
Abstract
Objective:
To describe the clinical and pathological features of endometrial carcinoma with extraperitoneal metastasis and examine whether surgery could improve the prognosis.
Methods:
The Surveillance, Epidemiology, and End Results database was used to analyze 730 patients who were diagnosed with extraperitoneal metastasis of endometrial cancer from 2010 to 2015, including metastasis to the lung, bone, or brain.
Results:
Of the 730 patients, 372 (50.96%) patients had single lung metastases, and 196(26.85%) patients had multiple organ metastases that included pulmonary invasion. Therefore, the lung was the most common target organ for extraperitoneal metastasis of endometrial cancer. In multivariate risk factor analysis, grade 3 tumor (odds ratio = 3.39, P < .001), positive peritoneal cytology (odds ratio = 2.02, P < .001), and cervical stromal invasion (odds ratio = 1.42, P = .030) were independent risk factors for extraperitoneal metastasis. Once metastasis occurred in the brain or multiple organs, the prognosis was often poor. Of the patients, 362 underwent surgery, and surgery was performed only for primary tumors of the reproductive organs in almost all patients (97.23%) with extraperitoneal metastasis. The median cancer-specific survival periods of patients with solitary pulmonary metastasis undergoing surgery and those without surgery were 23 (16.43-29.57) months and 9 (6.21-11.79) months, respectively (P < .001), and survival superiority also existed in patients with bone metastasis (19 vs 8 months, P = .015) and multiple organs metastases (15 vs 4 months, P < .001). However, patients with brain metastasis had the same median survival period in the 2 groups (6 months, P = .146).
Conclusions:
The lung was the most common target organ for extraperitoneal metastasis in patients with endometrial cancer. Surgery was associated with improved survival in women with extraperitoneal metastasis, except for patients with brain metastasis.
Introduction
The incidence and mortality of endometrial cancer are increasing. 1 Patient prognosis is relatively optimistic in the early stages, especially for endometrioid carcinoma. However, the prognosis for patients with advanced disease is extremely poor, with metastasis being the main cause of death. 2 According to the International Federation of Gynecology and Obstetrics (FIGO) 26th Annual Report on the Results of Treatment in Gynecological Cancer, the incidence of stage IV endometrial cancer was 3% and the 5-year survival rate was 19% 3 It is difficult to clarify the clinical characteristics of patients with extraperitoneal metastasis due to the low incidence and variable presentation. Several retrospective studies have shown that surgery could improve prognosis in this disease. 4 -6 However, some authors contend that the prognosis of advanced endometrial cancer depends on its biological characteristics and that surgery was not a protective factor for survival. 7 Furthermore, in clinical practice, it is often difficult to determine if surgery is worth performing once extraperitoneal metastasis occurs. The treatment options in the 2018 National Comprehensive Cancer Network (NCCN) guidelines for advanced endometrial adenocarcinoma are equally variable. 8 Strategies for the treatment of extraperitoneal metastasis require more extensive research. In this study, we analyzed the clinical features of endometrial carcinoma with extraperitoneal metastasis, including lung, bone, and brain metastases, and investigated the value of surgery in patient prognosis.
Materials and Methods
The patients were selected from the SEER database. The eligibility criteria included the following: (1) a primary diagnosis of endometrial cancer, including metastasis to at least one site that included the lung, bone, or brain, between 2010 and 2015; and (2) a pathological diagnosis of endometrioid adenocarcinoma, serous adenocarcinoma, or clear cell adenocarcinoma.
A total of 730 patients met the inclusion criteria. Extraperitoneally negative patients with stage III or stage IVA endometrioid adenocarcinoma, serous adenocarcinoma, or clear cell adenocarcinoma tumors during the same period were selected as the control group (n = 3650). The recorded data included the age at diagnosis, grade, histology, tumor invasion, lymphatic dissemination, surgery, peritoneal cytology, extraperitoneal metastatic organs, and months of survival. The surgical site was recorded by program coding. Codes 40 and 50 represented total hysterectomy with or without removal of a fallopian tube and ovary, and code 60 represented radical hysterectomy. Codes 11 and 12 represented local tumor destruction via photodynamic therapy or fulguration. However, the local location was not clear. Survival was calculated as the number of months from cancer diagnosis to death.
SPSS Statistics version 22 was used for the statistical analyses. The clinical and pathological characteristics were compared using Pearson χ2 and Fisher exact tests. Multivariate logistic models were performed to estimate the odds ratio (OR) and 95% CI to analyze independent risk factors for extraperitoneal metastasis. The Kaplan-Meier and log-rank tests were used to estimate survival and compare differences between the groups, respectively. Values of P less than .05 were considered statistically significant.
Results
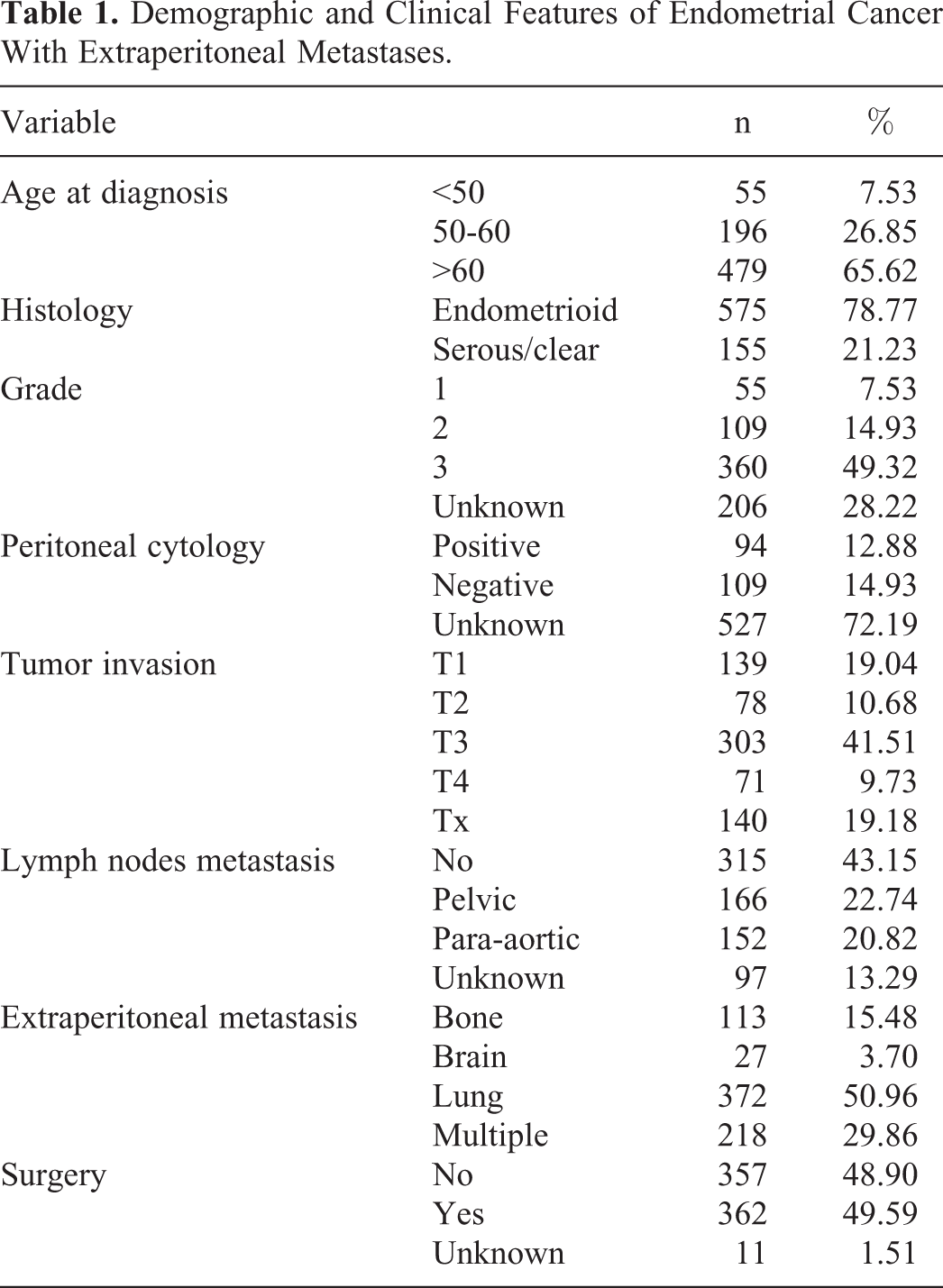
Patients with stage IVB accounted for 5.67% (4231) of the cases in the SEER database. Before 2010, this proportion was only 2.44%. A total of 730 patients with stage IVB disease were diagnosed with at least one extraperitoneal metastasis, such as to the lung, bone, or brain. The demographic and clinical features of the patients with endometrial carcinoma with extraperitoneal metastasis are shown in Table 1. The average age at diagnosis was 64.81 ± 10.92 years. Of the 730 patients, 113 (15.48%) presented with bone metastases, 372 (50.96%) with lung metastases, 27 (3.70%) with brain metastases, and 218 (29.86%) with multiple metastases (including two or more metastatic organs). One hundred ninety-six patients had multiple organ metastases that included pulmonary invasion. Therefore, the proportion of lung metastasis in patients with extraperitoneal metastasis was as high as 77.81%. Of the patients, 362 patients underwent surgery, 317 of which underwent total hysterectomies with or without removal of a fallopian tube and ovary. Thirty-five patients underwent radical hysterectomies. Another 10 patients had local tumor destruction. In our cohort, surgery was performed for primary tumors of the reproductive organs in almost all patients (97.23%) with extraperitoneal metastasis. Surgery was not performed at the metastatic site. However, in the 10 patients who received photodynamic therapy or fulguration, the location of the tumor destruction was not clear. In multivariate models, grade 3 tumor (OR = 3.39, P < .001), positive peritoneal cytology (OR = 2.02, P < .001), and cervical stromal invasion (OR = 1.42, P = .030) were independent high-risk factors for extraperitoneal metastasis compared to patients with advanced disease without extraperitoneal metastasis (Table 2).
Demographic and Clinical Features of Endometrial Cancer With Extraperitoneal Metastases.
Multivariate Risk Factor Analysis for Extraperitoneal Metastases.
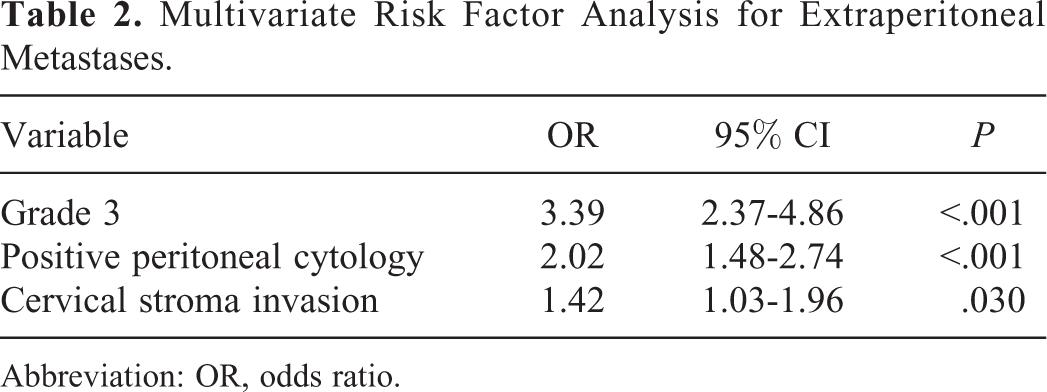
Abbreviation: OR, odds ratio.
Kaplan-Meier univariate analysis of the entire cohort of patients with endometrial cancer with extraperitoneal metastasis revealed that, in addition to tumor grade and lymph node metastasis, extraperitoneal metastasis of organs and surgery were 2 important factors affecting survival. The median survival period of the different groups based on surgery is shown in Table 3. The median survival periods of patients with lung, bone, or brain metastases were 17 (14.25-19.75) months, 15 (8.55-21.45) months, and 6 (1.40-10.60) months, respectively. Once multiple metastases occur, the median survival period was 7 (4.41-9.60) months. In evaluating the effect of surgery on survival, the median survival periods of patients with lung, bone, brain, and multiple organs metastases that did undergo surgery were 9 months, 8 months, and 4 months, respectively; whereas surgery significantly improved the survival of patients with lung, bone, or multiple organ dissemination to median survival periods of 23 months, 19 months, and 15 months, respectively. However, there was no significant difference in the survival of patients with brain metastasis who underwent surgery and those who did not.
The Median Survival Period of Different Groups Based on Surgery (Months).

Discussion
The epidemiology of endometrial cancer with distant metastasis is not well characterized due to the rarity of this condition. According to the FIGO 26th Annual Report, approximately 3% of patients with endometrial cancer treated between 1999 and 2001 were classified with stage IV disease. 3 Our results, based on SEER data, demonstrated that the incidence of stage IVB disease increased to 5.67% from 2010 to 2015, indicating an increased incidence in patients with advanced endometrial cancer. In stage IVB disease, most patients have intra-abdominal metastasis, such as liver and omentum invasion, and only 17.25% of the patients had extraperitoneal metastasis. Poorly differentiated, positive peritoneal cytology, and cervical stromal invasion are independent high-risk factors for extraperitoneal metastasis. These factors have been widely accepted as high-risk endometrial cancer features by clinicians. It is worthy to emphasize that, clinically, more attention should be paid to patients with high-risk factors who are prone to extraperitoneal metastasis.
Endometrial carcinoma has the highest frequency of pulmonary metastasis compared to other gynecologic malignancies, such as cervical and ovarian cancers, occurring in up to 20% to 25% of the patients with reoccurrence. 9 In our study, the lungs accounted for the majority of the affected organs (77.81%). In patients with multiple organ metastases, pulmonary metastases were found in 89.91% of the cases. The prevalence of bone metastasis in endometrial carcinoma ranges from 4% to 7%, which is the second most commonly involved extraperitoneal organ, 10 whereas central nervous system involvement is relatively rare (1%). 11 The prognosis of patients with stage IVB disease is generally poor. 12,13 Patients with lung or bone metastases often have better outcomes than patients with brain metastasis (median cancer-specific survival period 15 or 14 months vs 6 months, respectively). Once multiple metastases occur, the prognosis is very poor, with a median survival time of 7 months. Turan reported that the overall survival of patients with isolated pulmonary metastasis was 54 months, compared to 10 months in patients with synchronized pulmonary recurrence (metastasis to other organs as well). 14
Surgery remains controversial for patients with advanced endometrial cancer with distant metastasis. Tanioka et al 7 suggested that optimal cytoreductive surgery as a primary therapy was not significantly correlated with overall survival. However, the histologic characteristics and the extent of the disease were more important determinants of outcomes than any type of treatment. The 2018 NCCN guidelines recommended choosing palliative hysterectomy with or without chemotherapy, radiotherapy, or hormonal therapy according to the characteristics of stage IVB. 8 However, in recent years, surgery as an important basic treatment has become widely accepted by researchers. Several studies have reported that optimal surgical cytoreduction was essential for achieving the best therapeutic effects. 15 -17 Ueda et al 18 showed that the median progression-free survival and overall survival (OS) of patients with optimal cytoreduction were significantly better than those with suboptimal reduction, not only among stage IVB patients with only intra-abdominal metastasis but also among patients with extra-abdominal metastasis. A meta-analysis by Barlin et al 19 reported that optimal cytoreduction could improve survival in advanced and recurrent endometrial cancer. Of note, most extraperitoneal metastases were unresectable in these studies. 15 -17 Eto found that intra-abdominal optimal cytoreductive surgery, including hysterectomy, were prognostic factors in the presence of extra-abdominal metastasis. 20,21 We compared the OS between patients who underwent surgery and those who did not. Surgery was performed only for primary tumors of the reproductive organs in almost all cases in our study, and the results confirmed that surgery had a beneficial effect on prognosis. Surgery prolonged the cancer-specific survival of patients with isolated lung or bone metastases, but not for patients with brain metastasis. Surgical intervention was a favorable prognostic factor even in patients with multiple organ metastases.
Due to the complexity of advanced tumors and poorer performance in elderly patients, a surgical strategy to achieve optimal cytoreduction is worth consideration. In a study by Rabinovich, the neoadjuvant setting was associated with maximal debulking rates and improved or equivalent survival. 16 Eto et al 20 divided 426 stage IVB patients into 3 groups according to their initial treatment: primary surgery, primary chemotherapy, and palliative care. The median OS of these groups was 21, 12, and 1 month, respectively (P < .0001). In the primary chemotherapy group, when patients subsequently underwent surgery, they achieved similar OS to those in the primary surgery group. Based on these studies and our results, surgery is recommended as the first treatment choice for endometrial cancer with distant metastasis when optimal cytoreductive surgery is applicable. Otherwise, preoperative reduction of the tumor burden by chemotherapy is the most advantageous choice.
Brain metastasis is rare in endometrial cancer and the prognosis is generally poor. Our research revealed that patients with brain metastasis had a median survival time of approximately 6 months, which is much shorter than the expected survival for metastasis to other organs. Strategies for brain metastasis include surgical resection, chemotherapy, and radiotherapy, for example, stereotactic radiosurgery and whole-brain radiation therapy. Each treatment has shown efficacy in some literature reviews of case reports and studies with small case series. 22 -24 Uccella et al 25 found that complete surgical resection of cerebral lesions plus radiotherapy was independently associated with prolonged survival after a diagnosis of brain metastasis, whereas our study indicated that surgery did not improve the survival of those patients. The potential value of surgery needs further study. We prefer to make individualized plans according to the patient’s physical condition, the regions of the brain affected, the degree of dissemination, and other relevant factors, with the aim of improving the patient’s end-stage quality of life and survival.
There are some limitations to our study. First, adjuvant therapy is an important treatment for patients with advanced endometrial cancer. However, chemotherapy and radiotherapy data of the patients were not available due to the limitations of the database. Therefore, the impact of radiotherapy and chemotherapy on the patients could not be analyzed. Second, almost all patients in our study were treated only for primary tumors, except for 10 individual patients where the location of the tumor destruction was unclear. It is not clear whether the removal of a metastatic tumor benefits patients with advanced disease. The best surgical treatment strategy for patients with distant metastasis needs to be further explored.
In conclusion, stage IVB disease with extraperitoneal metastasis was closely related to grade 3 tumors, positive peritoneal cytology, and cervical stromal invasion. Surgery at the primary site played an important role in improving the survival of patients, except for patients with brain metastasis. Individualized treatment strategies, including optimal cytoreductive surgery and pre- and postoperative adjuvant therapy, should be selected according to the patient’s condition.
Footnotes
Authors’ Note
Our study did not require an ethical board approval because it did not contain human or animal trials.
Acknowledgments
Thanks for the fund support provided by Beijing High-level Health Personnel Training Program (2015-3-090).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was support by Beijing High-level Health Personnel Training Program (2015-3-090).