
Abstract
In this study, the volume response and treatment outcome after hippocampus-sparing whole-brain radiotherapy (HS-WBRT) with simultaneous integrated boost (SIB) using tomotherapy were evaluated. Patients with primary lung adenocarcinoma and multiple brain metastases who had a Karnofsky performance status ≥70 and exhibited well-controlled extracranial disease were treated. The prescribed dose was administered in 10 to 14 fractions as 25 to 28 Gy to whole-brain parenchyma, as 40 to 48 Gy to the gross metastatic lesion, and as 30 to 42 Gy to a 5-mm margin to the metastatic lesion. Double-dose gadolinium contrast-enhanced magnetic resonance imaging at 1-mm slice thickness was performed before treatment and at 1, 4, and 7 months post-treatment. The tumor volume reduction ratio was calculated for each follow-up. Between July 2011 and September 2012, 11 patients with 70 lesions were included in this analysis. The median number of lesions per patient was 4 (range, 2-15). The median initial tumor volume was 0.235 cm3 (range, 0.020-10.140 cm3). The treatment plans were evaluated regarding conformation number (CN), target coverage (TC), and homogeneity index (HI). The median follow-up duration was 14 months (range, 3-25 months) and the 1-year intracranial control rate was 67%. The tumor volume reduction was most prominent during the first month with a median reduction rate of 0.717 (range, −0.190 to 1.000). Complete remission was seen in 22 (33%) lesions, and 45 (64%) lesions showed more than 65% reduction in tumor volume. The CN, TC, and HI values were comparable to that of previous studies, and the mean hippocampal dose was 13.65 Gy. No treatment breaks or ≥G3 acute toxicities were observed during or after treatment. The HS-WBRT with SIB in patients with multiple brain metastases was effective and feasible for volume reduction and showed excellent intracranial control.
Introduction
Brain metastasis is the most common type of intracranial tumor and whole-brain radiotherapy (WBRT) has been established as one of the standard treatment modalities. 1 -3 As new systemic treatment options become available, which increase the survival of patients with advanced disease, the incidence of brain metastases is likely to increase, and the necessity for intracranial control is increasing. Patients with good performance status, well-controlled extracranial disease, and a limited number of lesions could benefit, in terms of intracranial tumor control, from more aggressive treatment such as stereotactic radiosurgery (SRS) or neurosurgical resection combined with WBRT. 4 -7
However, WBRT has been linked to memory function decline, and SRS or surgical resection without WBRT became another treatment option in patients with oligo-brain metastasis. 5,8 The main cause of memory function decline is hippocampal damage, and efforts to reduce the hippocampal dose during WBRT have been made. 9,10 The Radiation Therapy Oncology Group (RTOG) 0933 phase II clinical trial reported the outcome of patients with brain metastasis who were treated with hippocampus-sparing WBRT (HS-WBRT). Hippocampal sparing was associated with better memory preservation at 4-month follow-up compared with historical controls. 11
Although HS-WBRT may be followed by a sequential SRS boost delivered to the gross tumor, the whole brain and gross tumor may be treated simultaneously (simultaneous integrated boost [SIB]) by intensity-modulated radiation therapy. The HS-WBRT with SIB may be performed using helical tomotherapy or volumetric modulated arc therapy. 12 -14 Compared with HS-WBRT plus sequential SRS boost, HS-WBRT with SIB has several advantages. First, SIB to multiple brain metastases does not require separate stereotactic procedures and can reduce the treatment period. Second, tumors >3 cm or those with significant mass effect are not good candidates for SRS, 15 and fractionated delivery can be more effective in reducing normal tissue complication. Finally, multiple targets can be easily treated at different dose levels in the course of treatment allowing a lower exposure to the hippocampus compared to when using WBRT plus SRS. 16 Dosimetric studies reported that HS-WBRT with SIB results in high-quality dose distribution to multiple brain metastases and the whole brain. 12,16,17
Tumor shrinkage after WBRT has been reported to correlate with better survival and neurocognitive function preservation. 18 Previously, we reported the early volumetric change, treatment outcome, and feasibility of low-dose WBRT plus local boost using 3-dimensional conformal radiotherapy (RT) for brain metastases. 19 However, the patients did not receive HS-WBRT, and boost RT was delivered after WBRT. The HS-WBRT with SIB using helical tomotherapy was adopted in our institution since 2011 and primary diagnosis of the majority of patients was adenocarcinoma of lung. The whole-brain dose was reduced below 30 Gy, and the gross tumor dose was elevated above 30 Gy. We retrospectively reviewed the volume response and treatment outcome in patients treated with HS-WBRT with SIB using helical tomotherapy for multiple brain metastases. The dose distribution characteristics were also calculated to evaluate feasibility. Since the tumor response to RT is varied in different histologic types, we have analyzed only the patients diagnosed with primary lung adenocarcinoma.
Materials and Methods
Patient Characteristics
Between July 2011 and September 2012, 70 metastatic lesions arising from 11 patients with histologically proven lung adenocarcinoma were treated with HS-WBRT plus SIB using helical tomotherapy. All patients underwent position verification and correction using megavoltage computed tomography (CT) prior to each treatment session. Inclusion criteria included patients with controlled extracranial disease who had Karnofsky performance status (KPS) ≥70 without leptomeningeal seeding. All patients underwent double-dose gadolinium contrast-enhanced magnetic resonance imaging (MRI) at 1-mm thickness slice intervals before RT and at follow-up. This study was approved by the institutional review board.
The patients’ characteristics are summarized in Table 1. Seven patients had synchronous brain metastasis at the initial diagnosis, and 4 patients had metachronous brain metastasis. One patient underwent metastasectomy of the largest cystic lesion because of left-side motor weakness. Three patients with localized disease at the initial diagnosis underwent resection of the primary tumor and experienced brain metastasis without locoregional recurrence during follow-up. At the time of brain RT, 4 patients had brain metastasis only, 3 patients had additional single-bone metastasis, 1 patient had contralateral lung metastasis, and 3 patients had combined bone and nonregional lymph node metastasis. One patient with a progressive extracranial lesion at the time of brain RT did not meet the inclusion criteria. However, the patient was young (44 years), had a good performance status (KPS 90), and previously showed a good response to chemotherapy and targeted agents; therefore, HS-WBRT with SIB was administered at the physician’s discretion. Six patients were receiving gefitinib during HS-WBRT and continued gefitinib treatment after HS-WBRT. In all, 5 patients did not receive systemic treatment during HS-WBRT, but 3 received systemic chemotherapy and 1 received erlotinib after HS-WBRT.
Patient Characteristics.
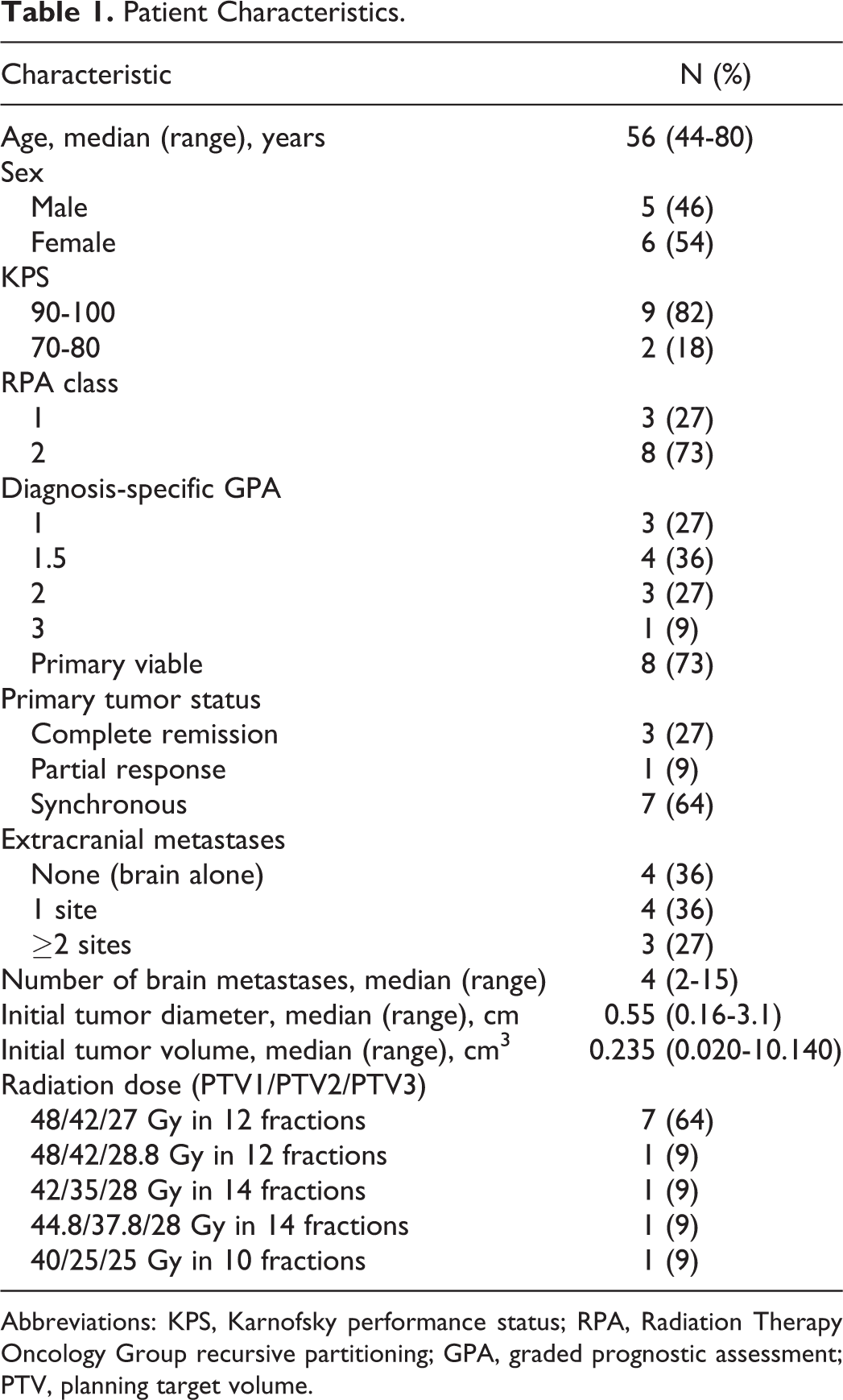
Abbreviations: KPS, Karnofsky performance status; RPA, Radiation Therapy Oncology Group recursive partitioning; GPA, graded prognostic assessment; PTV, planning target volume.
Treatment Planning and Evaluation
Treatment planning was based on planning CT scans without intravenous contrast agent with 1-mm slice thickness intervals. Contrast-enhanced T1-sequences were fused to the planning CT for gross tumor and hippocampal contouring. Planning target volume (PTV) 1 was defined as all visible lesions on an MRI scan. The PTV2 was defined as the addition of a 3- to 5-mm margin on PTV1. The 3- to 5-mm margin was intended to cover the areas with a higher risk of microscopic tumor spread compared with normal brain tissue. PTV3 was defined as the whole-brain parenchyma with a 3-mm margin, excluding the hippocampus with 1-mm margin. Current recommendations consider a 5-mm volumetric expansion from the hippocampus to create a hippocampal avoidance zone 20 ; however, because the lack of prospective data on the incidence of perihippocampal recurrence after hippocampus sparing, we applied a 1-mm margin in concern of recurrence in the perihippocampal area. Both hippocampi were delineated based on MRI scans according to the RTOG guideline. 20 None of the patients had a metastatic lesion either in the hippocampus per se or in the hippocampal avoidance region defined as a 5-mm geometric expansion from the hippocampus by RTOG. 20
Treatment plans were optimized using the tomotherapy planning software (TomoTherapy Inc, Madison, Wisconsin, version 3.1.x). A field width of 2.5 cm and a pitch of 0.287 were used in most patients. For 1 patient who had 15 metastatic lesions, a field width of 1.0 cm and a pitch of 0.43 were used to achieve better conformity. The median for modulation factor was 1.30 (range, 1.09-1.69). The prescribed dose to PTV1, PTV2, and PTV3 was 48, 42, and 27 Gy in 12 fractions. The prescription dose of PTV3 was reduced compared to the standard WBRT dose to spare the healthy brain tissue. All patients were evaluated with a double-dose gadolinium contrast-enhanced brain MRI at 1-mm thickness, so the sensitivity of detecting very small brain metastases was high, but because brain tissue appearing normal could harbor microscopic tumors, a prophylactic dose was applied to the radiologically normal brain tissue. PTVs were prescribed at 95%. The minimally accepted dose was 80%, and the maximum dose limit was 110% of the prescribed dose. The hippocampal dose was restricted to a mean dose below 15 Gy. The treatment plans were evaluated regarding conformation number (CN), target coverage (TC), and homogeneity index (HI). The CN is defined as (VT,pres/VT) × (VT,pres/Vpres). VT,pres is the volume within the target receiving a dose equal to or greater than the prescription dose, VT is the target volume, and Vpres is the volume receiving a dose equal or greater than the prescription dose. The CN value can range between 0 and 1, with CN = 1 characterizing perfect conformation of the prescription isodose to the target volume. The TC is defined as VT,pres/VT. It can range from 0 to 1, with TC = 1 representing perfect coverage. The HI is defined as (D2% − D98%)/Dmedian. D2% is the greatest dose delivered to 2% of the target volume, D98% is the dose delivered to 98% of the target volume, and Dmedian is the median dose of the target volume. Smaller HI values indicate more homogeneous dose distributions, with HI = 0 for perfect target dose homogeneity.
The biologically equivalent dose in 2-Gy fractions (EQD2) using the linear quadratic model was used to compare different dose schedules. For calculating the dose delivered to tumor and normal organs, α/β ratio of 10 and 3 Gy was used, respectively.
Follow-up
Patients underwent follow-up with brain MRI and a neurological examination at 1, 4, and 7 months post-RT. Toxicity was graded according to the Common Terminology Criteria for Adverse Events (CTCAE) Version 4.0. All follow-up MRI scans were performed with the same protocol as the pre-RT MRI. All MRI scans were fused using MIM 6.0 (MIM Software, Inc, Cleveland, Ohio; Figure 1), and the volume and diameter of each lesion were obtained. Only the contrast enhancing lesion was delineated and 2 physicians have delineated in consensus to increase reliability in volume measurement. The volume reduction ratio (VRR), VRR = (VpreRT − VpostRT)/VpreRT, was calculated using the volume data for each lesion. We used last observation carried forward for patients that discontinued follow-up.

Volumetry of serial brain magnetic resonance imaging using the MIM software.
Treatment response in each individual lesion was evaluated according to the response evaluation criteria in solid tumors (version 1.1). 21 Objective response was defined as a complete response (CR) or partial response (PR). Local progression was defined as increase of the previously defined lesion included in the PTV2. Remote intracranial progression was defined as any new lesion developing outside the PTV2. Overall survival was defined from the start of RT to any cause of death.
Statistical Analysis
Survival and time to progression were estimated using the Kaplan-Meier method. The correlation of the initial tumor size to response was evaluated using logistic regression. Correlations between 2 variables were assessed using the Pearson correlation coefficient, r. A P value of <.05 was considered as statistically significant. Statistical analyses were performed with IBM SPSS version 20.0 (SPSS, Chicago, Illinois).
Results
Treatment Outcome
The median follow-up period from the diagnosis of brain metastasis to the last brain MRI scan was 10 months (range, 2-14 months). The median follow-up period for all patients was 14 months (range, 3-25 months). The 1-year intracranial control rate was 67% (95% confidence interval [CI], 47%-100%), and the 1-year overall survival rate was 72% (95% CI, 44%-99%; Figure 2). One patient who experienced intracranial recurrence achieved a CR for all 15 lesions but developed leptomeningeal seeding without local progression after 1 year. Four patients died because of extracranial disease progression. One patient who had progressive extracranial disease at the time of brain RT died 3 months after the diagnosis of brain metastasis. The other 6 patients survived >10 months after treatment.

Overall survival and intracranial control of the patients.
Early Tumor Response
The volume change in the 70 brain lesions is shown in Figure 3. Volume reduction was most prominent during the first follow-up after brain RT and minimal during the second and third follow-up. The median VRR value at first, second, and third follow-up was 0.717 (range, −0.190-1.000), 0.806 (range, −0.125-1.000), and 0.806 (range, −0.125-1.000), respectively. All patients were evaluated with their first follow-up MRI, but 2 patients died before second and third follow-up and 3 patients refused the third follow-up MRI. Fifty-four lesions showed volume reduction and a single lesion displayed a 19% increase in volume at the first follow-up. Figure 4 summarizes the response of the metastatic lesions at each follow-up. Objective response was observed in 45 lesions and it was achieved at first follow-up for 39 lesions. No patients exhibited radiologic progression until third follow-up. The radiologic tumor response at the last follow-up was CR in 22 lesions, PR in 23, and stable disease in 25. The overall CR rate was 31%, and the objective response rate was 64%. Five patients had an objective response for all brain lesions and 6 patients had a mixed response. Pre-RT volume was not significantly associated with objective response rate (odds ratio [OR] 0.33, 95% CI 0.10-1.13) and CR rate (OR 0.49, 95% CI 0.22-1.08).

Change in tumor volume of each metastatic lesion on preradiotherapy on the first, second, and third follow-up.

Radiologic response of the 70 metastatic lesions on serial follow-up.
Dose Distribution Characteristics
The mean ± standard deviation of CN values for PTV1 and PTV2 were 0.40 ± 0.20 and 0.48 ± 0.16, respectively. The mean ± standard deviation of TC values for PTV1, PTV2, and PTV3 were 0.94 ± 0.12, 0.99 ± 0.02, and 0.89 ± 0.05, respectively. The mean ± standard deviation of HI values for PTV1, PTV2, and PTV3 were 0.08 ± 0.03, 0.17 ± 0.04, and 0.52 ± 0.16, respectively. There was a positive correlation between CN and pre-RT volume for PTV1 (r = .72, P = .043, 2-sided); CN values improved with increasing pre-RT tumor volume. There were no significant correlations between pre-RT tumor volume and other indexes. The number of lesions and dosimetric indexes had no significant correlation.
The bilateral hippocampal dose is as follows: the EQD2 (α/β = 3 Gy) to 2% of the structure volume was 23.02 ± 3.82 Gy, and the EQD2 of the hippocampal mean dose was 13.65 ± 2.23 Gy.
Toxicity
There were no treatment breaks in any patient undergoing RT. There were no grade 3 toxicities, and most of the side effects were mild and included headache and nausea that were manageable with conservative treatment. No brain edema was evident, either clinically or radiologically. Prior to RT, 3 patients developed neurologic symptoms such as left visual field defect, left motor weakness, and dizziness, which did not progress after RT.
Discussion
This retrospective study showed that lung adenocarcinoma brain metastasis with well-controlled extracranial disease resulted in rapid volume reduction and excellent intracranial tumor control in response to HS-WBRT and SIB. Using helical tomotherapy, we were able to achieve good dose conformity and homogeneity including patients with more than 10 metastatic lesions. This report was unique for the following reasons: (1) volume reduction kinetics were analyzed in a homogeneous group of patients; (2) every patient underwent 1-mm thickness double-dose Gd-enhanced MRI, meaning that very small lesions were detectable; and (3) homogeneous RT technique was adapted for treatment delivery in all patients.
The reduction in tumor volume was most prominent during the first month after brain RT and 88% of the objective responders achieved objective response within 1 month. Although rare, further volume reduction was seen 7-month posttreatment. The median VRR at 1 month in our study was higher than the median VRR at 2 months reported from a previous study after WBRT only (0.72 vs 0.45). 18 This higher dose delivered to the gross tumor may have resulted in the higher rate of radiologic tumor response. The EQD2 (α/β = 10 Gy) to PTV1 was a median of 56.0 Gy, which is much higher than the commonly used schedule of 30 Gy in 10 fractions (EQD2 = 32.5 Gy [α/β = 10 Gy]). In addition, while delivering a higher dose to the gross tumor, a lower dose of 27 Gy in 12 fractions (EQD2 = 27.6 Gy [α/β = 3 Gy]) was administered to the grossly normal brain parenchyma to spare normal brain structures, which is lower than the 30 Gy in 10 fractions schedule (EQD2 = 36.0 Gy [α/β = 3 Gy]). Although 1 patient with 15 metastatic lesions experienced leptomeningeal seeding, intracranial control was not compromised in other patients.
A limited number of studies have reported on the dose distribution characteristics for HS-WBRT with SIB. 12,17 They applied a 2- to 5-mm safety margin to the gross tumor to create the PTV, which is similar to PTV2 in the current study. The TC and HI values in our study were comparable to those in previous studies. However, the CN values from other studies (CN = 0.708 ± 0.128 and 0.60 ± 0.13) were better than those for PTV2 observed in our study (CN = 0.48 ± 0.16). This inferior conformity is likely to be caused by the different volume distributions. It has been reported that better dose conformity can be achieved in larger targets. 12,14,17 In concordance, a clear dependence of CN on pre-RT volume was observed in the current study. Some patients included in this study had very small tumor volumes, and lower CN values could be the result of using 1-mm slice thickness brain MRI for target contouring. Alternatively, the large number of treated lesions in the current study could account for the lower CN value. Most of the previous studies evaluated the plan quality in patients with oligometastasis. However, the current study demonstrates how moderate conformity can be achieved in patients with >10 lesions. The higher hippocampal dose, compared with other studies, using HS-WBRT was mainly due to the small hippocampal-avoiding region, which expanded only 1 mm from the hippocampal contour compared with the 5 mm reported previously. 17,20 The minimal margin of 1 mm used in our study came from the concern of increased perihippocampal recurrence with a wider margin. However, a recent prospective study showed that only 4.5% of patients who developed intracranial progression after HS-WBRT experienced progression in the hippocampal avoidance area using a 5-mm margin to the hippocampus, which seems feasible. 11 Despite accepting a minimum whole-brain dose of 80%, the very narrow avoidance zone of 1-mm margin made it difficult to achieve a dose gradient. Although none of the patients had memory function decline that interfered with daily activities, we could not determine whether the higher hippocampal dose influenced memory function in this study because of a lack of quantitative neurocognitive function data. Recently published data from RTOG 0933, a phase II multi-institutional trial, describe the benefit of hippocampus sparing during standard WBRT of 30 Gy in 10 fractions. 11 The maximal hippocampal dose did not exceed 16 Gy and the dose to 100% of the hippocampus did not exceed 9 Gy. Memory decline was significantly lower in that study compared with historical controls. Another retrospective study reported that an EQD2 to 40% of the bilateral hippocampi >7.3 Gy was associated with long-term impairment of delayed recall, 12 but the actual threshold dose for the hippocampus is yet to be investigated.
Currently, the diagnosis-specific graded prognostic assessment (GPA) is used to predict the prognosis of patients with brain metastasis from different primary tumors. For nonsmall cell lung cancer, the main 4 prognostic factors are age, performance status, extracranial metastases, and the number of brain metastases. 22 In our cohort, patients were anticipated to have a dismal prognosis with a relatively low diagnosis-specific GPA score because most of the patients had extracranial metastases with >3 metastatic brain lesions. The median survival reported for patients with nonsmall cell lung cancer with a GPA score of 1.5 to 2, which includes most of the patients in our study, is 5.5 months. Here, excluding the patient who had progressive extracranial disease, 10 patients survived for a median of 14.5 months (range, 10.4-24.9 months). Therefore, patients with well-controlled extracranial metastases should be distinguished from patients with progressive extracranial metastases since they have a better prognosis and may benefit from more aggressive brain treatment. However, careful patient selection should be performed to avoid unnecessary treatment, such as in the case here of the patient with progressive extracranial disease who died 2.7 months after a diagnosis of brain metastasis.
This study has limitations such as its retrospective nature and small number of patients. Only 1 patient experienced intracranial recurrence and we were not able to define the prognostic value of early tumor volume response. In addition, neurocognitive function tests were not routinely performed, and the effect of hippocampal sparing could not be assessed quantitatively. Furthermore, the patients’ quality of life was not assessed using standardized questionnaires. Future studies in a larger population with an assessment of functional outcome and quality of life would address these limitations and further confirm the efficacy of this treatment.
In conclusion, HS-WBRT with SIB can deliver high-dose RT to brain tumors while reducing the dose delivered to the hippocampus with a high-quality dose distribution resulting in rapid tumor reduction and excellent intracranial control. The value of tumor volume reduction at 1 month is to be evaluated in a larger patient cohort.
Footnotes
Abbreviations
Authors’ Note
This study was presented as a poster at the 55th Annual Meeting of the American Society of Radiation Oncology (ASTRO), Atlanta, GA, September 22-25, 2013.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a faculty research grant of Yonsei University College of Medicine (6-2014-0031).