
Abstract
In our center, the feasibility and related acute toxicities of hypofractionated helical tomotherapy have been evaluated in older aged patients with prostate cancer . Between February 2009 and February 2014, 67 patients (older than 65 years) were enrolled in a prospective phase I-II study (registered number, ChiCTR-ONC-13004037). Patients in cohort 1 (n = 33) and cohort 2 (n = 34) received 76 Gy in 34 fractions (2.25 Gy/F) and 71.6 Gy in 28 fractions (2.65 Gy/F), respectively, to the prostate and seminal vesicles, while 25 patients in cohort 2 also received integrated elective lymph node irradiation (50.4 Gy). All patients were treated with helical tomotherapy, and daily image guidance was performed before each treatment. Acute toxicities were assessed with Radiation Therapy Oncology Group (RTOG)/European Organization for Research on Treatment of Cancer (EORTC) criteria. No significant difference was detected between the 2 cohorts in the incidence of acute toxicities. In cohort 1, the incidences of grade 1 and 2 genitourinary and gastrointestinal toxicities were 45.5% and 45.4%, respectively, and without grade 3 and 4 toxicities. In cohort 2, the incidences of acute grade 1 and 2 genitourinary and gastrointestinal toxicities were 47.1% and 55.9%, respectively, and grade 3 genitourinary toxicity (hematuria) was noted only in 1 patient. No significant difference was detected in the incidence of acute toxicities between the patients receiving integrated elective lymph node irradiation and those receiving irradiation to prostate and seminal vesicle in cohort 2. Univariate and multivariate analyses were performed with clinical parameters. Only the baseline weight was found negatively correlated with genitourinary toxicities at a weak level (relative risk = 0.946, 95% confidence interval 0.896-0.998], P = .043). This study shows that 2 hypofractionation regimens (76 Gy/34F and 71.6 Gy/28F) delivered with HT are well tolerated in older aged patients having prostate cancer without significant difference for acute toxicities between the 2 cohorts. Late toxicities and treatment outcomes for these patients are under investigation.
Introduction
According to global statistics, prostate cancer (PC) is the second most common cancer in men and the sixth cause of mortality with 85% of patients older than 65 years when diagnosed. 1 Initial treatment recommendation of PC includes surgery, androgen deprivation therapy (ADT), and radiation therapy (RT). External-beam radical RT plays an important role in PC treatment. Several studies have shown improved biochemical relapse-free survival and freedom from distant metastasis with escalated dose. 2,3 National Comprehensive Cancer Network (NCCN; 2014) recommends a dose of 75.6 to 79.2 Gy in conventional fractionation to the prostate for low-risk cancer and higher than 80 Gy for intermediate- and high-risk cancer.
Conventionally fractionated RT is delivered with 1.8 to 2 Gy fractional dose. However, hypofractionated RT is a more efficient dose delivery regimen with increased fractional dose. There are still controversies on the α/β value for PC. Recent studies have shown a lower α/β value (1.4-3.1 Gy) for PC than for most cancers, 4 –8 even lower than the surrounding late-responding organs at risk (OARs). This indicates that PC would be more responsive to the size of fractional dose rather than the total dose. Due to this radiobiological feature, the hypothesis is that hypofractionation would yield better local control than conventional fractionated RT without increasing the risk of treatment-related toxicities. In addition, there is benefit in improving medical resource use and convenience for patients. On the other hand, some researchers argued that the above-mentioned studies might have neglected some relevant factors, and the α/β value could be risen up to higher than 4 Gy. 8 –10 As most published studies suggested, we used a lower α/β value in this study (3 Gy).
However, by increasing the fractional dose, the error of each treatment would result in more severe mistake in consequence. Helical tomotherapy (HT; Accuray Incorporated, Sunnyvale, California) can form a sharp dose gradient at the edge of the target volume, which enables a high-dose delivery to the target volume and better sparing of the surrounding OARs; and daily megavoltage computed tomography (MVCT) image guidance is recommended to reduce interfractional errors of hypofractionated RT. 11 The aim of this study is to evaluate the feasibility and related acute toxicities of hypofractionated HT in older aged patients with PC.
Materials and Methods
Patients
This was a single-institution, prospective, phase I-II clinical trial, registered with number ChiCTR-ONC-13004037. The research ethics board of the Chinese PLA General Hospital approved the study, and all eligible patients provided written informed consent.
Eligible patients were older than 65 years and had histologically confirmed PC. All patients were recruited in chronological order, 33 patients were recruited to the cohort 1 from February 2009 to July 2011, and 34 patients were recruited subsequently from July 2011 to February 2014 to the cohort 2. Risk classification was established according to the NCCN: low risk (clinical state T1-T2a, Gleason score 2-6, prostate-specific antigen [PSA] < 10 ng/mL), intermediate risk (clinical stage T2b-T2c or Gleason score 7 or PSA 10-20 ng/mL), high risk (T3a or Gleason score 8-10 or PSA > 20 ng/mL), and very high risk (T3b-T4). Exclusion criteria included distant metastasis, lymph node involvement, previous prostate surgical operation, previous pelvic RT, active collagen vascular disease, active inflammatory bowel disease, or a hip prosthesis. Pretreatment evaluations included the patient’s history, physical examination, staging investigations including whole-body bone scan, chest CT, abdominal ultrasound, pelvic magnetic resonance imaging (MRI), blood work including PSA determination, and liver function tests.
Patients in cohorts 1 and 2 were treated with 76 Gy in 34 fractions (2.25 Gy/F) and 71.6 Gy in 28 fractions (2.65 Gy/F), respectively. Table 1 shows the clinical data of the 2 groups. Patients at intermediate risk, high risk, or very high risk received neoadjuvant ADT for 3 months and concurrent ADT with irradiation, after which patients at high risk or very high risk continued ADT for a total duration of 2 to 3 years. Clinical evaluation and PSA measurements were scheduled every 3 to 4 months in the first 2 years and twice a year thereafter. A complete examination including bone scan and pelvic MRI was recommended for increasing PSA levels and/or clinical signs.
Patient Characteristics.

Abbreviations: PSA, prostate-specific antigen; CI, confidence interval.
Radiation Therapy
All patients underwent CT scan simulation in the treatment position (supine, arms crossed on forehead, and immobilized by thermoplastic mask). Plain and contrast-enhanced axial images were obtained from the lower level of L3 to proximal femur at 3-mm intervals.
The target volumes and OARs were contoured by radiation oncologists. Clinical target volume (CTV) 1 included the entire prostate gland and the seminal vesicles (SVs). The CTV2 included the periprostatic, obturator, external, and internal iliac lymph nodes, with upper bound of the lower level of S1. Planning target volumes (PTVs) were defined as CTVs plus a 5-mm margin in all directions except anterior and posterior to the prostate, in which the margins were 3 mm. The margins were modified to avoid high-dose irradiation of the rectum and bladder. The OARs included the bilateral femoral heads, bladder, and rectum. All images and volume structures were then transferred to the workstation of the TomoTherapy Hi-Art Treatment System for planning.
A single-phase treatment plan was generated by TomoTherapy Hi-Art 2.2.4.1 workstation using plain CT images. The plan required that the prescription dose covers at least 95% of the PTV. All patients in cohort 1 received a dose of 76 Gy in 34 fractions to PTV1 and no patient received elective lymph node irradiation. The dose-volume constraints for OARs were as follows: femoral head V50 = 0%, bladder and rectum V40 ≤ 40%, and bladder and rectum V65 ≤ 20%. All patients in cohort 2 received a dose of 71.6 Gy in 28 fractions to PTV1. Patients with a risk of lymph node involvement of >15% according to Roach et al 12 received 50.4 Gy in 28 fractions to PTV2. The dose–volume constraints for OARs were as follows: femoral head V50 = 0%, bladder and rectum V40 ≤ 40%, and bladder and rectum V60 ≤ 20%. A field width of 2.5 cm was used for all patients. The plans were delivered after having been approved by senior radiation oncologists. A MVCT study was taken before each treatment. After the correction of the patient’s setup errors with an automatic bone alignment, a manual soft tissue alignment was performed to correct any position errors of the prostate gland.
Acute toxicities were assessed weekly during RT and 3 months after treatment. Acute toxicity was defined as toxicity occurring within 90 days from the end of RT. After 90 days, any adverse events were classified as late toxicity. The toxicity was measured according to the RTOG/EORTC scale. The frequency of nocturia and defecation was recorded at each visit. D value was defined as the frequency difference between the most serious nocturia or defecation during acute period and the pretreatment condition.
Statistical Analyses
All data analyses were performed using IBM Statistical Package for Social Sciences, Version 20.0. We used Pearson chi-square test or Fisher test in bivariate analysis of the 2 groups and t-test or Mann-Whitney test for continuous variables. Logistic regression was performed to analyze correlations among clinical parameters (only the parameters with P < .15 in the univariate analysis to exclude those with the weakest correlation with acute toxicities) and acute toxicities. Mean values in our study were indicated with 95% CIs. Level of statistical significance was P < .05.
Results
Sixty-seven eligible patients with PC were treated between 2009 and 2014 in our center. The distributions of different risks were comparable in cohorts 1 and 2 (Table 1). The median follow-up in cohorts 1 and 2 was 53 months (range, 33-66 months) and 18 months (range, 2-33 months), respectively. The median pretreatment PSA levels of arm 1 and arm 2 were 14.95 ng/mL (range, 2.19-109.3 ng/mL) and 22.4 ng/mL (range, 1.3-118 ng/mL), respectively.
The average durations of RT of the 2 cohorts were 49.1 days (95% CI, 47.6-50.5 days) and 40.5 days (95% CI, 39.5-41.6 days), respectively. The treatment duration of cohort 2 was shorter by 17.5% compared to cohort 1. The distribution of acute toxicities is shown in Table 2. Among the patients in cohort 1, more than half of the cases did not experience any genitourinary (GU) or gastrointestinal (GI) toxicities; and no grade 3 and 4 events were noted. Among the patients in cohort 2, 50.0% and 44.1% did not experience any GU and GI toxicities, respectively. The grade 1 or 2 acute toxicities were all well tolerated, and no patients required medication. Grade 3 GU toxicity (hematuria) was noted in 1 patient, without any other grade 3 and 4 toxicities. All acute toxicities decreased 1 month after the end of RT and no grade 2 or higher toxicities were noted at 3-month follow-up. No significant differences were detected between the 2 cohorts in the incidence of toxicities and the D values. The majority of the patients did not lose weight. Fourteen (42.4%) patients in cohort 1 and 18 (53%) in cohort 2 experienced no weight change during RT.
Acute Toxicities.

Abbreviations: GU, genitourinary; GI, gastrointestinal; D value, the frequency difference of nocturnal enuresis or bowel movement at the end of radiation therapy and the baseline; CI, confidence interval.
In cohort 2, 25 patients received integrated elective lymph node irradiation. The incidence of grade 0, 1, 2, 3, and 4 acute GU toxicities were 40%, 52%, 4%, 4%, and 0%, respectively; and the incidence of grade 0, 1, 2, 3, and 4 acute GI toxicities were 36%, 52%, 12%, 0%, and 0%, respectively. Nine patients in cohort 2 received prostate and SV irradiation alone. In this subgroup, the grade 0, 1, 2, 3, and 4 acute GU toxicities were 77.8%, 11.1%, 11.1%, 0%, and 0%, respectively; the grade 0, 1, 2, 3, and 4 acute GI toxicities were 66.7%, 33.3%, 0%, 0%, and 0%, respectively. Mild weight change was noted in patients with or without elective lymph node irradiation. As shown in Table 3, no significant difference was detected between these 2 subgroups.
Acute Toxicities in Subgroups of the Cohort 2.
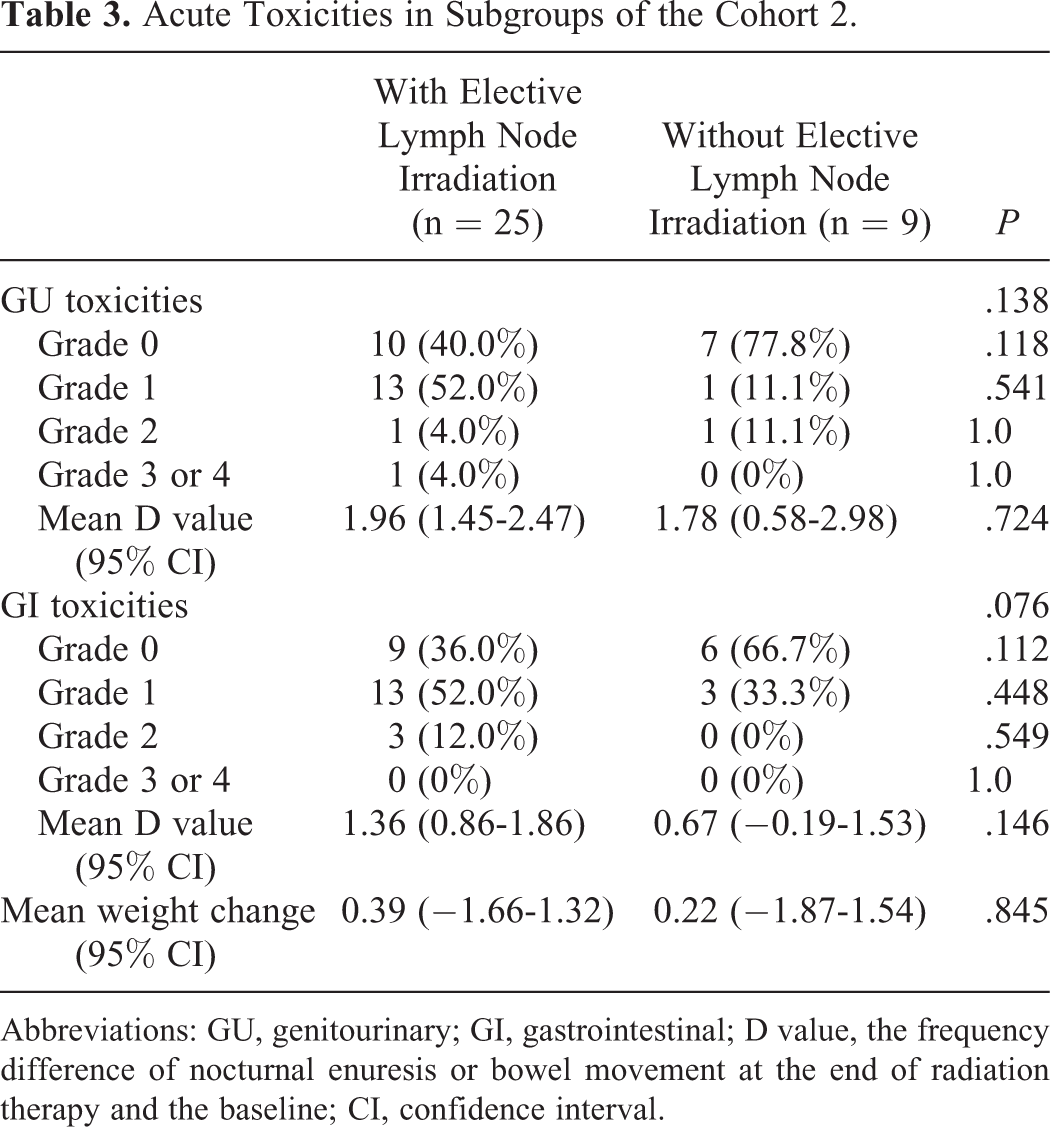
Abbreviations: GU, genitourinary; GI, gastrointestinal; D value, the frequency difference of nocturnal enuresis or bowel movement at the end of radiation therapy and the baseline; CI, confidence interval.
At 3-month follow-up, the PSA level dropped back to normal in all patients except 1, who developed bone metastasis only 4 months after RT and died of cerebral hemorrhage 2 months later.
Tables 4 and 5 show the results of univariate analysis and multivariate logistic regression, respectively. The clinical parameters included age, baseline weight, baseline PSA, Gleason score, clinical stage, elective lymph node irradiation, and dose regimens. Only 1 parameter, baseline weight, was found to be negatively correlated with GU toxicity at a weak level (relative risk [RR] = 0.946, 95% CI: 0.896-0.998, P = 0.043), which indicated that higher weight may lead to a decrease in GU toxicities. No parameter was found to be associated with GI toxicity.
Univariate Analysis for Prognostic Factors of Acute Toxicities.
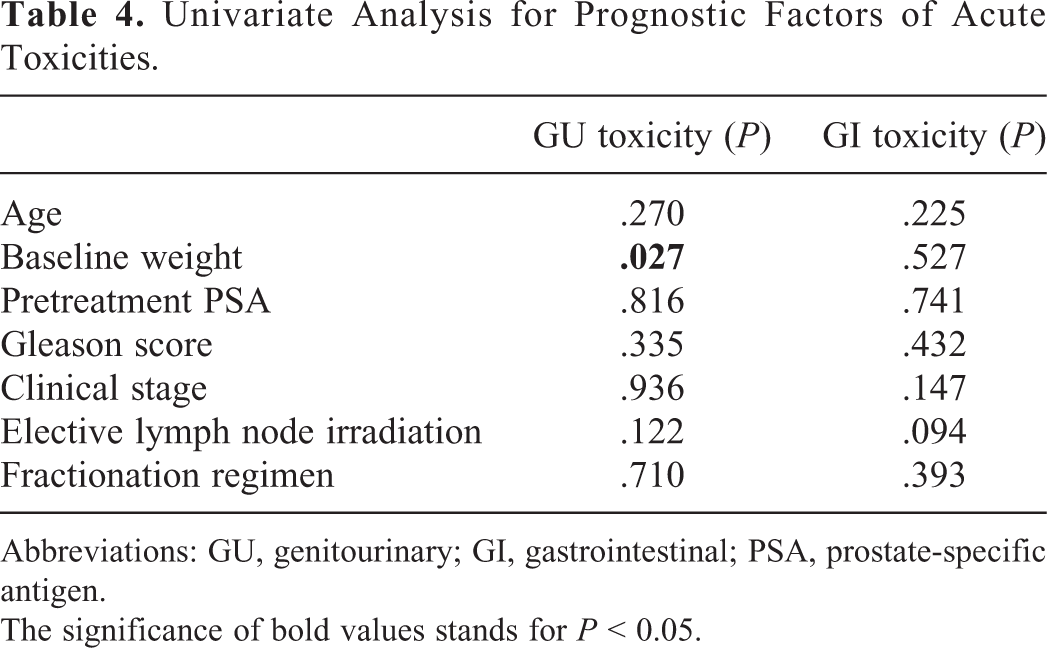
Abbreviations: GU, genitourinary; GI, gastrointestinal; PSA, prostate-specific antigen.
The significance of bold values stands for P < 0.05.
Multivariate Logistic Regression Analysis for Prognostic Factors of Acute Toxicities.

Abbreviations: GU, genitourinary; GI, gastrointestinal; CI, confidence interval.
The significance of bold values stands for P < 0.05.
Discussion
Intensity-modulated radiation therapy (IMRT) is considered the current standard treatment of PC. In this study, all patients were treated with HT, a special form of IMRT which can produce a well-distributed dose in the PTV with effective sparing of OARs and can, therefore, reduce the incidence of side effects, as shown by a number of studies. 13 –16 However, the sharp gradient of dose at the margin of the PTV can be a double-edged sword. The deviations that may happen in daily treatments require a certain expansion of CTV to guarantee effective target coverage. This may lead to dose escalation to the bowel and bladder, and finally result in an increase in toxicities. To resolve this problem, daily imaging is believed to be essential in PC RT, and HT can provide daily fan beam MVCT guidance for precise target localization to reduce variation and improve the accuracy of dose delivery. 13,16 Zelefsky et al have shown that image guided high-dose IMRT is associated with an improvement in biochemical tumor control among high-risk patients with PC and a lower rate of late urinary toxicity compared with high-dose IMRT without image guidance. 17
In 1999, Brenner and Hall reported for the first time a low α/β value of 1.5 Gy (95% CI: 0.8-2.2 Gy) in PC. 7 Similar results have been presented in several studies recently. 4 –6 Although some researchers hold different opinions, such as when the proliferation and hypoxic tumor cells were taken into account, the α/β value would rise to 3.1 Gy or even higher, 8,9 most studies had shown a lower α/β value in comparison to late reacting OARs (3-5 Gy). This biological feature leads to a higher fractionation sensitivity compared to other malignant tumors, and there will also be a beneficial aspect to applying hypofractionation to improve patient convenience and to reduce health care costs. In this study, we compared 2 hypofractionation regimens, assuming an α/β value of 3 Gy for PC. The biologically effective dose (BED) reached 132.7 Gy in both groups. This dose regimen is equivalent to a conventional fractionation regimen of 82.9 Gy in 46 fractions, 1.8 Gy per fraction.
Two early randomized trials have compared a hypofractionation regimen with conventional fractionation using a 2-dimensional conventional RT (2DCRT) technique, and with the limits of technology, the hypofractionation regimens failed to achieve a favorable tumor control probability. 18 –21 Better tumor control and low toxicity with higher-BED hypofractionation regimens, realized with 3-dimensional conformal RT (3DCRT), were reported in several randomized trials. 22 –25 Several phase III studies showed that dose escalation was worthwhile in terms of local or biochemical control for PC. 26 –36 The meta-analysis of Viani et al showed that high-dose RT was superior to conventional-dose RT in preventing biochemical failure in low-, intermediate-, and high-risk patients with PC. 37 There is no doubt that IMRT achieves better dose distribution in the target and better sparing for OARs compared to 2DCRT or 3DCRT and therefore can increase the dose to the target, increasing the tumor control probability. Several published IMRT-based hypofractionation studies reported their data on acute toxicities, most of them showing tolerable and comparable toxicities to conventional fractionation. The RTOG-0126 study showed that IMRT was associated with a significant reduction in grade 2 or greater GU and/or GI acute toxicity compared to 3DCRT, and there was a trend toward a clinically meaningful reduction in grade 2 or greater GI late toxicity with IMRT. 38 Three phase III IMRT-based studies showed GU and GI toxicities, especially late toxicities, with hypofractionated regimens comparable to conventional fractionation. 39 –42
The distribution of acute toxicities is presented in Table 2, without a statistically significant difference between the 2 cohorts. And meanwhile, acute toxicities were well tolerated, with only one grade 3 event, indicating that the 71.6 Gy/28F regimen was as safe as the 76 Gy/34F regimen. The GI symptoms mainly increased the frequency of bowel movements or tenesmus, grade 1 toxicities not requiring medication, and patients suffering from grade 2 GI toxicities being given antisymptomatic treatments. Only 1 patient in cohort 2 developed grade 3 GU toxicity as hematuria with grade 2 leucopenia during treatment, but the nocturia did not worsen as compared to the pretreatment state. This solitary case was not enough to demonstrate a correlation between the increased fractional dose and toxicity. We believe that a larger sample would be more revelatory. One of the published hypofractionation trials was similar to our schedule, Pollack et al 41 reporting the preliminary results of a multicenter phase III trial, which included 100 patients treated with IMRT technique in conventional (76 Gy/38F) or hypofractionation (70.2 Gy/26F) regimens. The distribution of grade 2 acute GU toxicities was 54% versus 40%, and that of grade 3 acute GU toxicities was 2% versus 8%, respectively. The distribution of grade 2 acute GI toxicities was 8% versus 18%, respectively, with no grade 3 toxicities in both cohorts. The difference didn’t reach a significant level. They indicated that there was a slight but not significant increase in GI toxicities during weeks 2, 3, and 4. However, the toxicities were considered to be tolerable.
With the precise technique of IMRT, and especially HT, hypofractionated RT using a simultaneously integrated boost to the prostate and SVs in combination with elective pelvic nodal irradiation is feasible. However, the benefit of prophylactic irradiation of pelvic lymph nodes in intermediate- and high-risk patients with PC is still controversial. The results from 2 phase III trials comparing whole pelvic RT (WPRT) and prostate-only RT did not show long-term advantages in progress-free survival (PFS) or overall survival when using WPRT, although 4-year PFS was higher in the patients with WPRT in the RTOG-9413 study. 43 –45 The RTOG 0924 is recruiting patients, and we hope it provides better answers. In cohort 2 of this study, 25 (73.5%) patients at greater than 15% risk of lymph node involvement according to Roach et al 12 received 50.4 Gy in 28 fractions to elective lymph nodes. Statistical analysis did not detect a correlation between node irradiation and incidence of acute GU or GI toxicities. However, with a median follow-up of 80 months (range, 72-87 months) in cohort 1, no pelvic node relapse occurred. Three patients developed bone metastases: 1 had a metastasis in a lumbar vertebra 1 year after RT and died of chronic obstructive pulmonary disease a year later; another patient had multiple metastases in vertebrae 4 months after RT and died of a cerebral hemorrhage soon after; and the last patient had sacral and femoral metastases 39 months after RT and developed a lung metastasis 3 months later. One patient had a biochemical failure with elevated PSA from 0.6 to 4 ng/mL but without clinically detectable locoregional recurrence or distant metastasis.
As shown by published prospective studies, hypofractionated IMRT with pelvic irradiation and simultaneous integrated boost to the prostate and SVs is feasible with low rates of grade 3 or greater acute toxicities if the fractional dose is less than 3 Gy or the BED3 is less than 130 Gy (Table 6). As compared to the results of the published prospective hypofractionation trials, our study yielded a similar or favorable outcome in acute toxicities with possible reasons being: (1) the margins from CTV to PTV were larger than 5 mm in most of the other studies, mainly around 8 mm. According to our experience, the margin from CTV to PTV can be narrowed to 5 mm when daily image guided radiation therapy (IGRT) is performed, similar to the result of Iwama et al. 13 (2) The patients’ treatment position was daily corrected by IGRT, which was based on the position of the prostate gland, to avoid excessive irradiation to the rectum and bladder. Accurate RT with IMRT and IGRT techniques enables us to reduce the incidence of acute toxicities; however, a larger sample and longer term follow-up are needed for further assessment not only of late toxicities but also of treatment outcome. No consensus exists on the most efficient treatment schedules. Various regimens have been used in clinical trials. In this study, we observed favorable toxicities with 2 hypofractionation regimens. This encourages us to increase the fractional dose in a further trial in order to find out the most efficient yet safe hypofractionation regimen for PC.
Published Prospective Clinical Trials of Hypofractionated IMRT for Prostate Cancer and Acute Toxicities.
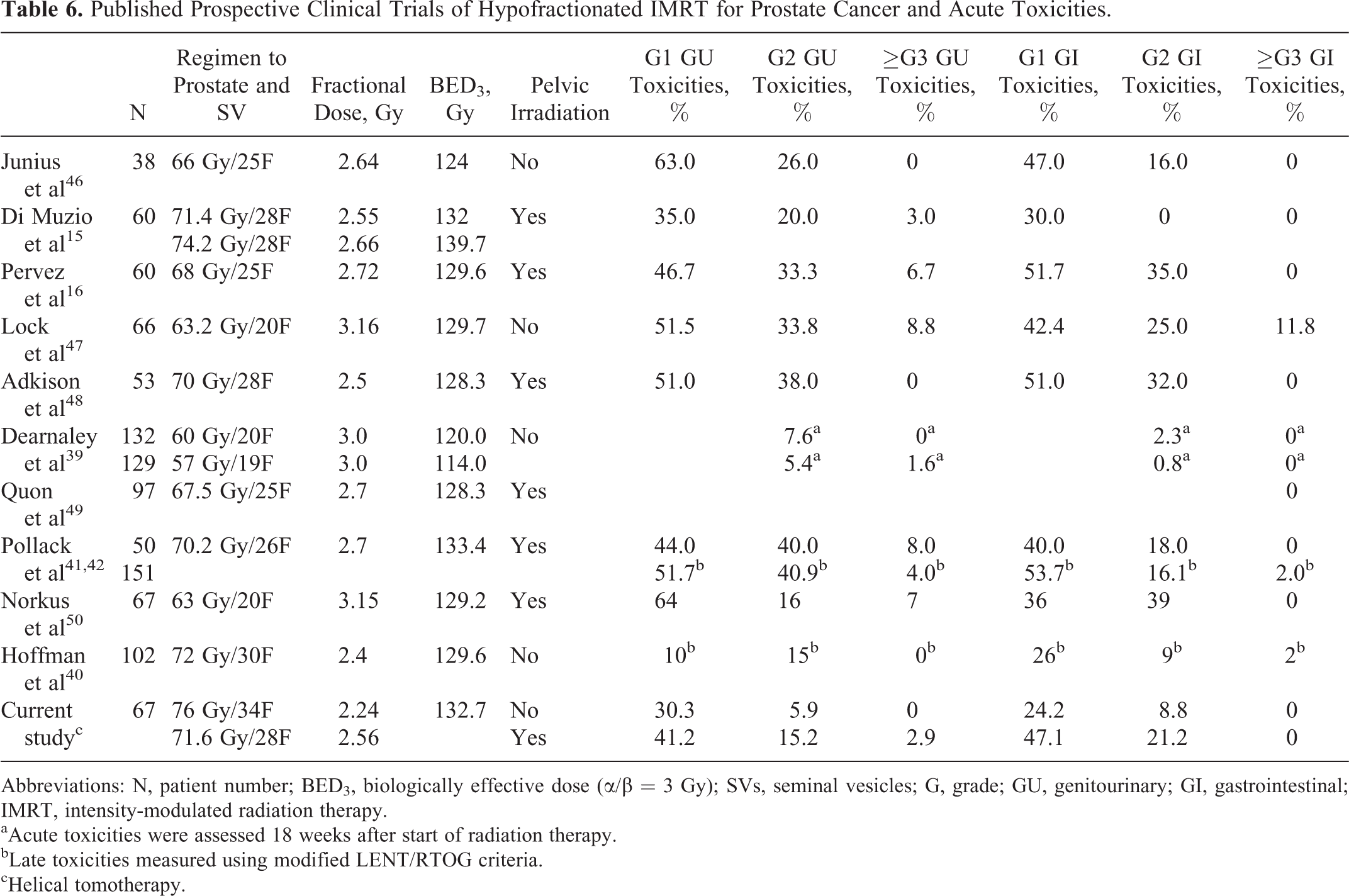
Abbreviations: N, patient number; BED3, biologically effective dose (α/β = 3 Gy); SVs, seminal vesicles; G, grade; GU, genitourinary; GI, gastrointestinal; IMRT, intensity-modulated radiation therapy.
aAcute toxicities were assessed 18 weeks after start of radiation therapy.
bLate toxicities measured using modified LENT/RTOG criteria.
cHelical tomotherapy.
Clinical and treatment factors influencing the risk of acute toxicities in this study are summarized in Tables 4 and 5. The only factor found to be related to GU toxicity was higher baseline weight correlating with reduced GU toxicities. However, as it is only a weak correlation with a RR > 0.9, a larger sample study would provide more information. Similar results were shown by Viani et al 37 and Guckenberger et al. 51 None of the factors, such as hypofractionation treatment, whole pelvic irradiation, ADT, age, PTV, and rectum/bladder volume, and so on was found significantly related to acute toxicities. Nowadays, age remains the major predictor of eligibility for curative treatment of localized PC, men aged 70 to 79 years having a significant 5-fold increased risk of not receiving curative treatment compared with men aged 60 to 69 years, as shown by de Camargo Cancela et al in a population-based study. 52 Some studies indicated that older age was related to the incidence of acute and late bowel toxicities following external-beam RT for PC as shown by Hamstra et al, 53 however, IGRT and IMRT were associated with lower rate of severe rectal toxicity than 3DCRT. In the study of Longobardi et al, although acute bowel toxicity after WPRT HT with integrated prostate or prostatic bed boost was associated with larger nodal CTV and older age, severe toxicity was mild and relatively rare, 54 as shown in this study. Because of shorter life expectancy and higher incidence of comorbid illness, there are quite a number of older aged patients who do not benefit from curative therapy. However, lack of radical treatment is still an important factor that may increase recurrence and distant metastases, and as older age predicts less aggressive PC and decreased metastasis, local radical treatment becomes essential in the control of PC for older aged patients. 55
The present study is only the preliminary results of a phase I-II trial, with favorable outcomes of acute toxicities of hypofractionated IMRT for older aged patients with PC. As the follow-up is short, especially in cohort 2, late toxicities and survival parameters should be observed for the next step. As the moderate hypofractionation regimens were well tolerated in this preliminary research, a new regimen with larger fractional dose will be considered.
Footnotes
Authors’ Note
Hai-Xia Liu participated in acquisition of data, performed the statistical analysis, and drafted the manuscript. Lei Du, Wei Yu, and Bo-Ning Cai participated in acquisition of data. Shou-Ping Xu and Chuan-Bin Xie contributed to data analysis. Lin Ma was responsible for study conception and design, participated in acquisition of data, and revised the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.