF3, trefoil factor 3.
Discussion
At present, several screening methods are used to screen for CRC; however, a sizeable number of patients with CRC are diagnosed at an advanced stage of the disease and have a poor outcome. Recently, several molecules have been investigated for the diagnosis of CRC. Unfortunately, there was still some limitations in clinical practice due to an inefficiency in the early detection of CRC. 17,18 Carcinoembryonic antigen is the most commonly used tumor marker for the detection of CRC; however, recent studies have indicated a poor diagnostic value of CEA due to its poor sensitivity and specificity. 19,20 Similarly, in the current study, the sensitivity and specificity of CEA for CRC were 62.2% and 72.7%, respectively; this finding is in agreement with previous studies. Therefore, novel and reliable biomarkers are needed for CRC screening.
Trefoil factor proteins have been reported to play a role in cell proliferation, apoptosis, migration, invasion, and angiogenesis. In addition, serum TFF levels have been observed to be elevated in patients with cancer and could thus serve as potential biomarkers. Previously, Kaise et al 21 reported that serum TFF3 is a promising marker for the diagnosis of gastric cancer; however, the diagnostic value of serum TFF3 in patients with CRC has not been fully evaluated.
In the current study, we showed that the serum TFF3 levels in patients with CRC are significantly higher than in patients with polyps and healthy controls. The ROC curve analysis further suggested that TFF3 is a useful marker for the diagnosis of CRC, with an AUC of 0.889 (95% CI: 0.846-0.993; P < .001; Figure 2), which was higher than that for CEA (AUC = 0.715). At an optimal cutoff value of 5.591 ng/mL, the sensitivity, specificity, and LR of serum TFF3 for patients with CRC were 74.2%, 94.8%, and 14.25, respectively. In addition, the sensitivity and specificity of TFF3 were higher in patients with CEA (74.2% vs 62.2% and 94.8% vs 72.7%, respectively). All of these results suggested that serum TFF3 might be a more promising biomarker for the diagnosis of CRC than CEA. In addition, we found that the serum TFF3 levels in patients with early CRC (TNM stage I, 3.67 ± 1.27 ng/mL) were significantly increased compared to healthy controls (P < .001); however, there was no significant difference compared with patients who had polyps (P = .576). Therefore, the serum TFF3 might be not a good biomarker for the early detection of CRC.
The striking decrease in the serum TFF3 level after surgery suggests that TFF3 can serve as a potential surveillance biomarker to assess the therapeutic response for patients with CRC. Additionally, we found that a high level of serum TFF3 expression is associated with poor tumor differentiation and clinical TNM stage; however, no significant relationship was found between the serum TFF3 level and patient age, gender, tumor size, tumor type, tumor location, lymph node metastases, and distant metastases. We also failed to find a significant correlation between the serum CEA level and clinical features. To further explore the potential role of TFF3 in prognosis of patients with CRC, we are undertaking a long-term follow-up of the current study in patients with CRC who have undergone surgery.
There were some limitations in our study, such as the small study size, single-center study design, and patient selection bias. We recruited all participants from a clinical series of hospital-based cases together with healthy people from the health center rather than a population-based cohort, which could represent a risk of bias in patient selection. Therefore, more population-based studies, large-scale, or multicenter validation studies are needed to determine the diagnostic value of serum TFF3 in patients with CRC.
Conclusion
To summarize, serum TFF3 may serve as a new promising tumor biomarker for the diagnosis of CRC and prognosis, but TFF3 is not a good biomarker for the early detection of CRC. Moreover, large-scale studies are warranted to investigate the diagnostic and prognostic value of the serum TFF3 level for patients with CRC.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.