
Abstract
Stereotactic radiation technique including single fraction radiosurgery and conventional fractionated stereotactic radiotherapy is widely reported as an effective treatment of pituitary adenomas. Because of the restricted radiation tolerance dose of the optic pathway, single fraction radiosurgery has been accepted for small tumor located far away from the optic apparatus, while fractionated stereotactic radiotherapy may be suitable for larger tumor located close to the optic pathway. More recently, hypofractionated stereotactic radiotherapy has become an alternative treatment option that provides high rate of tumor control and visual preservation for the perioptic lesions within 2 to 3 mm of the optic pathway. The objective of the study was to analyze the clinical outcomes of perioptic pituitary adenomas treated with hypofractionated stereotactic radiotherapy. From 2009 to 2012, 40 patients with perioptic pituitary adenoma were treated with CyberKnife robotic radiosurgery. The median tumor volume was 3.35 cm3 (range, 0.82-25.86 cm3). The median prescribed dose was 25 Gy (range, 20-28 Gy) in 5 fractions (range, 3-5). After the median follow-up time of 38.5 months (range, 14-71 months), 1 (2.5%) patient with prolactinoma had tumor enlargement, 31 (77.5%) were stable, and the remaining 8 (20%) tumors were smaller in size. No patient’s vision deteriorated after hypofractionated stereotactic radiotherapy. Hormone normalization was observed in 7 (54%) of 13 patients. No newly developed hypopituitarism was detected in our study. These data confirmed that hypofractionated stereotactic radiotherapy achieved high rates of tumor control and visual preservation. Because of the shorter duration of treatment, it may be preferable to use hypofractionated stereotactic radiotherapy over fractionated stereotactic radiotherapy for selected pituitary adenomas immediately adjacent to the optic apparatus.
Keywords
Introduction
There are various treatment options for pituitary adenomas including surgery, medical treatment, and radiation. Radiation therapy is often reserved for patients who have tumors that are not controlled successfully with surgical or medical treatment. It is also considered for medically or surgically inoperable patients. Stereotactic radiation technique including single fraction radiosurgery (SRS) or conventional fractionated stereotactic radiotherapy (FSRT) is widely reported as an effective treatment of pituitary adenomas. However, SRS and FSRT are selected for use in different clinical situations that depend mainly on the restricted tolerance dose to the optic pathway. 1 Thus, SRS is unsuitable for tumors located very close to the optic pathway, while FSRT is commonly used in large tumors adjacent to the optic apparatus. Moreover, with the use of older frame-based SRS/FSRT technique, some disadvantages are mentioned, not only the pin site-related morbidity, not practical for multisession treatment and unable to treat extracranial disease, but also the longer treatment time in conventional fractionation schedules (20-25 fractions). More recently, hypofractionated stereotactic radiotherapy (HSRT) with frameless radiosurgery system has become an attractive alternative treatment option that can eliminate the aforementioned disadvantages in frame-based stereotactic system. In Thailand, the first frameless CyberKnife (CK) robotic radiosurgery machine was installed in our institute in 2009. To improve the treatment outcome and patients’ satisfaction while maintaining low rate of optic neuropathy, we started protocol-based HSRT for perioptic pituitary adenoma using CK. The aim of this study was to analyze the outcome regarding tumor control, visual preservation, hormone response, and toxicity of HSRT using CK for perioptic pituitary adenoma in our hospital.
Materials and Methods
Patients
This study was approved by our institutional review board. Informed consent was obtained from all patients. Before treatment, all patients were analyzed and approved by our radiosurgery board. Eligibility criteria for HSRT protocol were as follows: (1) perioptic pituitary adenoma defined from the tumor located within 2 mm of the optic apparatus as determined by magnetic resonance imaging (MRI), (2) recurrent or residual after maximum resection, (3) surgically or medically inoperable, and/or (4) patient preference.
From January 2009 to December 2012, a total number of 40 consecutive patients having perioptic pituitary adenoma treated with HSRT using CK were included in this study. Of the 40 patients, there were 16 (40%) males and 24 (60%) females, with the median age of 49.5 years (range, 26-68 years). Thirty-nine (98%) patients had previously undergone surgery. Two (95%) patients previously received conventional radiation. Before undergoing HSRT, 11 (28%) patients experienced existing visual deficit and 33 (82%) received hormone supplement for hypopituitarism. Table 1 summarizes the baseline characteristics of this study.
Baseline and Treatment Characteristics of 40 Patients With Perioptic Pituitary Adenomas.a

Abbreviations: BED, biological effective dose; CK, CyberKnife; HSRT, hypofractionated stereotactic radiotherapy.
a HSRT by CyberKnife system.
CyberKnife model G4 (Accuray Inc, Sunnyvale, California) uses a 6-MV light-weight linear accelerator mounted on a fully articulated robotic arm. Multiplan (Accuray Inc) software was used for inverse planning. Patients were immobilized in the supine position with a thermoplastic face mask. Individual treatment planning was done at a workstation using an image set from a contrast-enhanced computed tomography (CT) scan, 1.25-mm slice thickness, with or without gadolinium-enhanced MRI. Gross tumor volume (GTV) and critical structure were delineated in each consecutive slice of CT and MRI. No additional margin was added from the GTV to obtain the clinical target volume and the planning target volume.
Hypofractionated stereotactic radiotherapy was delivered in 3 to 5 fractions, with the total dose of 20 to 25 Gy. Radiation dose was prescribed to the periphery of the lesion. Plans and isodoses were selected and prescribed individually in each patient. In our practice, we selected the prescribed isodose that ideally covers more than 95% of the target volume with no minimum isodose or tumor coverage imposed. Therefore, the tumor dose and prescribed isodose line might be different in each individual patient based upon the tumor subtype, size and shape of the tumor, tumor location, and individual physician preference. For example, if tumor was functioning subtype, physician might need more high dose or hot area inside the tumor so they selected the lower prescribed isodose line to produce higher dose within the tumor. However, when the dose delivered to the optic apparatus exceeded their tolerance dose, the prescribed dose was reduced. Radiation treatment was given once a day, consecutively 3 to 5 days in a week. The whole process of treatment planning was determined and finalized by a radiosurgery staff team consisting of neurosurgeons, radiation oncologists, and medical physicists. Prescribed dose, biological effective dose, and single-dose equivalent for commonly used dose schedules in our study are summarized in Table 2.
Prescribed Dose, BED Gy3, and Single-Dose Equivalent for Commonly Used Dose Schedules in Our Study.

Abbreviation: BED, biological effective dose.
Clinical Evaluation
After HSRT, all patients were routinely followed at 1, 3, 6, and 12 months during the first year. The interval of 6 to 12 months was continued thereafter. Magnetic resonance imaging was performed annually for the first 5 years and every 2 years thereafter. Tumor control was defined as the absence of radiologic tumor progression. Endocrine assessment with serum or urine tests was conducted by endocrinologists. Criteria for complete remission of functioning pituitary adenomas were defined as follows: (1) fasting growth hormone (GH) levels <2.5 ng/mL and normal insulin-like growth factor 1 level in acromegaly; (2) normalized adrenocorticotrophic hormone, cortisol levels, and urine-free cortisol level in Cushing disease; and (3) prolactin levels <20 ng/mL in prolactinoma.
Results
With the median follow-up of 38.5 months (range, 12-71 months), no patient died during this period. The median prescribed dose of 25 Gy (range, 20-28 Gy) in 5 fractions (range, 3-5) was used. The median prescribed isodose was 76% (range, 65%-85%). The median biological effective dose (BED) Gy3 was 66.7 Gy (range, 35-60 Gy). The median tumor volume was 3.35 cm3 (range, 0.82-25.86 cm3). The treatment characteristics are summarized in Table 1.
Tumor Control and Radiographic Response
After a median follow-up time, 39 (97.5%) patients experienced either smaller tumor (8 patients) or stable disease (31 patients), whereas 1 (2.5%) patient with prolactinoma developed tumor enlargement in the field of radiation. The patient was subsequently treated with transsphenoidal tumor removal and still alive without tumor progression at the last follow-up.
Vision
Eleven (28%) of the 40 patients experienced preexisting visual deficit, both visual acuity and visual field before HSRT. With the median clinical follow-up of 38.5 months (range, 12-71 months), vision was improved in 2 (18%) patients and remained stable in the rest. No patient developed newly vision deterioration after HSRT (Table 3).
Imaging and Vision Change After HSRT.

Abbreviations: ACTH, adrenocorticotrophic hormone; CR, complete remission; GH, growth hormone; HSRT, hypofractionated stereotactic radiotherapy; PR, partial remission; PRL, prolactin.
Hormonal Control
In our study, 13 patients with functioning pituitary adenoma were followed up for hormonal evaluation. Hormonal control to HSRT in the setting of concurrent medical therapy was analyzed. Seven (54%) of the 13 patients with functioning pituitary adenoma were recorded for hormone normalization. The median time to hormonal control was 28 months (range, 24-71 months). Seven patients had GH hypersecretion at baseline, whereas 4 (57%) patients had complete remission. The remaining 3 patients continued to have elevated hormone level and were further treated with medication until the last follow-up. Five patients with prolactinoma who had failed dopamine agonist therapy were treated with HSRT, and 2 (40%) patients experienced hormone normalization. Three patients did not experience remission, and 1 of them also had simultaneous enlargement of the tumor. Thus, she underwent salvage tumor removal, whereas the other 2 patients were continuously treated with medication.
Complications
At the last follow-up, there was no report of newly developed hypopituitarism, visual deterioration, or other significant morbidities.
Discussion and Conclusion
Stereotactic irradiation including SRS and FSRT has shown excellent results with low risks of complications in pituitary adenoma. The long-term results from previous studies of frame-based radiosurgery systems, both GammaKnife and Linac based, have been reported with the tumor local control (LC) rates ranging from 83% to 100%, and the new onset of hypopituitarism is between 0% and 40%, 2 –6 which is similar to the results of FSRT that reported 97% to 100% LC rate and 18% to 35% hypopituitarism rate. 7 –9 With the present data review, the risk of RION is unusual if the maximum dose to the optic apparatus is not beyond the tolerance dose limitation. Nowadays, the maximal dose for optic apparatus less than 55 Gy for conventional fraction and less than 8 Gy for single fraction is recommended. 1,10 In general practice, if tumor is located very close to the optic apparatus, SRS seems to be risky to the optic pathway. In this circumstance, FSRT is widely accepted. Although FSRT has been proven effective and safe for tumor close to the optic apparatus, 5 to 6 weeks of treatment schedule is inconvenient for many patients.
More recently, HSRT with frameless stereotactic radiosurgery system has become an attractive alternative treatment option for perioptic lesions located adjacent to the optic apparatus because this technique still maintains ability to treat the lesion close to the optic apparatus while providing the short treatment time (3-5 fractions). Because of the relatively new approach of HSRT in perioptic pituitary adenoma, the previous studies in these particular tumors are still limited. The aim of this study was to report and review the outcome regarding tumor control, visual preservation, hormone responsiveness, and toxicity of HSRT using CK for perioptic pituitary adenoma.
In 2009, our hospital installed the first robotic radiosurgery (CK) in Thailand. After that, we have developed the protocol for perioptic pituitary adenoma defined from the tumor located within 2 mm of the optic apparatus and treated with HSRT using CK. The prescribed dose of 25 Gy in 5 fractions (BED Gy3 = 66.7 Gy) was commonly used in most cases. However, the other prescribed dose was selected for use depending on individual’s physician consideration. For example, if a dose would expose critical structures to radiation beyond their tolerance, such as 25 Gy for optic pathway, a lower prescribed dose was selected. With this protocol, there was no excess dose delivered to the optic apparatus. This study has shown excellent results of HSRT for perioptic pituitary adenoma. The overall tumor control rate was 97.5% without vision deterioration and any severe late complication, which were comparable with 98% to 100% LC rates reported in previous studies. 7,11,12 Table 4 summarizes the LC rates from previous reports of perioptic pituitary adenoma treated with HSRT.
Summary of the Local Control Rates From the Previously Reported Studies of Pituitary Adenoma Treated With HSRT.
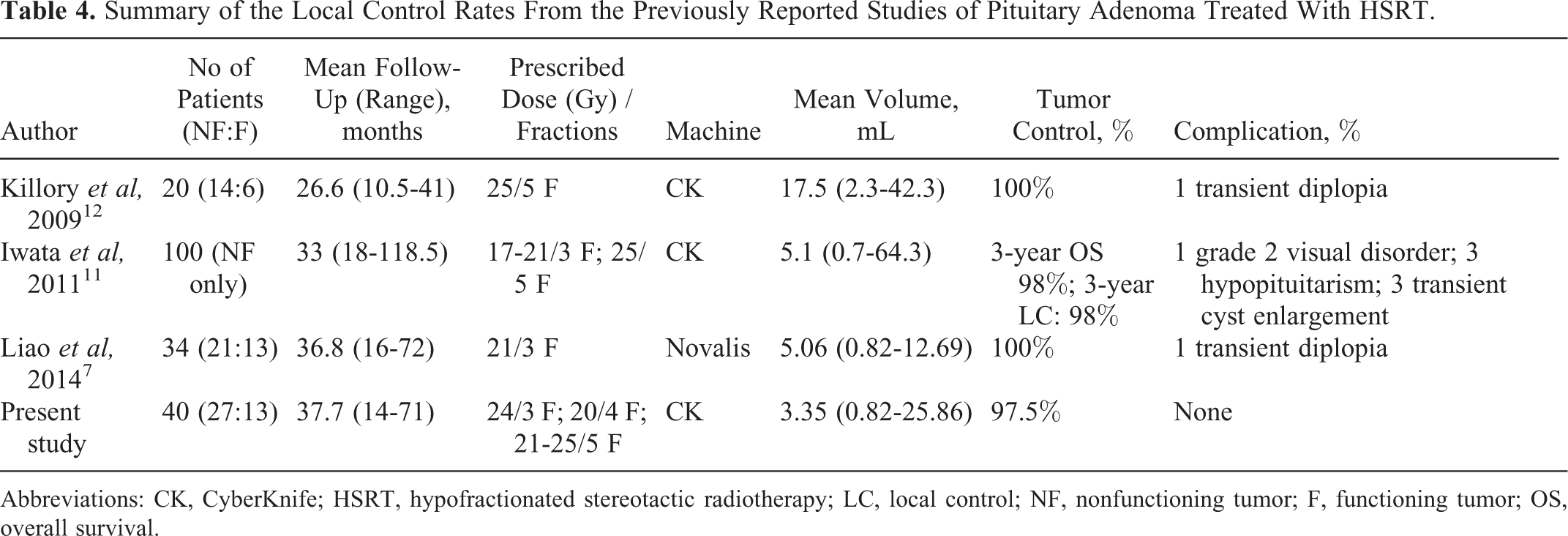
Abbreviations: CK, CyberKnife; HSRT, hypofractionated stereotactic radiotherapy; LC, local control; NF, nonfunctioning tumor; F, functioning tumor; OS, overall survival.
Although fractionation schedule seems to have no impact for LC, the impact on the rate of hormone normalization using different fractionation schedules is still debatable. Most series have demonstrated endocrine remission that varies widely between 5% and 63% 3,13 –15 after SRS treatment and from 20% to 42% following FSRT technique. 8,16 The 54% hormonal normalization rate observed in this study is similar to hormonal normalization rates reported in other HSRT published studies 7,11,12 and also comparable with SRS and FSRT techniques. Nevertheless, comparing hormonal normalization between various fractionations including SRS, HSRT, or FSRT is difficult because of the retrospective nature, nonrandomized comparative study, difference in baseline characteristics such as tumor volume and pretreatment hormone levels, and difference in the definition of hormonal normalization. A well-designed study with large number of patients for examining hormonal control rate with various fractionations is required.
The most complication of concern in perioptic tumor after HSRT is RION. The data from Quantitative Analyses of Normal Tissue Effects in the Clinic (QUANTEC) analysis determined for the optic apparatus have a dose tolerance in the range of 8 to 10 Gy for single fraction and 55 to 60 Gy for conventional fraction. From a recent study, if optic chiasm dose is not beyond their dose tolerance, a near-zero risk of RION is observed. 1 Because of a relatively new approach of HSRT in perioptic tumor, the dose tolerance of optic apparatus and the incidence of RION are still unknown. In general practice with HSRT, the accepted maximal tolerated dose to the optic apparatus is usually equivalent with tumor marginal dose. For example, the planned prescribed dose was either 21 Gy in 3 fractions or 25 Gy in 5 fractions, and the maximal dose at optic apparatus was usually not more than 21 Gy or 25 Gy in 3 to 5 fractions. 17 However, when the doses delivered to the optic apparatus exceed these levels, the prescribed doses were reduced. With this practice, the previous studies have consistently reported a very low rate of RION after HSRT. 7,11,12 Nevertheless, in the absence of radiation injury, a higher dose might not produce greater tumor and hormonal control over the longer term. Clearly, the long-term follow-up of a decade and beyond will guide us but how we know if we have optimized dosing already. Hypofractionated stereotactic radiotherapy provides not only the low incidence of RION but also the low rate of hypopituitarism. Stereotactic radiation technique has a theoretical advantage over conventional radiation therapy because it reduces target volume with rapid dose falloff outside the tumor volume, which ensures that less of the remaining pituitary and hypothalamus is exposed to radiation. From previous studies, the incident of hypopituitarism is >50% after conventional RT. 18,19 The hypopituitarism rate seems to be lower in SRS treatment which has reported less than 20% after SRS. 17 Our study reported no newly detected hypopituitarism after HSRT that is comparable to the previous reports. 7 However, our study is based on the analysis of chart review and not systematic regular checkup of hormone level. Therefore, the exact rate of new hypopituitarism may have been missed. In addition to the median follow-up time of 38 months, it might be too short to make the conclusion of no hypopituitarism happened after treatment.
This study showed excellent outcomes of CK HSRT using 25 Gy in 5 fractions in patients with perioptic pituitary adenoma (See Figure 1). To protect visual damage while providing short treatment time, HSRT seems preferable in tumors located within 2 to 3 mm of the optic apparatus. Further well-designed study with long-term follow-up is needed to evaluate especially for hormonal control and long-term complications such as RION, hypopituitarism, and radiation-induced malignancy.
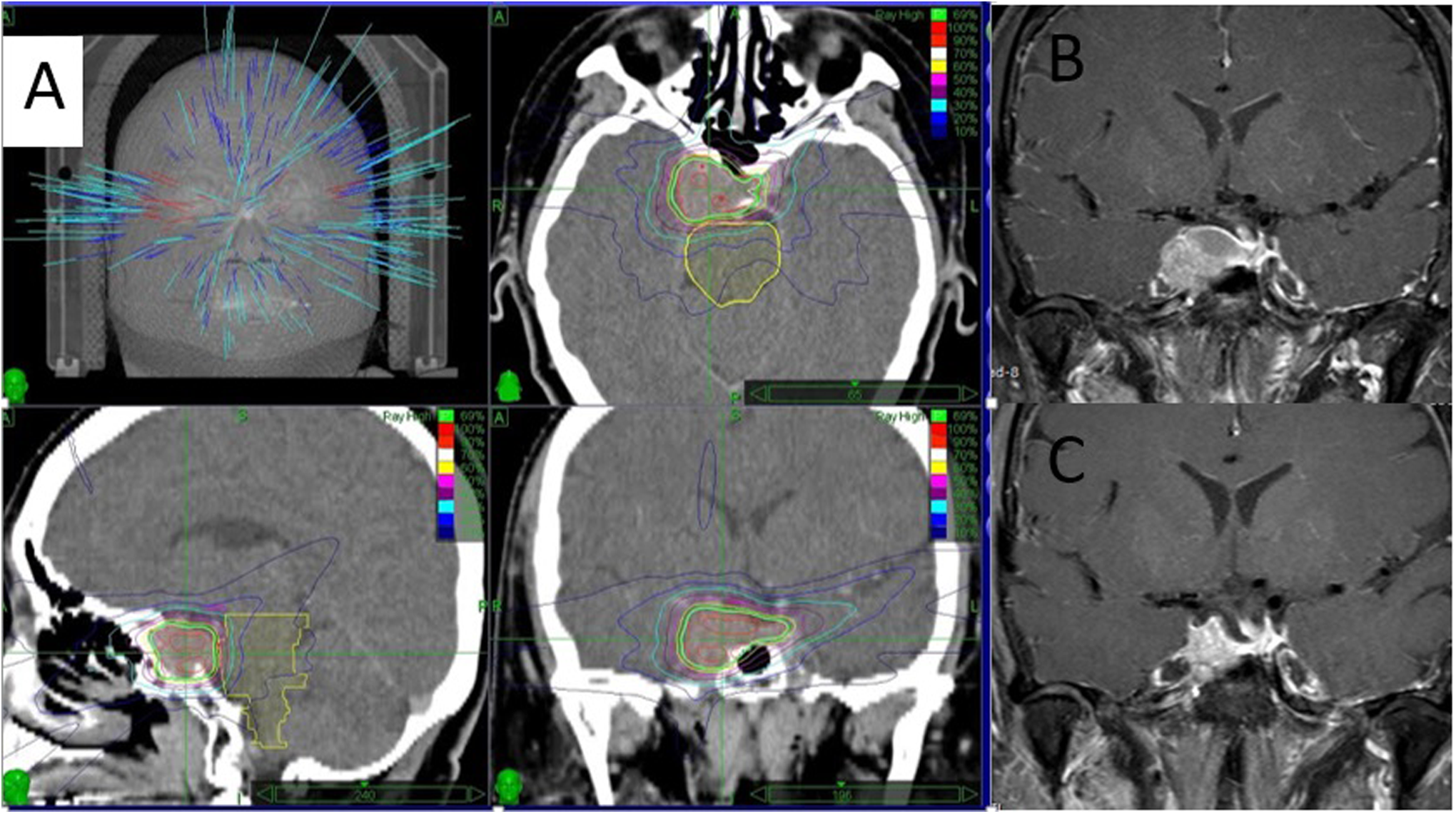
CyberKnife (CK) treatment planning (A), coronal magnetic resonance imaging (MRI) showing a residual pituitary adenoma in the right cavernous sinus adherent to the right optic nerve after transsphenoidal tumor resection (B), coronal 2-year follow-up MRI showing tumor shrinkage after CK (C). (A case from Ramathibodi Hospital with permisssion).
Footnotes
Acknowledgments
The authors thank Mr Prasert Assavaprathuangkulm and Mr Yothin Kumsang for his assistance in the database. Professor Amnuay Thithapandha helped edit the English language.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.