
Abstract
Objective:
Radiation treatment planning for locally advanced lung cancer can be technically challenging, as delivery of ≥60 Gy to large volumes with concurrent chemotherapy is often associated with significant risk of normal tissue toxicity. We clinically implemented a novel hybrid RapidArc technique in patients with lung cancer and compared these plans with 3-dimensional conformal radiotherapy and RapidArc-only plans.
Materials/Methods:
Hybrid RapidArc was used to treat 11 patients with locally advanced lung cancer having bulky mediastinal adenopathy. All 11 patients received concurrent chemotherapy. All underwent a 4-dimensional computed tomography planning scan. Hybrid RapidArc plans concurrently combined static (60%) and RapidArc (40%) beams. All cases were replanned using 3- to 5-field 3-dimensional conformal radiotherapy and RapidArc technique as controls.
Results:
Significant reductions in dose were observed in hybrid RapidArc plans compared to 3-dimensional conformal radiotherapy plans for total lung V20 and mean (−2% and −0.6 Gy); contralateral lung mean (−2.92 Gy); and esophagus V60 and mean (−16.0% and −2.2 Gy; all P < .05). Contralateral lung doses were significantly lower for hybrid RapidArc plans compared to RapidArc-only plans (all P < .05). Compared to 3-dimensional conformal radiotherapy, heart V60 and mean dose were significantly improved with hybrid RapidArc (3% vs 5%, P = .04 and 16.32 Gy vs 16.65 Gy, P = .03). However, heart V40 and V45 and maximum spinal cord dose were significantly lower with RapidArc plans compared to hybrid RapidArc plans. Conformity and homogeneity were significantly better with hybrid RapidArc plans compared to 3-dimensional conformal radiotherapy plans (P < .05). Treatment was well tolerated, with no grade 3+ toxicities.
Conclusion:
To our knowledge, this is the first report on the clinical application of hybrid RapidArc in patients with locally advanced lung cancer. Hybrid RapidArc permitted safe delivery of 60 to 66 Gy to large lung tumors with concurrent chemotherapy and demonstrated advantages for reduction in low-dose lung volumes, esophageal dose, and mean heart dose.
Keywords
Introduction
Radiation treatment planning for locally advanced lung cancer can be technically challenging, as delivery of doses of ≥60 Gy to large volumes with concurrent chemotherapy is often associated with significant risk of normal tissue toxicities. 1 –3 Three-dimensional conformal radiotherapy (3D-CRT), intensity-modulated radiotherapy (IMRT), and volumetric-modulated arc therapy (VMAT) have been used to treat locally advanced lung cancer. The advantage of IMRT over 3D-CRT is improved target conformity and sparing of organs at risk (OARs). 4 RapidArc (RA; Varian Medical Systems, Palo Alto, California) is a form of VMAT in which intensity-modulated radiation beam arcs are delivered to the target, coordinated with changes in gantry speed, multileaf collimation (MLC) shape, and dose rate. 5,6 Compared to IMRT, RA has decreased treatment time and further improved conformity of high dose and sparing of OARs. 4
For treatments of lung cancers, limiting dose to the esophagus and normal lung can significantly reduce treatment-related morbidity. A predictor of esophagitis is the V60 (the esophageal volume receiving at least 60 Gy), 7 which can be decreased with the higher conformality achievable with VMAT. However, a potential cost of VMAT and IMRT is widely distributed low-dose levels in tissues surrounding the target such as the normal lung. Studies have shown an increased risk of radiation pneumonitis with a lung V5 >60% (volume of lung receiving at least 5 Gy is more than 60%). 8 –10
Hybrid RapidArc (H-RA) is a novel technique in which the majority of dose to the target is delivered with traditional, static 3D-CRT fields and the remainder with VMAT fields. 1 –4,11 An advantage of H-RA over conventional IMRT and 3D-CRT is the delivery of high dose to the target, while reducing low dose to the surrounding normal tissue. 2 Also, with IMRT, the MLC leaves move during the delivery of dose. Although beam gating techniques are generally used to account for tumor motion in the lung, the rotating gantry, moving MLC leaves, changing dose rate, and respiratory motion may result in a distribution of dose that was not predicted in the treatment plan. 12,13 With an IMRT contribution of only about 40% of the total dose, the uncertainties in dose distribution will be reduced.
Several planning studies have reported improved distribution of dose using H-RA. 1 –4,11 However, to date, this is not common practice, and, to our knowledge, no studies have reported clinical outcomes of patients with locally advanced lung cancer treated with H-RA. In our study, we present the dosimetry and clinical outcomes of patients with locally advanced lung cancer treated with this technique.
Methods
Patient Characteristics
Hybrid RapidArc was used to treat 11 patients with locally advanced lung cancer having bulky mediastinal adenopathy (stage III disease). Seven of the 11 patients were men. Median age at the start of H-RA was 64 years, with a range from 44 years to 83 years. All 11 patients received concurrent chemotherapy. Patient demographics, tumor characteristics, radiation doses, and chemotherapy treatments are listed in Table 1. For our patient cohort, overall survival was assessed from the start date of H-RA. Toxicity was collected retrospectively from physician notes. Treatment-associated toxicities were assessed using the Common Terminology Criteria for Adverse Events version 4.03 published by the US National Cancer Institute.
Patient Demographics, Tumor Characteristics, and Treatment Regimen.

Abbreviation: F, female; M, male.
Dosimetry
All patients underwent a 4-dimensional computed tomography (4D-CT) planning scan in preparation for radiation planning. A board-certified radiation oncologist contoured the gross tumor volume (GTV) on the planning CT scan. A clinical target volume (CTV) was contoured around the GTV to include areas at risk for microscopic disease. A free-breathing 4D-CT scan and Real-time Position Management system (Varian Medical Systems) were used to measure tumor motion. For this cohort of patients with large mediastinal tumors and compromised lung function, the clinical decision was made to not restrict breathing motion with any motion management devices due to concern for reproducibility and patient tolerance. The maximum intensity projection generated from the 4D-CT was used to contour an internal target volume (ITV). The ITV accounts for any movement of the CTV during treatment. A margin was added to the ITV to create a planning target volume (PTV), which compensates for any setup uncertainties. A certified medical dosimetrist generated the radiation plans, which were approved by the radiation oncologist. All patients were treated with H-RA plans. Three-dimensional conformal radiotherapy and RA plans were retrospectively generated and compared to H-RA plans. Figure 1 shows typical beam arrangements for standard 3D-CRT and H-RA plans. Lateral avoidance sectors were used to limit dose to lung in RA plans. All plans were normalized with a minimum PTV coverage of V95% > 95% (at least 95% of the PTV receives more than 95% of the prescription dose). Hybrid RapidArc plans concurrently combined static (60%) and RA (40%) beams. All cases were replanned using 3- to 5-field 3D-CRT-only technique for comparison. Because the treated volumes were larger than those treated with stereotactic radiosurgery or stereotactic body radiation therapy, additional fields were not used for 3D-CRT in order to limit low dose to the surrounding OARs. The conformity index (CI) was defined as the ratio of the prescription isodose volume to the target volume. 14 The homogeneity index (HI) was defined by the following equation: (D2% − D98%)/D50%, where D2% was the cutoff dose of the maximum 2% and D98% was the cutoff dose of the minimum 2% of dose within the target volume. D50% was the mean target dose within the target volume.

A, Typical beam arrangement for a 3-dimensional conformal radiotherapy (3D-CRT) plan. B, Typical beam arrangement for a hybrid RapidArc (H-RA) plan.
Statistics
IBM SPSS Statistics 23 software was used for statistical analysis. Student t test was used for comparing differences at a .05 significance level.
Results
The average ITV was 195 cm3. A mean margin of 0.62 cm around the ITV was used to create the PTV, and the mean PTV was 513 cm3 (range, 213-952 cm3). Hybrid RapidArc plans spared significantly more total and contralateral lung volume than 3D-CRT plans. Total and contralateral lung mean doses were 17.85 Gy and 6.43 Gy, respectively, for H-RA plans and 18.45 Gy and 9.35 Gy, respectively, for 3D-CRT plans (P < .05). The median V20 to the total and contralateral lung was 29% and 5%, respectively, for H-RA plans and 31% and 8%, respectively, for 3D-CRT plans (P < .05). Esophagus mean dose and median esophageal V60 were also significantly lower with H-RA. Esophageal mean dose was 2.2 Gy lower with H-RA compared to 3D-CRT (P < .01). Esophagus V60 was 16% lower with H-RA versus 3D-CRT (P = .03). The 3D-CRT plans treated larger extra areas to prescription dose levels (mean CI: 1.81 vs 1.25, P < .01). The heart V60 was significantly lower for H-RA plans (3% vs 5%, P = .04). Mean heart dose was also significantly better for H-RA plans compared to 3D-CRT plans (16.32 Gy vs 16.65 Gy, P = .03). A comparison of the isodoses for a 3D-CRT plan and an H-RA plan is shown in Figure 2. Hybrid RapidArc produced significantly improved dose homogeneity, as reflected in lower HI (9.4% vs 13.6%, P = .02).

Isodoses in a sample patient. A 3-dimensional conformal radiotherapy (3D-CRT) plan is shown on the left, and a hybrid RapidArc (H-RA) plan is shown on the right. Blue shades represent low doses (5-20 Gy).
Hybrid RapidArc plans were also compared to RA-only plans. Dose homogeneity and all measured dose parameters to the contralateral lung were significantly improved with H-RA compared to RA-only plans. The HI was significantly lower in the H-RA plans versus the RA plans (9.4% vs 11.5%, P < .01). Although the contralateral lung V5 trended toward significant improvement with the H-RA plans compared to the 3D-CRT plans (P = .07), it was significantly improved with H-RA plans compared to RA plans (37% vs 45%, P < .01). There was no significant difference between H-RA and RA in CI, total lung doses, esophageal doses, mean heart dose, or heart V60. However, heart V40 and V45 and maximum spinal cord dose were significantly lower for RA plans compared to H-RA plans. A comparison of the CIs, HIs, and doses to OARs for 3D-CRT, RA, and H-RA plans is shown in Table 2.
Dosimetric Comparisons for 3D-CRT and H-RA Plans.
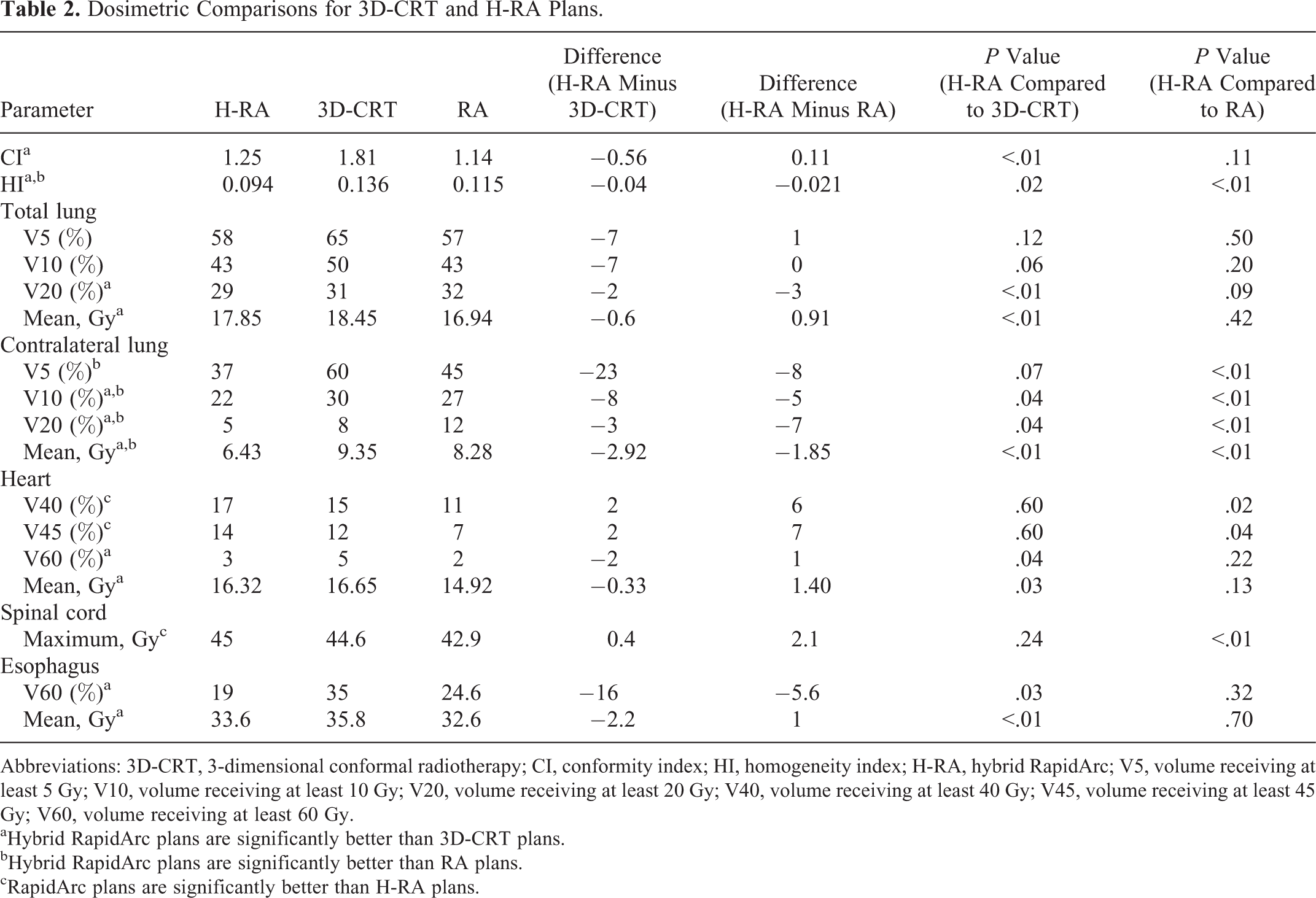
Abbreviations: 3D-CRT, 3-dimensional conformal radiotherapy; CI, conformity index; HI, homogeneity index; H-RA, hybrid RapidArc; V5, volume receiving at least 5 Gy; V10, volume receiving at least 10 Gy; V20, volume receiving at least 20 Gy; V40, volume receiving at least 40 Gy; V45, volume receiving at least 45 Gy; V60, volume receiving at least 60 Gy.
aHybrid RapidArc plans are significantly better than 3D-CRT plans.
bHybrid RapidArc plans are significantly better than RA plans.
cRapidArc plans are significantly better than H-RA plans.
Median follow-up time was 17.1 months. All patients completed RT as planned. Treatment was well tolerated in all 11 patients, with no grade 3+ toxicities. No patient required a feeding tube or developed symptomatic pneumonitis. Five patients developed grade 1 or 2 esophagitis and 7 patients developed grade 1 or 2 pharyngeal mucositis (Table 3). Within our cohort of patients, the estimated mean overall survival was 21.2 months, and 12-month overall survival was 77.1%.
Common Terminology Criteria for Adverse Events (CTCAE) Version 4.03 Treatment-Associated Toxicities.a
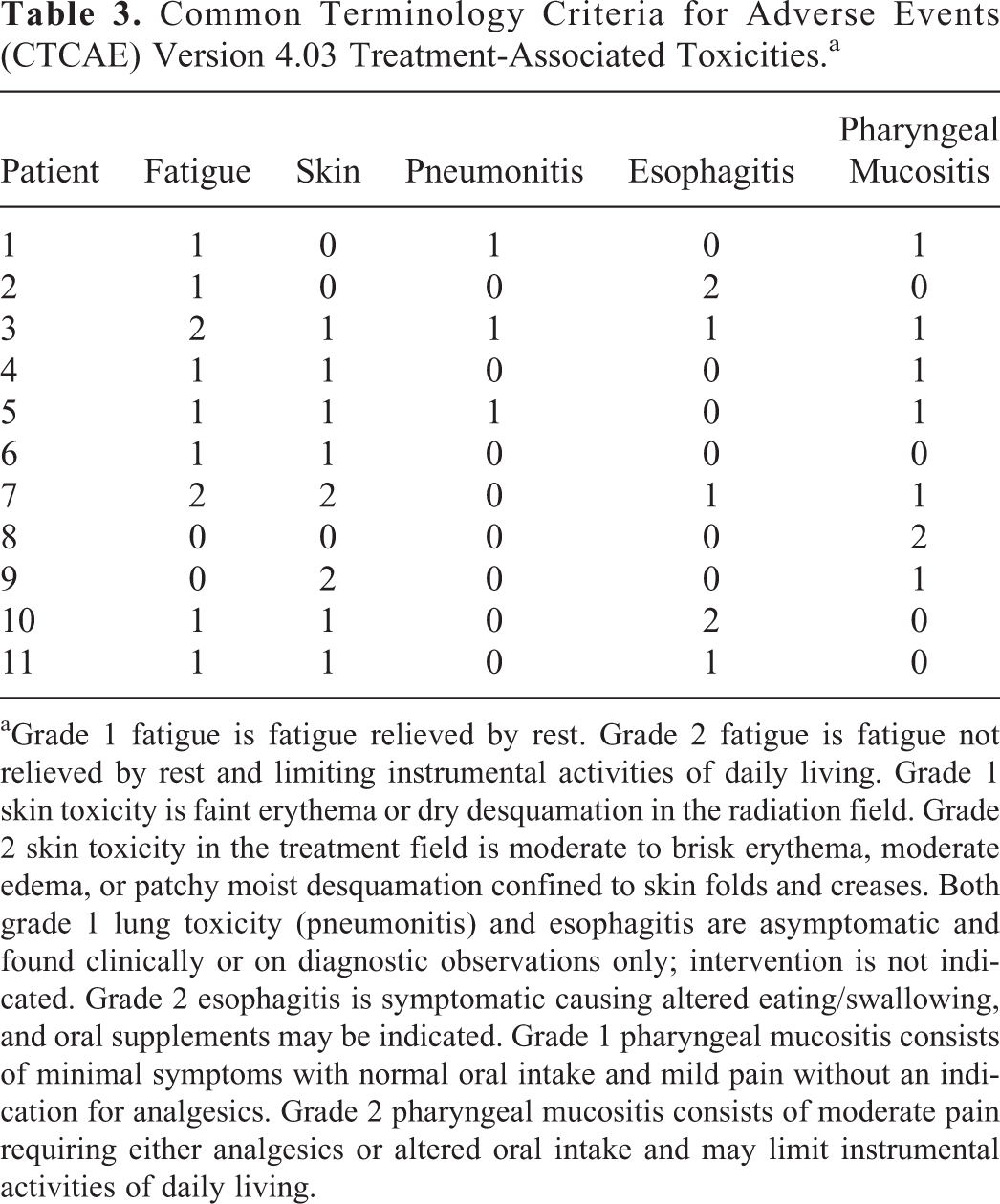
aGrade 1 fatigue is fatigue relieved by rest. Grade 2 fatigue is fatigue not relieved by rest and limiting instrumental activities of daily living. Grade 1 skin toxicity is faint erythema or dry desquamation in the radiation field. Grade 2 skin toxicity in the treatment field is moderate to brisk erythema, moderate edema, or patchy moist desquamation confined to skin folds and creases. Both grade 1 lung toxicity (pneumonitis) and esophagitis are asymptomatic and found clinically or on diagnostic observations only; intervention is not indicated. Grade 2 esophagitis is symptomatic causing altered eating/swallowing, and oral supplements may be indicated. Grade 1 pharyngeal mucositis consists of minimal symptoms with normal oral intake and mild pain without an indication for analgesics. Grade 2 pharyngeal mucositis consists of moderate pain requiring either analgesics or altered oral intake and may limit instrumental activities of daily living.
Discussion
The delivery of therapeutic radiation has evolved from the 2-dimensional era to the 3D era in which CT simulation provides the radiation oncologist with a more accurate representation of tumor volume. 15 For lung tumors, motion management most commonly involving a 4D-CT scan is used to generate CT data sets corresponding to different phases of the respiratory cycle. 16 3D-CRT and IMRT are useful tools to deliver a more conformal dose to the tumor and are now standard of practice. 17 IMRT can produce more conformal plans than 3D-CRT by optimally modulating the individual beamlets that make up the radiation beams. 17 VMAT is a type of IMRT in which the gantry is continuously moving while the MLC leaves and dose rate are varying throughout the arc. An advantage of VMAT over IMRT is a shorter delivery time and hence reduction in the amount of patient motion during treatment. 18,19
Although IMRT and VMAT can deliver a more conformal and homogeneous plan than 3D-CRT, a disadvantage of IMRT and VMAT compared to 3D-CRT is that larger normal tissue volumes are exposed to low-dose radiation. Nine-field IMRT has been demonstrated to produce larger total and contralateral lung V5 and V20 compared to 4- or 5-field IMRT and 3D-CRT. 2 The limitations of VMAT and IMRT are especially concerning when treating lung tumors because large volumes of low-dose radiation increase the risk of pneumonitis and esophagitis. 7,8,20,21 IMRT has shown reduced rates of pneumonitis compared to 3D-CRT. 22,23 The Radiation Therapy Oncology Group (RTOG) 0617 trial showed significantly higher rates of severe pneumonitis in patients treated with 3D-CRT compared to IMRT (7.9% vs 3.5%, P = .046), and the V20 may be more predictive of the risk of pneumonitis than the V5. 22 However, a meta-analysis by Hu et al shows an increased risk of esophagitis with IMRT versus 3D-CRT. 23
Hybrid RapidArc offers a reasonable alternative strategy to potentially decrease both pneumonitis and esophagitis in patients with locally advanced lung cancer treated with radiotherapy. In our study, in the initial phases of implementing the H-RA treatments, comparisons were made for patients with different dose splitting (40-60, 50-50, 60-40, etc), and 60% to 40% provided the best combination of both techniques. With the majority of the dose delivered with static beams, uncertainties inherent to IMRT were minimized. However, sufficient IMRT contribution allowed for dose carving around irregular target volumes and normal structures while maintaining conformality. With 60% of the dose in H-RA plans delivered through static beams, the integral dose to the lung is reduced. The remainder of the dose is delivered through RA beams to maintain a highly conformal plan and to reduce the esophageal dose.
Dosimetry-only studies have also shown improved conformity and decreased dose to OARs using hybrid IMRT and H-RA. Blom et al 1 showed that hybrid IMRT resulted in lower total lung V5 and contralateral lung V5, as well as better V95% PTV coverage compared to RA. The CI was improved, and lung V20, heart V60, and esophagus V60 and V40 were lower with RA plans. 1 Agapito et al 11 showed that mean lung dose, V20, V10, PTV coverage, and conformity were better with H-RA compared to 3D-CRT. However, V5, cord max, and heart dose were worse with H-RA; also, the time to deliver H-RA compared to 3D-CRT was longer in this study. 11 In a comparison of 3D-CRT versus 2-arc RA versus H-RA, there was better conformity, homogeneity, low dose to lung (V20 and less), mean lung dose, esophagus V55, and cord dose in the H-RA plans. 4 Chan et al 4 also showed that H-RA plans had shorter treatment times compared to 3D-CRT plans.
Although no clinical trials have compared H-RA to 3D-CRT for locally advanced non–small cell lung cancer, several small studies have demonstrated that hybrid IMRT can be used to create highly conformal plans to locally advanced lung tumors while reducing the volume of low dose. Mayo et al 2 used hybrid IMRT to treat cancers of the lung and esophagus. The authors treated 18 patients with static beams that delivered about two-thirds of the prescribed dose, and IMRT beams were used for the remaining one-third of the dose. They found that hybrid plans treated significantly smaller total and contralateral lung volumes. Verbakel et al 3 also reported improved lung doses in patients with non–small cell lung cancer treated with hybrid IMRT compared with comparative 3D-CRT, full IMRT, and RA plans.
Similar to the results of the aforementioned studies, we demonstrate that H-RA resulted in significantly decreased total and contralateral lung V20 and mean doses compared to 3D-CRT. Additionally, esophageal mean dose and V60 were significantly lower in the H-RA plans compared to the 3D-CRT plans. We demonstrated a significant improvement in CI (1.25 vs 1.81) and HI (0.094 vs 0.136) in the H-RA plans (P < .05). We also showed significant improvement in HI and contralateral lung doses in H-RA plans compared to the RA-only plans. Interestingly, RA plans did have improved maximum spinal cord doses compared to H-RA plans. However, at the maximum spinal cord doses reported (45 Gy for H-RA plans and 42.9 Gy for RA plans), this may not be clinically relevant, as the probability of myelopathy at 45 Gy is 0.03%. 24 Likewise, the improvement in heart V40 and V45 with RA plans over H-RA plans is probably not clinically relevant, as these doses in our study were all under 20%. Emami et al have reported a 5% risk of pericarditis at 5 years with a heart V45 of 66%. 25 It has also been reported that a mean heart dose under 26 Gy reduces the risk of pericarditis to under 15%. 26
Unique to our study was that patients were treated with H-RA. Previous studies have reported dosimetry and clinical outcomes in patients treated with hybrid IMRT. 2,3 We report comparable or improved dosimetry and toxicity in patients treated with H-RA. Mayo et al reported better lung V5 and V20 with hybrid IMRT compared to our reported V5 and V20. 2 However, the average PTV for patients with lung cancer in the Mayo study was 179.1 cm3, whereas our average PTV was 513 cm3. Verbakel et al reported toxicities of 14 patients with lung cancer treated with hybrid IMRT. Five patients developed grade 3 esophagitis, and 3 developed grade 3 pneumonitis. 3 No patient in our cohort developed grade 3 toxicity with H-RA treatment.
One of the limitations of this study is the small number of patients in our cohort. Although the H-RA plans had significantly improved lung V20 and mean lung and esophageal doses, the overall differences were small and may not be clinically relevant. However, it has been reported that esophageal V60 is the best predictor of radiation esophagitis. 7 With a V60 >17%, the risk of grade ≥3 radiation esophagitis is 22%, whereas the risk of grade ≥3 radiation esophagitis is <10% with an esophageal V60 ≤17%. 7 In our study, 6 of 11 H-RA plans had an esophageal V60 >17%; of the 3D-CRT plans, 9 of 11 had an esophageal V60 >17%. Seven of 11 RA plans had an esophageal V60 >17%. Shaikh et al reported that the risk of radiation pneumonitis is significantly increased with a lung V5 >65% and a V20 >25%, 21 while secondary analysis of RTOG 0617 indicates that V20 is more predictive of radiation pneumonitis risk. 22 In the H-RA and RA plans in our study, 9 of 11 had a V20 ≥25%, whereas the V20 was ≥25% for all 11 of the 3D-CRT plans. Given the importance of the esophageal V60 and lung V20, H-RA may be used to reduce the dose to the normal esophagus and lung and potentially reduce the risk of radiation esophagitis and pneumonitis. Another limitation of this study is its retrospective nature, as there is potential selection bias for our patient cohort, and because patients were not treated on a prospective clinical trial, long-term follow-up is limited. A third limitation is that motion management was not used. In our clinical practice, patients with bulky mediastinal tumors are not set up with motion management such as breath-hold or compression bridge due to concerns for reproducibility and patient tolerance. The breathing motion was accounted for using 4D-CT and assessing internal motion for ITV generation.
To our knowledge, this is the first report on the clinical application of H-RA in patients with locally advanced lung cancer, with reported toxicity and survival. Hybrid RapidArc permitted safe delivery of 60 to 66 Gy to large lung tumors with concurrent chemotherapy and demonstrated advantages for significant reduction in mean total and contralateral lung dose, mean esophageal dose, and mean heart dose. Improved plan conformity and homogeneity were achieved with H-RA. Treatment was well tolerated, with no grade 3 or higher toxicities reported. All patients maintained their pretreatment diet without requiring placement of a feeding tube. No patient developed symptomatic radiation-induced pneumonitis. By reducing dose to OARs, H-RA may decrease the risk of radiation toxicity. We conclude that H-RA may be preferable to 3D conformal techniques for the treatment of large lung tumors, bulky mediastinal adenopathy, and stage III disease.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.