
Abstract
Purpose:
To assess the efficacy of stereotactic body radiotherapy in patients with unresectable locally advanced pancreatic cancer.
Materials and Methods:
All patients received a prescription dose of 45 Gy in 6 fractions. Primary end point was freedom from local progression. Secondary end points were overall survival, progression-free survival, and toxicity. Actuarial survival analysis and univariate or multivariate analysis were investigated.
Results:
Forty-five patients were enrolled in a phase 2 trial. Median follow-up was 13.5 months. Freedom from local progression was 90% at 2 years. On univariate (P < .03) and multivariate analyses (P < .001), lesion size was statistically significant for freedom from local progression. Median progression-free survival and overall survival were 8 and 13 months, respectively. On multivariate analysis, tumor size (P < .001) and freedom from local progression (P < .002) were significantly correlated with overall survival. Thirty-two (71%) patients with locally advanced pancreatic cancer received chemotherapy before stereotactic body radiotherapy. Median overall survival from diagnosis was 19 months. Multivariate analysis showed that freedom from local progression (P < .035), tumor diameter (P < .002), and computed tomography before stereotactic body radiotherapy (P < .001) were significantly correlated with overall survival from diagnosis.
Conclusion:
Stereotactic body radiotherapy is a safe and effective treatment for patients with locally advanced pancreatic cancer with no G3 toxicity or greater and could be a promising therapeutic option in multimodality treatment regimen.
Introduction
Pancreatic ductal adenocarcinoma is characterized by a poor prognosis, with a 5-year overall survival (OS) rate of about 6%. 1,2 Surgery is the gold standard of care with 5-year OS rates of 20% to 25%. More than 50% of patients, however, are unresectable at the time of diagnosis, mainly due to locally advanced disease or distant metastases. 3 In patients with locally advanced pancreatic cancer (LAPC), the integration of chemotherapy and chemoradiation treatment (CRT) is the current therapeutic option associated with a significant grade 3 to 4 toxicity rate and with a median OS of 5 to 15 months. 4 –8
In the last years, the feasibility and efficacy of stereotactic body radiotherapy (SBRT) in the treatment of pancreatic cancer were investigated, 9 but only few prospective trials have been performed and several studies reported significant late toxicity rates. 10 –23
The aim of this study was to investigate the efficacy and safety of pancreatic SBRT with a total dose of 45 Gy in 6 fractions of 7.5 Gy/fraction.
Materials and Methods
Enrolment and Eligibility
Patients with histologically proven LAPC were enrolled in this prospective, observational, single-arm, single-institution phase 2 trial, approved by the Humanitas Ethical Review Board. All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all participants.
Primary end point was local control (LC) such as freedom from local progression (FFLP). Secondary end points were OS, progression-free survival (PFS), and toxicity rate.
Inclusion criteria were histologically proven unresectable primary pancreatic adenocarcinoma, age ≥18 years, Karnofsky performance score of at least 70, lesions with maximum diameter not exceeding 5 cm, negative lymph node, and absence of distant metastasis. Exclusion criteria were previous abdominal radiotherapy, nodal and/or metastatic disease, gastric or duodenal obstruction, and concurrent chemotherapy.
All patients were evaluated by a medical oncologist, a biliary–pancreatic surgeon, a radiologist, and a radiation oncologist in a multidisciplinary board.
Unresectable pancreatic cancer was defined according to the American Hepato–Pancreato–Biliary Association/Society of surgical Oncology/Society for Surgery of the Alimentary Tract criteria 24
Stereotactic Body Radiation
Patients were immobilized in supine position with the arms above the head, using a thermoplastic body mask including a Styrofoam block for abdominal compression to minimize internal organ motion (spontaneous or breath induced).
A contrast-free and venous phase contrast-enhanced computed tomography (CT) scan with a slice thickness of 3 mm was acquired for all patients. The clinical target volume (CTV), defined as the gross tumor volume (GTV) with no additional margins, was delineated on the venous phase of CT scan.
Eight patients had a positive staging [18F]fluorodeoxyglucose-positron emission tomography (FDG-PET). In this subpopulation of patients, FDG-PET scan was acquired during the simulation phase, and planning CT images were coregistered (with deformable registration methods) with positron emission tomography–computed tomography (PET-CT) to better identify the GTV.
In all 8 patients, no significant difference in the GTV defined by PET and by venous contrast-enhanced CT was detected.
The planning target volume (PTV) was generated from GTV by adding a margin of 5 mm in the left–right direction, 5 mm in the anterior–posterior direction, and 10 mm in the cranial–caudal direction. Organs at risk (OARs), including the duodenum, the stomach, the small bowel, the kidneys, the liver, and the spinal cord, were contoured.
Stereotactic body radiotherapy plans were optimized and delivered according to the RapidArc (Varian Medical Systems, Palo Alto, California) volumetric-modulated arc technique. Beam energy of 6 to 10 MV with flattened or unflattened Flattening Filter Free (FFF) photon beams was selected for all patients. Treatments were delivered by a TrueBeam linear accelerator (Varian Medical Systems).
A total dose of 45 Gy was given in 6 consecutive daily fractions (7.5 Gy/fraction) with plan normalization to the mean dose to CTV. Biologically equivalent dose was 78.8 and 157.5 Gy using α/β = 10 Gy for tumor and α/β = 3 Gy for late gastrointestinal toxicity, respectively. The optimization of the dose distribution was performed with the purpose of achieving the following clinical goals. A required target coverage of V95% = 100% for the CTV. A maximum acceptable dose heterogeneity to the CTV of D98% > 95% and D2% < 107%.
For PTV, the same objectives were ideally to be achieved but with a lower priority than the constraints to the OARs. The dose–volume constraints for the OARs were duodenum D1cm3 < 36 Gy, stomach and small bowels D3cm3 < 36 Gy, kidneys V15Gy < 35%, liver, total spared volume (Vtot − V21Gy, ) > 700 cm3, and spinal cord D1cm3 < 18 Gy.
Image guidance was performed by means of cone beam CT imaging before every treatment session to verify the correct position of the patient.
Response Evaluation and Follow-Up
Patients underwent clinical assessment at 1 month after SBRT and then every 3 months thereafter by the treating radiation oncologist. Clinical examination, evaluation of CA19-9 levels, and a contrast-enhanced CT scan were performed at each step of the follow-up. A PET-CT scan was also performed every 6 months after SBRT in those patients who had a pre-SBRT staging PET-CT scan. Local control was defined according to RECIST criteria. 25 Acute and late toxicity was scored according to the National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events (CTCAE) v3.0. 26
Statistical Analysis
Plan quality assessment was performed by means of numerical analysis of the dose–volume histograms computed for each organ/structure from the treatment plan. Several metrics were computed and results will be reported for the dose–volume parameters used as objectives in the optimization. The conformity index was defined as the ratio of the body volume irradiated at 95% of the prescription dose to the volume of the target (PTV).
From the clinical point of view, the primary end point of this trial was to evaluate LC. Freedom from local progression was calculated from the end of SBRT to the first assessment of local progression. Patients who did not develop local disease progression were censored at the date of the last scan.
Secondary end points were PFS, OS, and toxicity. Progression-free survival was calculated from the end of SBRT to the first assessment of disease progression, and OS was calculated from the end of SBRT to death.
Freedom from local progression, PFS, and OS rates were calculated by Kaplan-Meier method, and the log-rank test statistic was used for univariate analysis to assess the level of statistical significance between the strata of selected prognostic factors. Cox regression provided a multivariate analysis of these end points with selected prognostic factors. A significant difference was considered when P ≤ .05.
Results
Forty-five patients were enrolled from 2011 to 2013; 43 were available for analysis (Figure 1). Patients and treatment characteristics are shown in Table 1. Median CTV was 23.97 cm3 (range: 3.66-53.59 cm3) and median PTV was 64.73 cm3 (range: 21.3-127.4 cm3).
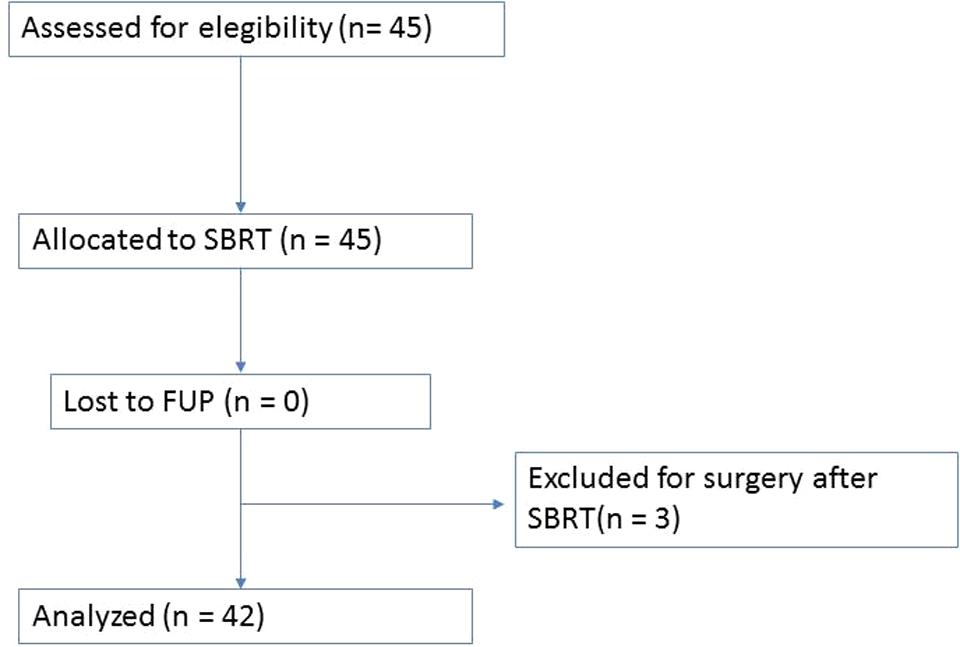
Study schematics.
Patients Characteristics.

Abbreviations: CTV clinical target volume; PTV, planning target volume; SBRT, stereotactic body radiotherapy.
Thirty-two (71%) patients received pre-SBRT chemotherapy, completed at least 2 weeks before SBRT. Table 2 presents the results of the numerical analysis of the treatment plans from a dose point of view. All planning objectives were respected for both target coverage and OARs sparing with only 1 mild violation in the duodenum for a patient receiving 36.5 Gy as near-to-maximum dose instead of the objective of <36 Gy. Conformity index resulted 1.11 ± 0.21.
Summary of Planning Dose–Volume Objectives.a

Abbreviations: CTV, clinical target volume, DVH, dose–volume histogram; PTV, planning target volume.
aResults are reported as mean and standard deviation. Values inside the square brackets represent the range.
Median follow-up was 13.5 months (6-48 months). Eight (18%) patients were alive at the time of analysis. Median follow-up in this group was 23.5 months (range 11-48 months).
Thirty-two (71%) patients received pre-SBRT chemotherapy, completed at least 2 weeks before SBRT. Chemotherapy cycles ranged between 3 and 14. Nineteen percent of these patients received a gemcitabine-based chemotherapy. The variability of regimen and number of cycles of systemic therapy were related to the PS, age, comorbidity, and compliance of patients and to the chemotherapy-related toxicity. The remaining 29% of the enrolled patients were not eligible to CT for age, comorbidity, or performance status.
Three patients had an important tumor regression at about 3 months after SBRT and were treated with radical surgery. These patients were excluded from the final analysis (Figure 1).
Twenty (48%) patients received CT at the time of local and/or systemic disease progression after SBRT. Gemcitabine-based chemotherapy was used in 14 patients, Fluorouracile-Irinotecan (FOLFIRI) in 4 patients, and capecitabine in 2 patients. A total of 11 patients were not eligible to CT at the time of disease progression for age or poor performance status. Table 3 summarizes the results for FFLP, OS, and OS from diagnosis (OSd).
Summary of the Actuarial Analysis for FFLP, PFS, OS, and Osd.

Abbreviations: CI, confidence interval; FFLP, freedom from local progression; OS, overall survival; OSd, overall survival from diagnosis; PFS, progression-free survival.
The actuarial curve for FFLP is shown in Figure 2A. Local progression occurred in 2 patients at 4 and 6 months and in 1 patient at 8 and 29 months. On univariate analysis, tumor diameter (P < .03) was statistically significant for LC (Table 4). One- and 2-year FFLP rates were 100% for patients with lesion size <3.5 cm and 76% for lesion size >3.5 cm (Figure 2B).
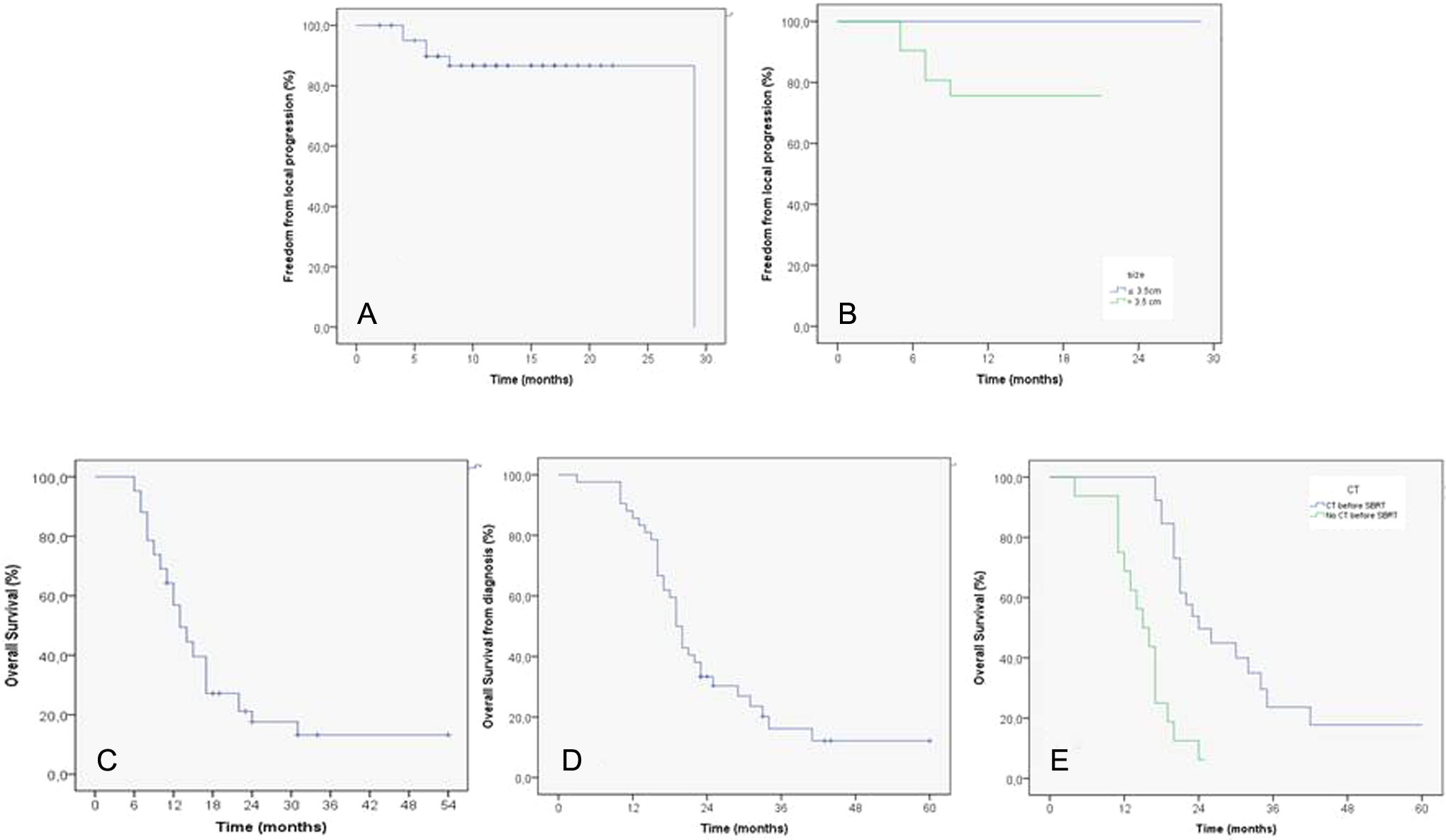
Actuarial survival curves of (A) freedom from local progression (FFLP); (B) FFLP for smaller and larger lesions; (C) progression-free survival; (D) overall survival; (E) overall survival from diagnosis (OSd); and (F) overall survival for patients who received (not received) chemotherapy before stereotactic body radiotherapy (SBRT).
Results of Univariate and Multivariate Analysis (P values).

Abbreviations: CT, computed tomography; FFLP, freedom from local progression; OS, overall survival; OSd, OSd, overall survival from diagnosis; SBRT, stereotactic body radiotherapy.
Actuarial OS is shown in Figure 2C; median OS was calculated from the end of SBRT. Eight (18%) patients were alive at the time of analysis, with a median OS of 23.5 months. On multivariate analysis, tumor size (P < .001) and FFLP (P < .002) were significantly correlated with OS (Table 4).
The actuarial curve for the OSd is shown in Figure 2C. On univariate analysis, CT before SBRT (P < .015) was significantly associated with OSd (Table 4). Median OSd was 23.93 months in those patients treated with CT and sequential SBRT and 15 months in those patients treated with only SBRT (Figure 2E). On multivariate analysis, FFLP (P < 0.035), tumor diameter (P < .002), and CT before SBRT (P < .001) were significantly correlated with OSd.
Figure 3 represents a typical treatment and a clinical response after SBRT. In the figure, the contour is the CTV that is reported together with the dose (in color wash ranging from 95% to 107% of the dose prescription to enhance the appraisal of the dose conformity, the PTV contour falls at the edge of the color wash). The follow-up image was acquired 6 months after treatment.

A typical example of treatment: (A) target volume before stereotactic body radiotherapy (SBRT); (B) dose distribution; (C) treatment response at 6 months after treatment during follow-up. Dose distribution is shown with color wash set at 95% to 107% of the prescription dose. The clinical target volume (CTV) contour is shown in the center of the dose distribution, and the planning target volume (PTV) contour is at the edge of the color wash.
Twenty-one (49%) patients experienced mild or moderate acute toxicity (grade 1 or 2): 4 (10%) nausea, 16 (37%) fatigue, and 1 (2%) abdominal pain. No case of acute toxicity ≥G3 was detected. Only 2 patients (4%) experienced late toxicity. These patients developed G2 gastritis after more than 3 months from SBRT, and they were treated with proton pump inhibitor (PPI). No late toxicity ≥G3 was experienced.
According to the Numerical Rating Scale scoring system, 17 (39%) patients experienced pain before SBRT. In 10 (62%) patients, pain control after treatment allowed suspension of analgesics administration; in 5 (28%) patients, analgesics dosage was reduced by 50%; and in 2 (10%) patients, administration was reduced by 20%.
Discussion
In the past years, the role of SBRT in the treatment of unresectable pancreatic cancer was investigated to confirm the hypothetical advantages of this therapy over conventional CRT.
As shown by Brunner et al, 9 higher LC related to the high doses used, short overall treatment time, and sequential integration with systemic therapy represent the crucial advantages of SBRT, but the dose-related gastrointestinal toxicity is still a serious open issue (Table 5).
Summary of treatment regimen, LC, PFS, OS, and late toxicity in recent study.

Abbreviations: FFLP, freedom from local progression; fr, fraction; GI, gastrointestinal toxicity; LAPC, locally advanced pancreatic cancer; OS, overall survival; PFS, progression-free survival; SBRT, stereotactic body radiotherapy.
Most of the published studies, indeed, demonstrated that acute toxicity was generally mild, but late toxicity was significant, with rates up to 18% to 47%. 12,13 Results of this phase 2 trial demonstrated that SBRT represents a significant and safe therapeutic option for patients with unresectable LAPC. Fractionation adopted in our study, indeed, was associated with a satisfactory LC rate, particularly for small lesions, with a very low toxicity profile. A promising OS rates were achieved almost in patients with LAPC and a low pre-SBRT CA19-9 value and in patients treated with CT before SBRT. In our study, indeed, no patients experienced perforation, ulcer, bleeding, or other acute or late grade 3 toxicity or higher. Only 2 patients experienced grade 2 late gastritis, confirming the safety of our SBRT regimen. We feel that this optimal toxicity profile is due to the crucial factors: our immobilization system that minimizes the internal organ motion, reducing the dose to OARs and the high conformity of dose, and the priority to duodenal, stomach, and bowel dose constraints. That is to limit the maximum dose to 36 Gy. Prospective studies on the efficacy of SBRT in patients with unresectable pancreatic cancer showed a 1-year LC rate ranging from 40% to 95% (Table 5). Satisfying results in terms of FFLP are reported in 4 phase 1 and 2 trials: 3 studies from Stanford University 11,13 –15 using a single fraction (25 Gy) and 1 from Baltimore group 17 using 3 fractions (15-30 Gy), with 1-year FFLP rate of about 92% to 100%. Reported rates of late duodenal ulceration, however, were significant (20%-47%). In 2014, the same group from Stanford University published a prospective study on SBRT in 5 fractions (33 Gy), with a decreasing late toxicity rate and 1-year FFLP rate of 78%. In our trial, fractionation of 45 Gy in 6 fractions allowed to achieve encouraging 1-year FFLP rates for LAPC with a very low toxicity profile. The correlation between FFLP and tumor diameter at univariate and multivariate analyses suggested the importance of dose escalation in patients with large lesions. As shown in our previous pilot study 21 and recently confirmed by Brunner et al, LC seems to be correlated with higher prescription dose. 9
In our experience, the importance of LC in patients with pancreatic cancer treated with SBRT is confirmed by significant correlation between FFLP and OS.
In most of the prospective published studies on SBRT for LAPC, median OS ranged from 5.7 to 19 months (Table 2). Better results were achieved when SBRT was performed after chemotherapy, with a median OS ranging from 10.3 to 20 months. 13,15–16,19 –23 These data could be related not only to the efficacy of systemic therapy but also to the selection of patients with a genetic tendency to local progression, during the time of CT.
In our phase 2 trial, median OS calculated from the end of SBRT was 13 months. As previously shown, tumor size and LC were significant prognostic factors, although the use of CT before SBRT was closely (P = .071) but nonsignificantly correlated with OS.
When calculated from diagnosis, median OS was 19 months. Most of the patients (71%), indeed, were suitable for sequential CT, administered before SBRT. Median OSd improved significantly not only in those cases with small lesions and optimal LC but also in patients pretreated with CT. In this setting of patients, median OSd was about 2 years. These results may confirm the importance of sequential integration of chemotherapy and SBRT in the treatment of LAPC. 9 A several number of elderly patients or unfit or with important comorbidity, however, are not suitable for chemotherapy. In our experience, even though 29% of enrolled patients with LAPC were not eligible to CT for age, comorbidity, or performance status, outcome after only SBRT was encouraging, with median OSd of 15 months. These data suggest that SBRT may be a viable alternative treatment also in patients with poor performance status, thanks also to low toxicity.
Conclusion
Freedom from local progression and OS in patients with unresectable locally advanced pancreatic adenocarcinoma seem to be improved by SBRT. Our results suggest that SBRT can be considered an effective and safe therapeutic option in the multimodality treatment of this disease.
Future studies and trials are needed to evaluate the escalation dose and the best integration with systemic therapy to improve the outcomes of these patients in terms of LC and OS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: L. Cozzi acts as Scientific Advisor to Varian Medical Systems and is Clinical Research Scientist at Humanitas Cancer Center. All other co-authors have no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.