
Abstract
Introduction:
Stereotactic body radiation therapy allows for the precise delivery of high-dose radiation to disease sites and is becoming increasingly used to treat nonspine bone metastases. Previous studies have shown that remineralization of lytic bone metastases follows after conventional radiotherapy. The objective of this study was to investigate changes in bone density in nonspine bone metastases following stereotactic body radiation therapy.
Methods:
A retrospective review was conducted for all patients treated with stereotactic body radiation therapy to nonspine bone metastases between May 2011 and April 2014. A minimum of 1 pretreatment and 1 posttreatment computed tomography scan was required. An independent musculoskeletal radiologist contoured the lesions on the most representative computed tomography slices. Density was measured in Hounsfield units and analyzed using pretreatment and posttreatment ratios.
Results:
Forty sites were treated (55% lytic, 30% sclerotic, and 15% mixed). The median follow-up duration was 7 months. Lytic osseous metastases from renal cell carcinoma progressed during initial follow-up imaging and then returned to baseline. Of 9 lytic lesions not from renal cell carcinoma, 6 showed an immediate increase in density and 2 remained stable. Six of 7 sclerotic lesions from prostate cancer showed decreased density throughout all follow-ups.
Conclusion:
Stereotactic body radiation therapy is efficacious in the remineralization of lytic and demineralization of sclerotic nonspine bone metastases.
Keywords
Introduction
A combination of treatment modalities, including analgesia, bone modifying agents, and external beam radiation therapy (EBRT), have been used as treatment options for nonspine bony metastatic disease. Stereotactic body radiation therapy (SBRT) allows for the precise delivery of high-dose radiation to disease sites while sparing normal tissue. 1 Stereotactic body radiation therapy is becoming an increasingly prevalent component in the management of nonspine bone metastases. Stereotactic body radiation therapy is indicated for patients with either oligometastatic disease, defined by 5 or fewer metastases, or oligoprogressive disease, defined by more than 5 metastases but only a few with significant progression. Additionally, SBRT is a treatment option for those who have tumors historically considered to be radioresistant and those who have been previously irradiated with EBRT. 1 –5
In the setting of EBRT, response to treatment for osseous metastases is typically measured by pain relief and improved quality of life. However, patients for whom SBRT is indicated may not be symptomatic, and so these EBRT end points may be less relevant in this context. Goals of treatment of SBRT are therefore focused on local disease control in addition to symptom relief if present. The Response Evaluation Criteria in Solid Tumors, the MD Anderson criteria, and the Positron Emission Tomography Response Criteria in Solid Tumors have been used in the end point assessments. 6
Another consideration in the determination of osseous tumor response is change in density following treatment. This avenue has been explored previously for osseous metastases following conventional radiotherapy. 7,8 In these trials, both X-ray and computed tomography (CT) scans have been used as imaging modalities. The latter is considered highly sensitive and has the ability to evaluate bone structure, including density. 9 Sclerosis of originally lytic lesions suggests response to treatment, while further lysis suggests progressive disease. Similarly, lysis of originally osteoblastic lesions is considered a response to treatment, while additional sclerosis suggests progression. The objective of this study was to investigate changes in density for both lytic and sclerotic nonspine bone metastases following SBRT.
Methods
A retrospective review was conducted for all 31 patients who were treated with SBRT to nonspine bone metastases at the Sunnybrook Odette Cancer Centre between May 2011 and April 2014. Patients were required to have a CT scan prior to the start of SBRT and at least 1 subsequent CT scan following treatment completion. Computed tomography scans were used as the imaging modality as they were routinely ordered by treating medical oncologists.
An independent musculoskeletal radiologist who was blinded to the condition of the patient, the dose of SBRT, and the clinical outcome reviewed the imaging. The radiated lesions were contoured on the most representative CT slice in the baseline imaging. The same region was also contoured and used for comparison for all subsequent imaging. Density was measured in Hounsfield units and analyzed using pretreatment and posttreatment ratios.
Due to inconsistent follow-up imaging intervals, density was grouped into months 1 to 3, 4 to 6, 7 to 9, and 10 to 12 for each patient, and the median density within these time periods was recorded. This median density value was also used to calculate the average posttreatment/pretreatment density ratio. The posttreatment/pretreatment density ratios were then analyzed based on type of lesion and primary cancer site.
Results
A total of 40 sites in 31 patients were treated. The most common primary cancer sites were renal cell, lung, and prostate. There were slightly more males (54.8%), and the median age at the time of SBRT was 64 years (range, 50-85 years). The SBRT prescribed doses ranged from 20 Gy in 1 fraction (20/1) to 50 Gy in 5 fractions (50/5). The most common dose fractionations were 35 Gy/5, 30 Gy/5, and 24 Gy/2. Ribs and pelvis were the most common irradiated bone metastases. Bone metastases were determined by the radiologist to be mainly lytic (55%), mainly sclerotic (30%), or mixed (15%). The median follow-up duration was 7 months. Patient and treatment characteristics can be found in Table 1.
Patient and Treatment Characteristics.

Abbreviation: SD, standard deviation.
Lytic Lesions
Of 22 (55%) lytic sites, 19 lesions maintained or increased in density throughout the 1-year follow-up. The change in median CT density for all lytic lesions was 1.04 at months 1 to 3, 1.34 at months 4 to 6, 1.35 at months 7 to 9, and 0.97 at months 10 to 12 (Table 2).
Hounsfield Density for All Lytic Lesions.

Abbreviation: L, left; R, right.
Lytic osseous metastases originating from renal cell carcinoma (RCC) appeared to progress during initial follow-up imaging and then returned to baseline closer to month 12 (Figure 1). When analyzed separately from all other lytic metastases, RCC metastases had a median CT density change of 0.8, 0.82, 1.1, and 0.97 at months 1 to 3, 4 to 6, 7 to 9, and 10 to 12 after treatment, respectively.
Posttreatment/pretreatment ratio for all lytic lesions from renal cell carcinoma.
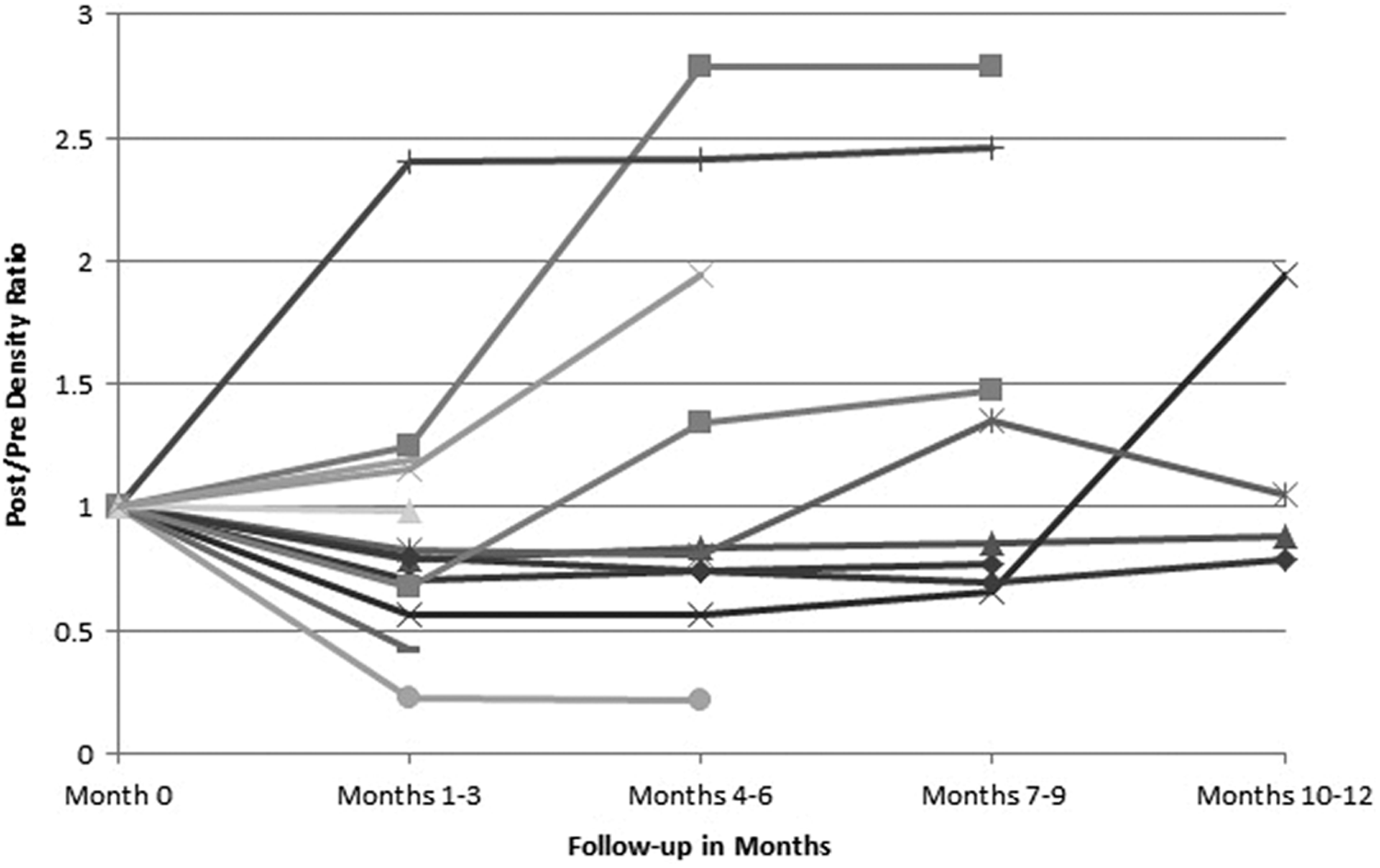
There were 9 lytic lesions from primary carcinomas other than RCC, including those from the lung, breast, and colon. Six of these lesions showed an immediate response by an increase in density, 2 remained stable with no noticeable impact on density, and 1 progressed by becoming increasingly lytic. In the 9 lytic lesions originating from non-RCC primaries, the change in median CT density following treatment was 1.94 and 1.86 between months 1 to 3 and 4 to 6, respectively. Figure 2 illustrates the change in density for all lytic lesions from non-RCC throughout all available follow-ups.

Posttreatment/pretreatment ratio for all lytic lesions from primary carcinomas other than renal cell carcinoma.
Sclerotic Lesions
Twelve (30%) sites irradiated were described as sclerotic. Overall, the sclerotic lesions consistently showed decreased density post-SBRT treatment when compared to baseline (Table 3). The median CT density change was 1.08, 0.94, 0.86, and 0.73 for months 1 to 3, 4 to 6, 7 to 9, and 10 to 12, respectively.
Hounsfield Density for All Sclerotic Lesions.

Abbreviation: L, left; R, right.
Five sclerotic metastases arose from primary carcinomas other than prostate, for which a mixed response was seen. When analyzed again including only prostate cancer metastases, the decrease in density was more substantial. Of the 7 prostate cancer metastases, none had CT follow-up from months 1 to 3. The change in median CT density for lesions imaged between months 4 to 6, 7 to 9, and 10 to 12 was 0.74, 0.86, and 0.58, respectively (Figure 3).

Posttreatment/pretreatment ratio for all sclerotic lesions from prostate carcinoma.
Dose Response
A variety of doses and fractionation regimens were utilized, most commonly 35 Gy/5 (47.5%) and 30 Gy/5 (22.5%). There did not seem to be a significant dose–response relationship.
Discussion
Similar studies of CT density following radiation have been conducted previously in the setting of EBRT. The results of a randomized control trial investigating pain relief and bone remineralization were published in 1999 by Koswig and Budach. 7 One hundred seven patients were included in the study and were randomized to receive either 8 Gy/1 or 30 Gy/10. Although there was no difference in pain relief between the 2 groups, the percentage of density change was 173% in the multiple fraction group and 120% in the single fraction group at 6 months after treatment. 7
The effect of EBRT on the remineralization of osteolytic bone metastases from primary breast carcinoma has also been reported. 8 Of the 25 treated lesions, the percentage of density change was 128%, 141%, and 145% 3 months following a single 8 Gy, 20 Gy/5 fractions, and 30 Gy/10 fractions, respectively. Again, an increase in density following radiation was observed with a larger dose of radiation resulting in a greater amount of remineralization. 8
Our study is the first to investigate remineralization for nonspine bone metastases in the context of SBRT. The results reported herein similarly demonstrate bone remineralization in lytic osseous metastases following radiation treatment. In lytic lesions originating from non-RCC primaries, the median CT density following treatment was 194% and 186% for imaged lesions between months 1 to 3 and 4 to 6, respectively. Our observed density change was greater than that reported in the 2 previous studies, 7,8 likely due to the greater doses of radiation delivered in SBRT compared to EBRT. A dose–response relationship was not observed in our study because most patients were treated with very similar SBRT doses.
Lytic lesions originating from RCC were unique from those of other histologies, as they appeared to show initial progression within the first 3 months and stabilization and/or remineralization after month 4. These data may provide insight into previously reported high rates of fracture in renal cell lytic spinal metastases that occurred early after the SBRT with the median time of 2 to 3 months. The initial lack or even reduction in remineralization may render the bone still weak or even weaker and hence the early fractures. 10
In the setting of EBRT, RCC has been considered to be radioresistant and pain response has remained poor. 3 However, studies that have been conducted with new technology suggest that the high radiation doses delivered in few fractions as in SBRT have the ability to overcome radioresistance. 2,11 –14 The biological pathways resulting in this observation are not entirely understood, but it is believed that the cancer cells undergo a different death mechanism in response to SBRT than with conventional radiotherapy. 15 Our results are consistent with other studies that have reported superior local control in metastatic RCC.
An avenue that has been less explored is the demineralization of sclerotic metastases. In our study, sclerotic metastases from nonprostate histologies had a mixed response to treatment, while the majority of those from prostate cancer showed a decrease in bone density. To our knowledge, the only other study that examined changes in sclerotic osseous metastases was that by German investigators Wachenfeld et al. 16 Their study included 14 patients with vertebral metastases from primary breast carcinoma that were treated with EBRT with a total dose from 30 to 36 Gy. Similar to our study, the authors observed a decrease in bone density of osteoblastic lesions. 16
Our study is limited by a small sample size and its retrospective nature, which did not allow CT scans of treated lesions to be completed at predetermined, consistent intervals. Additionally, only 1 musculoskeletal radiologist reviewed the imaging as opposed to 2 independent radiologists who could have verified the findings. Finally, these patients were undergoing other treatments such as chemotherapy and bisphosphonates, which may confound our results.
Overall, the results presented here show that SBRT is efficacious in the remineralization of lytic and demineralization of sclerotic nonspine bone metastases. Furthermore, our results suggest that SBRT may be more effective than EBRT in achieving this end point, at least in patients with oligometastatic disease. Future prospective investigations are warranted, in which the sample size is larger and imaging is ordered at set intervals for all patients. Confounding treatments should be taken into consideration in these studies. Eventually, a randomized control trial should be conducted in order to determine whether there is a dose–response relationship between dose of SBRT delivered and change in bone density as a secondary end point.
Footnotes
Acknowledgments
The authors thank the generous support of the Bratty Family Fund, Michael and Karyn Goldstein Cancer Research Fund, Joey and Mary Furfari Cancer Research Fund, Pulenzas Cancer Research Fund, Joseph and Silvana Melara Cancer Research Fund, and Ofelia Cancer Research Fund.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.