
Abstract
Stereotactic body radiation therapy in patients with spine metastases maximizes local tumor control and preserves neurologic function. A novel approach could be the use of stereotactic body radiation therapy with simultaneous integrated boost delivering modality. The aim of the present study is to report our experience in the treatment of spine metastases using a frameless radiosurgery system delivering stereotactic body radiation therapy–simultaneous integrated boost technique. The primary endpoints were the pain control and the time to local progression; the secondary ones were the overall survival and toxicity. A total of 20 patients with spine metastases and 22 metastatic sites were treated in our center with stereotactic body radiation therapy–simultaneous integrated boost between December 2007 and July 2018. Stereotactic body radiation therapy–simultaneous integrated boost treatments were delivered doses of 8 to 10 Gy in 1 fraction to isodose line of 50%. The median follow-up was 35 months (range: 12-110). The median time to local progression for all patients was not reached and the actuarial 1-, 2-, and 3-years local free progression rate was 86.36%. In 17 of 20 patients, a complete pain remission was observed and 3 of 20 patients had a partial pain remission (complete pain remission + partial pain remission: 100%). The median overall survival was 38 months (range 12-83). None of the patients experienced neither radiation adverse events (grade 1-4) nor reported pain flair reaction. None of the patients included in our series experienced vertebral compression fracture. Spine radiosurgery with stereotactic body radiation therapy–simultaneous integrated boost is safe. The use of this modality in spine metastases patients provides an excellent local control.
Introduction
Patients with cancer may have up to 40% of possibility to develop spinal metastases during the course of their disease. 1,2 However, in about 10% of the patients, they can represent the first clinical manifestation. Approximately 95% of the patients demonstrate epidural metastases (vertebral body and the pedicle regions), the 5% will be present with intradural, and less than 1% with intramedullary metastases. 3,4 Only 10% to 20% of the patients with spinal metastases will be alive for 2 years after the diagnosis. 5,6
Spinal metastasis is a complex condition that requires as therapeutic goals the palliation, the pain control, the spinal stability, the neurologic function maintenance, and the tumor control. The systemic treatments have improved providing extended life span in oncologic patients. The occurrence of spinal metastases in long-term survival patients encouraged the use of sophisticated treatment options, including stereotactic body radiation therapy (SBRT) and vertebroplasty. In this regard, the Spine Instability Neoplastic Score is one of the tools that provide a method for choosing between a surgical and alternative approach. 7,8
Pain is one of the most invalidating symptoms which occurs in more than 95% of patients with spinal metastases and it is present with specific characteristics: local, radicular, or mechanical pain. 9 Aggressive surgical techniques (ie, spondylectomy) permit to obtain adequate pain control and stability. 10,11 However, in patients with very limited life expectancy, vertebroplasty may be a valid alternative to control mechanical pain from vertebral body fractures in the absence of severe instability or spinal cord compression. 12 Radiation therapy has recently developed new promising tools (ie, intensity-modulated radiation therapy, volumetric arc therapy, and SBRT) to treat spine metastases. In particular, SBRT permits to deliver a higher dose for fraction to the tumor, significantly reducing the dose to the spinal cord. 13 -17 The primary goal of spine SBRT is to maximize local tumor control of the involved spine while preserving neurologic function. To date, in patients with very short life expectancy, the single fraction (8-10 Gy) 13 represent a valid alternative respect to 10 fractions of 3 Gy used in patients with better prognosis. 12
Hartsell et al reported no differences between the response of patients receiving 30 Gy in 10 treatment fractions and of those receiving 8 Gy in a single fraction, in terms of pain relief, narcotic relief, or pathologic fracture incidence. Overall, 89% of patients showed at least minimal relief of pain, with 53% obtaining complete relief and another 30% experiencing partial relief. 18
The use of advanced radiation techniques permits to deliver high dose with respect to the palliation. 19 Stereotactic body radiation therapy allows the use of different contouring approaches (whole vs partial vertebral) for body contouring and has a beneficial effect on the local in-field recurrence. 7 -11,20 Stereotactic body radiation therapy is widely employed in clinical practice but only a few data exist about its use in simultaneous integrated boost (SIB) modality. In our department, we deliver SBRT with SIB (SBRT-SIB) using a CyberKnife (Accuray Inc, Sunnyvale, California) system which permits to plan a heterogeneous dose. 21 -24 The use of high-dose radiation on the spine with SBRT can induce vertebral compression fractures (VCFs), 25 which are reported to develop more frequently (3% to 39%) than the more serious radiotherapy complication, that is, myelopathy (1% to 5%). 7 -11,20,26 Our hypothesis is that the use of hot spots on gross tumor volume (GTV) could decrease the risk of VCF and a dose of 8 Gy/1 Fx could be valid to treat whole vertebral body. 7 -11,20,26 This prompted us to report our experience on SBRT-SIB using a frameless radiosurgery system in patients with spine metastases.
Methods
Among all patients treated with SBRT for vertebral metastases in our center from December 2007 to July 2018, we have selected only patients treated with SBRT-SIB. Inclusion criteria were oligometastatic or oligorecurrent disease; life expectancy >6 months; no extradural spinal cord compression; <3 vertebral sites involved.
The primary end points were the pain control at the time of the last follow-up and the time to local progression (TTLP), which was defined as the imaging-based disease progression compared with the magnetic resonance imaging (MRI) or positron emission tomography-computed tomography (PET/CT) at the time of treatment. The secondary end points were the overall survival (OS) and toxicity according to National Cancer Institute Common Toxicity Criteria for Adverse Events (NCI CTCAE) version 4.0.
The study was approved by the local institutional review board: Comitato Etico Interaziendale della Provincia di Messina. Protocol Number: 61/19. Informed consent was obtained from the patients. 1. Imaging and treatment Treatments were delivered using the CyberKnife, an image-guided, frameless, LINAC-based, 6 MV radiosurgery system with Xsight Spine Tracking System for image-guided radiation therapy. The patients were immobilized with a vacuum bag for imaging acquisition and treatment. The pretreatment imaging consisted of a thin-section multiplanar reconstruction-gradient echo volumetric study conducted on a Siemens Magnetom 1.5 T MRI imaging system (Siemens, Erlangen, Germany), performed with the following parameters: repetition time 9.7 milliseconds, echo time 4 milliseconds, matrix 200 × 256, flip angle 1, orientation sagittal. A multislice body CT was also performed using a multislice scanner, Siemens Sensation 16 (Siemens). 2. Target, organ at risk delineation and treatment planning Manual contouring of the tumor and the critical volumes was performed on the coregistered MRI and CT data sets in the axial plane with simultaneous display of contours on reconstructed orthogonal images (Figure 1). The planning target volume (PTV) was delineated on the entire vertebrae of the involved levels with expansion of 1 mm in all direction and −1 mm in the cavitation around the spinal canal. The GTV was defined on the MR, CT, or PET-CT. The PTV-boost was outlined on a concept of anatomical target volume as a function of the topography of GTV and of the macroscopically involved elements of the vertebra (body, peduncles, transverse process, and spinous process; Figure 1). The PTV-boost plus PTV was used for SBRT-SIB prescription dose delivery. The spinal cord was contoured on the MRI. No spinal cord volume expansion was performed but the spinal canal was contoured on the CT images. Additional organs-at-risk were delineated in function of the anatomical districts (pharynx, esophagus, lungs, kidneys, bowel, etc). The Multiplan Treatment Planning System (Accuray Inc) was used for inverse planning. An inhomogeneous prescription in 1 fraction has been applied to create the hot spot of dose for the PTV-boost (SBRT-SIB).
21
-23
The hot spot was obtained with a prescription dose of 8 to 10 Gy to isodose line of 50% in order to obtain a PTV coverage of at least 95%. By tuning goals and constraints of the inverse planning, we were able to shift the whole dose from 16 to 20 Gy on the PTV Boost. 3. Patients assessment Follow-up imaging was based on our institutional practice, consisting of a full spine MRI study at 3-month intervals and PET/CT after 6 months. Time to local progression was defined as the time from treatment to a radiological documented disease progression in the treated spine using RECIST-Criteria (Revised Guidelines, Version 1.1, 2009).
27
The OS was defined as the duration from irradiation to patient death. The acute and late toxicity evaluations were performed according to NCI CTCAE version 4.0, 3 and the pain was assessed using the numeric rating scale (NRS). 4. Statistical data analysis and parameters Because of the relative rarity of spinal metastases requiring SBRT-SIB, we decided to accrue prospectively a consecutive series of patients during a period as long as 12 years to obtain a consistent population with precisely defined characteristics and homogeneously treated.
Estimates of TTLP and OS were calculated using the Kaplan-Meier method and the log-rank test was used to compare survival curves. Statistical tests were 2-tailed and a P value <.05 was considered statistically significant. All data were analyzed using the SPSS version 24.0 software package (IBM Corporation, Armonk, New York).
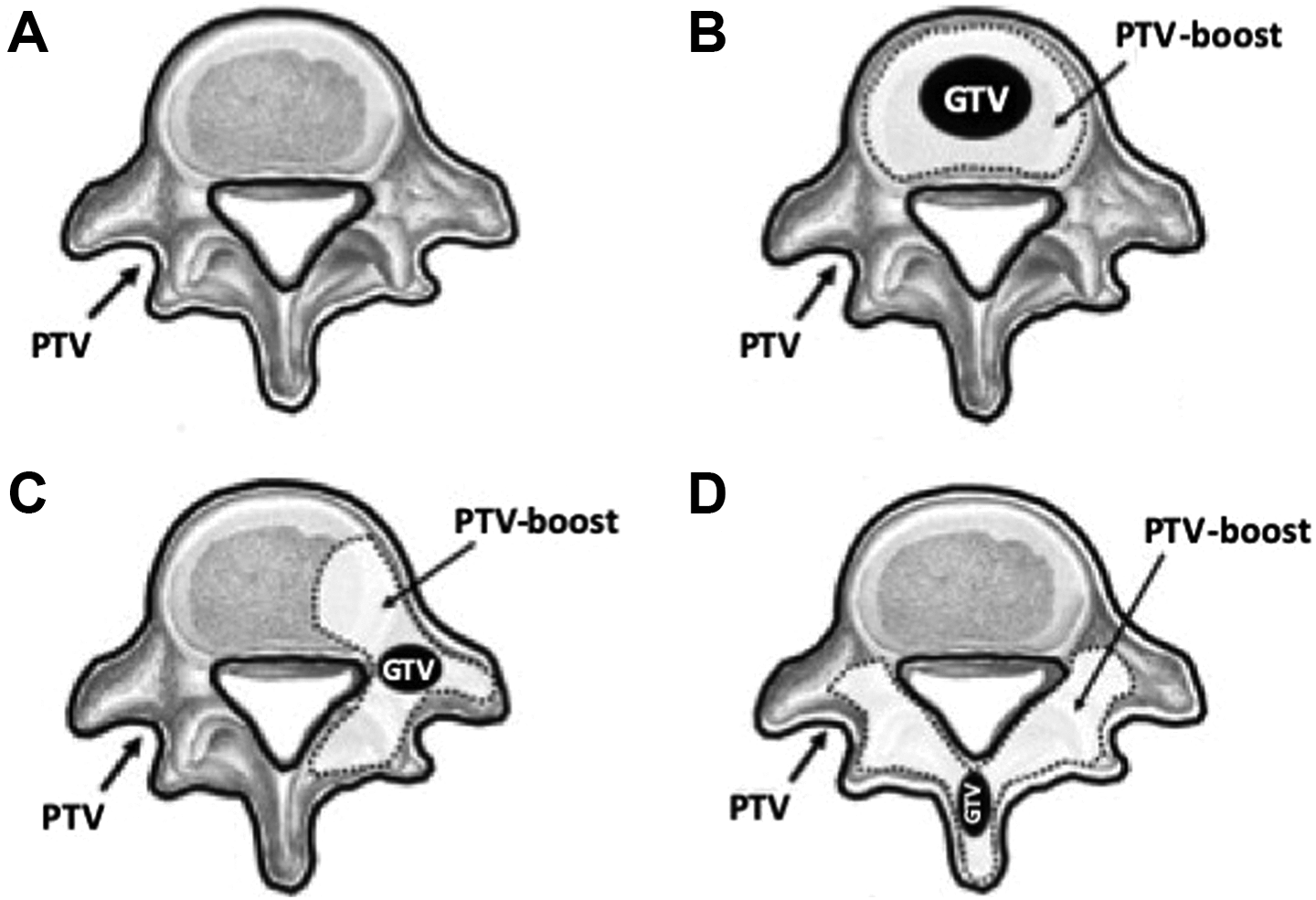
Concepts for the definition of PTV (A) and PTV-boost in relation to the topography of the GTV and of the likely micrometastatic disease (B, C, D). (B) GTV located in the vertebral body; (C) GTV located in the transverse process; (D) GTV located in the vertebral spinous process. GTV indicates gross tumor volume; PTV, planning target volume.
Results
A total of 20 patients with spine metastases and 22 metastatic sites were treated in our center with SBRT-SIB between December 2007 and July 2018. Clinical and main demographic characteristics of patients were summarized in Table 1. All patients were treated at the University Hospital of Messina, Italy. Details of treatment characteristics are shown in Table 2. The median follow-up was 35 months (range: 12-110).
Patients Characteristics.

Treatments Characteristics.
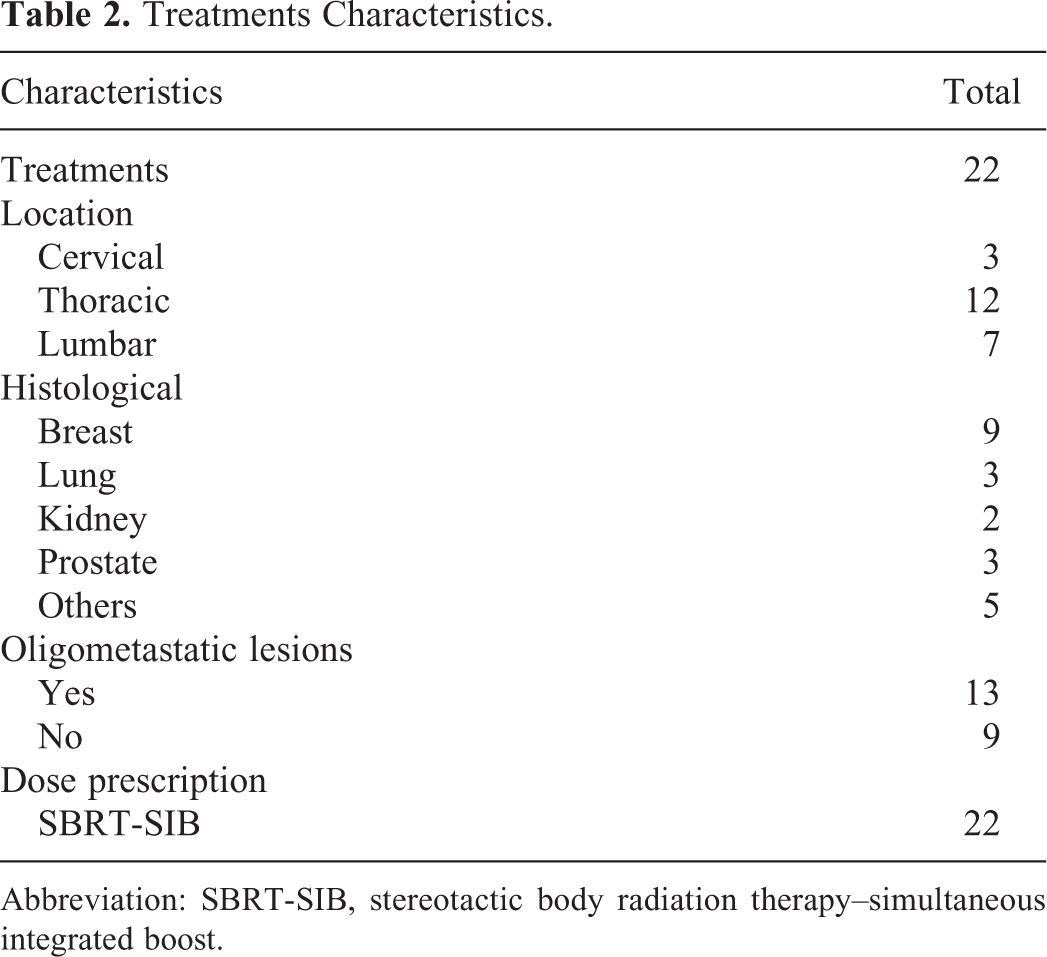
Abbreviation: SBRT-SIB, stereotactic body radiation therapy–simultaneous integrated boost.
Stereotactic body radiation therapy–simultaneous integrated boost treatments were delivered with doses of 8 to 10 Gy in 1 fraction to isodose line of 50% (D
max = 20 Gy; Median SIB- Biologically Equivalent Dose [BED]10 = 41.6 Gy (41.6-60); Equivalent Dose in 2 Gy per fraction [EQD2] Max = 50.00 Gy). 1. Time to local progression. The median TTLP for the overall sample was not reached and the actuarial 1-, 2-, and 3-years local progression rate was 86.36% (Figure 2). Only 2 patients (10%) had both imaging and clinical evidence of local progression 6 months after treatment and 1 patient (5%) 9 months after the treatment. 2. Overall survival The median OS for the entire cohort was 38 months with actuarial survival rates at 1, 2, and 3 years of 100%, 89.95%, and 59.31%, respectively (Figure 3). 3. Toxicity and pain control None of the patients experienced neither radiation adverse events (grade 1-4) nor reported pain flair reaction. None of the patients included in our series experienced VCF. In 17 of 20 patients, a complete pain remission (CR) was observed and 3 of 20 patients had a partial pain remission (PR; CR + PR: 100%).

Time to local progression (TTLP) for the overall sample.

Overall survival (OS) for the entire sample.
Discussion
Stereotactic body radiation therapy is often used in the treatment of vertebral metastases for the characteristic sharp dose decline outside the target volume. In spine-SBRT, the definition of the clinical volume tumor including the GTV often involves the entire vertebral volume. The goal is the maximum tumor control while preserving neurological functions. This concept has led to research for an SIB that shapes the dose to the local control of the tumor with significant dose reductions at the spinal cord (Table 3). 20,28,29
Current Literature on Stereotactic Body Radiotherapy With Simultaneous Integrated Boost in Patients With Spine Metastases.

Abbreviations: NA, not available; OS, overall survival; PTV, planning target volume; PFS: Progression Free Survival.
Several studies suggested that SBRT provides 70% to 100% rate of 1-year local control across clinical scenarios. 17,30 -32 When performed as the primary treatment modality, SBRT is associated with long-term local control rate of 80% to 95% for patients with spinal metastases. 17,33 -35 Analogously, in the adjuvant setting following surgery, SBRT provides local control rates ranging from 70% to 100%. 32,36 We observed that SBRT-SIB provides 1-, 2-, and 3-year TTLP actuarial rates of 86.36%, in line with previous SBRT reports. Figure 4 reports an SBRT-SIB treatment plan and the radiological results 6 months after the treatment.

Stereotactic body radiation therapy–simultaneous integrated boost treatment plan (A) and radiological results 6 months after the treatment (B).
With a radiation dose of 16 to 20 Gy in a single fraction, the tumor volume decreases of the 70% with a tumor regression of the 65% at 2 months. On the other hand, it has been reported that high-dose SBRT may increase the risk of VCF (3% to 39%) and myelopathy (1% to 5%). 7 -11,20 Our hypothesis holds that a SIB to the bone metastasis might overcome this problem. Despite our findings should be interpreted with caution, no VCF and myelopathy were reported in our series.
In this regard, Mantel et al have recently identified frequency, clinical relevance, and risk factors for VCF after spine SBRT with long-term follow-up in 56 patients (61 lesions) within a prospective multicenter phase 2 study (NCT01594892). 37 Post-SBRT VCF developed in 21 lesions (34.4%): of these, 10 lesions (16.4%) showed a progressive VCF, while a new VCF occurred in 11 lesions (18.0%). If on the one hand, SBRT dose did not significantly correlate to VCF in the univariate analysis, receiver operating characteristics analysis revealed that a relative involvement of ≥34.5% of the vertebral body best predicted a post-SBRT VCF with an area under the curve of 0.864, a sensitivity of 77.8%, and a specificity of 89.7%. In addition, in the same study, 37 a BED10 greater than 59.5 Gy has been delivered to the high dose PTV; in our patients, a median BED10 dose of 41.6 Gy has been reached. This could further justify the absence of VCF in our series.
In addition to long-term local control, one of the main purposes of spine SBRT is the pain control. Available data suggest that the 1-year actuarial pain control rate is 84% with doses higher than 14 Gy delivered in a single fraction. 30,38 The use of various SBRT doses in the range of 16 to 24 Gy has obtained higher pain control compared with 14 Gy in a single fraction (90%). 14,39,40 It is worth to note that we obtained an overall pain control in 100% cases, however, due to the small sample size, this data should be regarded with caution and the results may also depend on the use of a high dose of dexamethasone. Finally, in our study, we report a marginal failure rate of 5% after spinal SBRT-SIB, which is in line with previous studies. 15,41
Conclusions
This study suggests that SBRT-SIB provides an excellent TTLP in patients with vertebral metastases as well as a low in-field recurrent disease rate. In the present series, no VCF and myelopathy were reported. However, considering the relatively small sample size, further studies should be promoted to demonstrate the advantage of 8 to 10 Gy to isodose line of 50% in a single fraction in SBRT-SIB modality in patients with vertebral lesions.
Footnotes
Authors’ Note
The study was approved by the local institutional review board: Comitato Etico Interaziendale della Provincia di Messina. Protocol Number: 61/19. Isidora Ielo is also affiliated with Medical Physics Unit, A.O.U. “G. Martino”, Messina, Italy.
Acknowledgments
Authors would like to thank ab medica S.p.A for supporting the Article Processing Charge.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by ab medica S.p.A.