
Abstract
Objective:
To develop decision trees predicting for tumor volume reduction in patients with head and neck (H&N) cancer using pretreatment clinical and pathological parameters.
Methods:
Forty-eight patients treated with definitive concurrent chemoradiotherapy for squamous cell carcinoma of the nasopharynx, oropharynx, oral cavity, or hypopharynx were retrospectively analyzed. These patients were rescanned at a median dose of 37.8 Gy and replanned to account for anatomical changes. The percentages of gross tumor volume (GTV) change from initial to rescan computed tomography (CT; %GTVΔ) were calculated. Two decision trees were generated to correlate %GTVΔ in primary and nodal volumes with 14 characteristics including age, gender, Karnofsky performance status (KPS), site, human papilloma virus (HPV) status, tumor grade, primary tumor growth pattern (endophytic/exophytic), tumor/nodal/group stages, chemotherapy regimen, and primary, nodal, and total GTV volumes in the initial CT scan. The C4.5 Decision Tree induction algorithm was implemented.
Results:
The median %GTVΔ for primary, nodal, and total GTVs was 26.8%, 43.0%, and 31.2%, respectively. Type of chemotherapy, age, primary tumor growth pattern, site, KPS, and HPV status were the most predictive parameters for primary %GTVΔ decision tree, whereas for nodal %GTVΔ, KPS, site, age, primary tumor growth pattern, initial primary GTV, and total GTV volumes were predictive. Both decision trees had an accuracy of 88%.
Conclusions:
There can be significant changes in primary and nodal tumor volumes during the course of H&N chemoradiotherapy. Considering the proposed decision trees, radiation oncologists can select patients predicted to have high %GTVΔ, who would theoretically gain the most benefit from adaptive radiotherapy, in order to better use limited clinical resources.
Introduction
Radiation treatment delivery techniques for head and neck (H&N) cancer have changed dramatically since the emergence of computed tomography (CT) in the 1970s. For the first time, radiation oncologists were able to view 3-dimensional (3D) patient anatomy and use these data to develop 3D-based conformal radiation plans. 1 Another milestone in delivery technique occurred in the 1990s with intensity modulated radiotherapy (IMRT), which dramatically improved dose conformality, maximized tumor coverage, and increased sparing of normal tissues. 2 A more recent advance in treatment planning and delivery has been the use of image guidance to monitor for volume changes in target and organs at risk (OARs) to potentially “adapt” these plans as needed during the course of treatment. This process is called adaptive radiotherapy (ART). 3
Several institutions have reported significant changes in tumor volume and patient anatomy during the course of radiotherapy. Investigators have used a variety of image guidance techniques to assess for volume and anatomical changes, including CT on rails, 4 CT simulators, 5,6 cone-beam CT, 7 MVCT, 8 positron emission tomography, and magnetic resonance imaging. 9,10
Volumetric changes can potentially have a major impact on target and OAR dose coverage. Hence, without assessing for these changes, the patient might receive excessive dose to normal tissue or underdosage to target tissue. Single institution studies monitoring dose delivered to the parotid glands during the course of conventional H&N cancer treatment noted that the delivered dose to the parotids was significantly higher than compared to the pretreatment plan, estimated by recalculating the initial plan on the on-treatment CT scans. 4 This was due to anatomical changes from patient weight loss, tumor shrinkage, parotid gland shrinkage, and parotid gland center of volume medial displacement. Furthermore, Barker et al reported the decrease in gross tumor volume (GTV) at a median rate of 1.7% to 1.8% per day for H&N cancers, while the volume of the parotid glands decreased at a median rate of 0.6% per day. 11 Furthermore, tumor volume reduction has been clinically correlated with prognosis. In a recent study of 59 patients with oropharyngeal cancer treated with definitive RT and underwent adaptive replanning, patients who had pretreatment to mid-treatment tumor volume reduction rate greater than 35% had higher 3-year locoregional control rate, 94.4% versus 72.4%. 12
Even with all the benefits of ART, the utilization of ART for H&N cancer has been slow due to the additional personnel and resources needed to perform repeat imaging, recontouring, replanning, and analyzing previous and new treatment plans. Furthermore, repeat imaging and planning can increase the overall cost of patient care. Numerous studies have reported that the percentage of patients that would benefit from ART ranges from 21% to 66%. 6,13 Thus, a more prudent approach would be to identify the select patients with H&N cancer who are predicted to have significant tumor volume reduction prior to starting treatment. These patients would theoretically gain the most benefit from ART. The purpose of our study is to develop decision tree algorithms to predict for primary and nodal tumor volume reduction based on pretreatment clinical, pathological, and dosimetric factors.
Materials and Methods
Forty-eight patients with advanced H&N cancer who underwent definitive radiation therapy with concurrent chemotherapy at our institution from 2009 to 2014 were retrospectively analyzed per institutional review board. All patients had biopsy proven diagnosis of primary squamous cell carcinoma of the nasopharynx, oropharynx, oral cavity, or hypopharynx. All of the patients received 1 of the 3 chemotherapy regimens: cisplatin 100 mg/m2 (days 1, 22, and 44), weekly cisplatin (average dose 50 mg/m2), or weekly cetuximab (average dose 200 mg/m2). All chemotherapy was delivered intravenously.
The patients had pretreatment CT simulation using our departmental scanner (Big Bore; Phillips Medical Systems, Andover, Massachusetts). All patients were immobilized using a custom-fitted thermoplastic face mask and shoulder pulls. The CT scan was performed with 3 mm thick slices, and data were transferred to XIO (Elekta, Maryland Heights, Missouri) planning software (2009-July 2012) or Eclipse (Varian Medical Systems, Palo Alto, California; August 2012-present). All patients were treated with either static field IMRT or RapidArc. The initial treatment plans include 2 separate volumes: initial volume (gross tumor, CTV, and setup margin) and boost volume (GTV and setup margin) that were treated consecutively. The median initial, boost, and total doses were 48.6, 21.6, and 70.2 Gy, respectively.
During the course of radiation therapy, all of these patients had a repeat CT scan (rescan) due to changes in palpable (or visible) tumor size and/or patient weight loss (>15% from baseline). The decision to repeat the scan was determined at the treating physician’s discretion; therefore, only the patients who required a rescan were included in this study. The initial CT scan and plan were fused onto the rescan CT using bony and soft tissue anatomy. We analyzed the dose distributions and coverage of the original plan on the repeat CT scan for dosimetric evaluation. All of the patients were replanned for the boost portion of their treatment (21.6 Gy) using rescan CT.
The gross primary (GTVp) and gross nodal (GTVn) tumor volumes along with OAR were contoured on both the initial and rescan CT scans. The percentages of GTV volume change (%GTVΔ) for primary, nodal, and total GTV were calculated. Two separate decision tree analyses were performed. The patients were divided into high and low (H/L) tumor volume reduction groups based on the median total %GTVΔ for both the primary and nodal volumes (Figure 1). The H/L tumor volume change was the classifying attribute for each decision tree. The 14 predictive attributes (note 1) for the decision tree analysis included age, gender, Karnofsky performance status (KPS), primary site of tumor, human papilloma virus (HPV) status (estimated by p16 status), tumor grade, primary tumor growth pattern (endophytic vs exophytic), tumor stage, nodal stage, group stage, chemotherapy, and GTVp, GTVn, and total GTV volumes on initial planning CT (Table 1).

Tumor volume change from the initial CT scan (left) to rescan CT (right) demonstrating low and high tumor shrinkage in 2 representative patients (initial GTVp: red, rescan GTVp: green, initial GTVn: purple, and rescan GTVn: cyan). CT indicates computed tomography; GTVn, nodal gross tumor volume; GTVp, primary gross tumor volume.
Patient and Tumor Characteristics (48 Patients).

Abbreviation: HPV, human papilloma virus.
In this study, the C4.5 Decision Tree Induction algorithm was used to model primary and nodal tumor volume reduction using Weka 3.6.11 Data Mining Suite. 14 The decision tree induction algorithm that was used in this study was originally proposed by Quinlan. 15 Generating optimal decision trees to classify items according to their attributes has been studied extensively in statistical pattern recognition 16 and in the context of prediction of a target attribute. 17 Decision trees have also been used to help guide decision making for the use of radiotherapy, 18 H&N cancer management 19 and therapy outcome cause analysis. 20,21 Decision tree analysis is used as a well-proven classification technique for quantitative data sets.
Decision tree data analysis techniques in general and C4.5 implementation in particular were chosen for this study for several reasons. We have considered use of several alternative data mining techniques (ie, multivariate regression, segmentation/clustering algorithms, neural networks, and association rule mining methods, among others) but decided to present our findings with the decision tree implementation due to its significant advantages for the kind of data available for this study. The flexibility of the algorithm for handling different data attributes is an important factor in determination of the appropriate data mining technique. Decision tree implementations also lead to graphical depictions of associations between data attributes that are quite intuitive and easy to read. An audience who may not necessarily have an advanced data analysis background can still make sense of the results without a need for extended explanations of the implementation details. The method we implemented (C4.5) has been successfully used over the years for risk identification and mitigation, financial decision making, and strategic management scenarios. In fact it has been the most popular decision tree algorithm and has been used as a benchmark against newer implementations that were proposed later on.
In our implementation, the goal of the decision tree induction algorithm was to develop the optimal classification of instances based on the decision criteria learned from the data. The 14 patient and tumor characteristics were initially all treated to be equally likely to predict volume change. This algorithm recursively identifies those attributes that are most predictive of %GTVΔ while eliminating alternative methods that are not best fit to represent the underlying data. The two proposed decision trees are the ones with the highest predictive accuracies for primary and nodal volume change, respectively. The identification of the most predictive patient attributes was achieved using the gain ratios. The accuracy refers to the predictive ability of a decision tree to classify the data set and it is a type of goodness-of-fit measure. It is defined as the percentage of the accurate predictions made by the decision tree on the given data set.
Results
The median primary GTV on initial and rescan CT was 31.1 and 20.7 cm3, respectively. The median nodal GTV was 22.0 cm3 on initial CT and 12.9 cm3 on rescan CT. The median %GTVΔ between initial and rescan CTs was 26.8% for primary GTV and 43.0% for nodal GTV (P < .0001, Student paired t test; Figure 2). The median total %GTV reduction was 31.2%. Three patients had an increase in total GTV during treatment. The median dose at rescan was 37.8 Gy (range: 14.4-51.5 Gy). Median time between initial and rescan CT was 42 days (range: 23-77 days). There was no correlation between either the median time between scans or median dose at rescan with the percentage GTV changes.
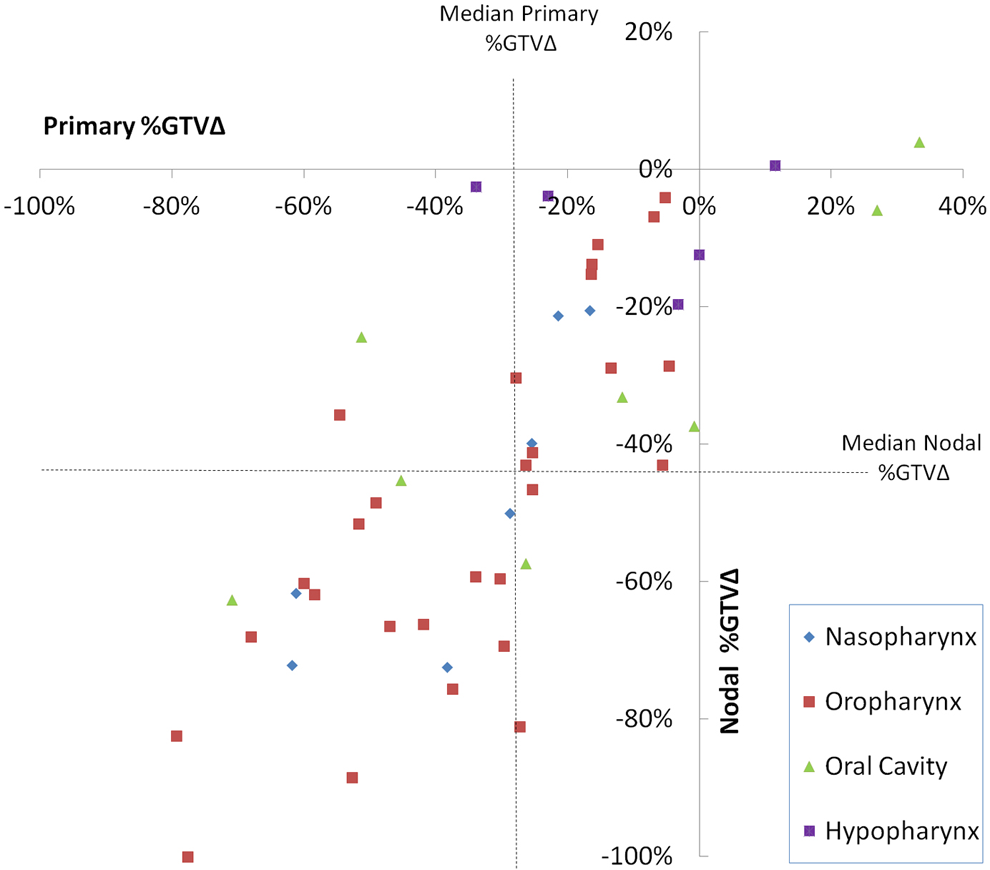
Primary and nodal gross tumor volume change (%GTVΔ) from the initial CT scan to rescan CT for different sites. Dashed lines show the median %GTVΔ. CT indicates computed tomography.
Since the rate of change in primary and nodal GTV volumes was significantly different, two separate decision trees were generated to predict primary and nodal GTV reduction in order to investigate the underlying pretreatment factors. Type of chemotherapy, age, primary tumor appearance, site, KPS, and HPV status were the most predictive for H/L primary GTV reduction and had an accuracy of 88% (Figure 3). The decision tree algorithm used to predict H/L nodal GTV volume change had an accuracy of 88% using the following attributes: KPS, site, age, primary tumor growth pattern, and pretreatment primary and total tumor volumes (Figure 4).

Decision tree predicting the primary tumor volume change (high or low) using patient and tumor characteristics. The numbers in parentheses at the leaves show the number of patients reaching that leaf/the number of patients not placed accurately. For example, the low (5/1) leaf demonstrates that of the 5 total patients, 4 of the 5 had low and 1 of the 5 had high primary tumor volume reduction.

Decision tree predicting the nodal tumor volume change (high or low) using the patient and tumor characteristics. The numbers in parentheses at the leaves show the number of patients reaching that leaf/the number of patients not placed accurately. For example, the high (13/1) leaf demonstrates that of the 13 patients, 12 of the 13 had high, and 1 of the 13 had low primary tumor volume reduction.
Decision Tree for GTVp Reduction
To predict volume reduction of the primary tumor, chemotherapy was the main factor separating the decision tree into 3 initial branches (Figure 3). In the cetuximab group, the primary tumor growth pattern determined the primary tumor volume shrinkage, with endophytic tumors having more volume reduction than exophytic tumors. In the low-dose cisplatin group, all of the patients had low volume reduction. For patients in the standard cisplatin group, the decision tree was further divided based on age. Patients with age ≤47 had higher volume reduction. For patients with age greater than 47, site was the next predicting parameter. Patients with age greater than 47 and sites other than oropharynx had low tumor volume reduction. For patients with primary oropharyngeal cancer, KPS partitioned the decision tree further, with KPS ≤80 having high volume reduction. Patients with KPS greater than 80 were further divided based on HPV status: HPV-positive patients were predicted to have low primary tumor volume reduction, while HPV negative or unknown ones predicted to have high volume shrinkage.
Decision Tree for GTVn Reduction
For predicting volume reduction in gross nodal volume, KPS was the main factor separating the decision tree algorithm into 2 initial branches (Figure 4). Patients with KPS ≤60 predicted to have high nodal volume reduction. For patients with KPS greater than 60, site was the next determining factor, with multiple subattributes further dividing the branches based on site. All of the patients with hypopharyngeal cancer had low nodal volume reduction. With respect to the primary tumor growth pattern in oral cavity patients, the exophytic group had high nodal volume reduction compared to the endophytic group. As for the nasopharynx group, all patients with age ≤51 had high nodal volume shrinkage. In the oropharynx group, the primary GTV partitioned the decision tree further. Patients with GTVp greater than 45.5 cm3 had low volume reduction. For patients with GTVp ≤45.5cm3, the volume reduction was determined by the total gross tumor volume (GTVtot = GTVp + GTVn): patients with GTVtot greater than 31.5 cm3 had high nodal volume reduction compared to the group with GTVtot ≤31.5 cm3.
Discussion
Based on this retrospective analysis, primary and nodal H&N tumor volume changes during chemoradiotherapy can potentially be predicted by pretreatment parameters. The use of a decision tree algorithm can selectively identify patients who are more likely to have significant tumor volume reduction. This group of patients may benefit the most from repeat imaging and replanning during a course of H&N chemoradiotherapy.
The two decision trees developed from our patient group are clinically relevant. In the decision tree algorithm predicting for primary tumor volume reduction, chemotherapy was the main factor separating the tree into 3 branches. All of the patients in the low-dose cisplatin group had low tumor volume reduction. Low-dose cisplatin has been shown to have inferior outcomes when compared to standard-dose cisplatin (100 mg/m2). 22 In the standard-dose cisplatin group, age was an important determining parameter. Several studies have noted that younger patients with H&N cancer squamous cell carcinoma (HNSCC) and minimal to no smoking history are more likely to have HPV-positive tumors compared to older patients. 23 -25 Furthermore, patients with HPV-positive HNSCC generally tend to have better prognosis compared to their HPV-negative counterparts. 26 -28 In this study, patients in the oral cavity and hypopharynx groups had low primary tumor volume reduction, which fits into the general response pattern for these subsites. 29 -31
In the decision algorithm predicting for nodal volume reduction, patients in the oropharyngeal group with smaller primary tumors, but larger total gross tumor volume had high nodal volume shrinkage. Over 70% of the newly diagnosed patients with oropharyngeal cancer are HPV positive. 32 Approximately 57% (16 of 28) of patients in the oropharyngeal group were HPV positive in this study. Several prospective trials have shown that patients with HPV-positive oropharyngeal squamous cell cancers are more likely to have smaller primary tumors, higher nodal burden, and overall, better prognosis than HPV-negative tumors. For instance, in the Trans-Tasman Radiation Oncology Group Phase III Trial 02.02, patients with p16-positive oropharyngeal tumors presented with smaller primary tumors but more advanced nodal disease. The p16-positive patients had significantly better 2-year overall survival and disease-free survival than p16 negative. 26
The 2 decision trees presented here provide several interesting, hypothesis-generating results. In the cetuximab group, the endophytic growing tumors had high primary volume reduction. In the literature, HNSCC with exophytic growth pattern is known to have better response (tumor shrinkage) and prognosis than endophytic tumors. 33,34 However, a recent study analyzed 60 patients with HNSCC treated with radiotherapy and found no difference in disease progression or recurrence-free survival between exophytic and endophytic tumors. 35 Nevertheless, a prospective trial is needed to investigate whether cetuximab is more effective for endophytic rather than exophytic H&N tumors. Moreover, in the oropharyngeal group, HPV status provided surprising and counterintuitive results: HPV-negative patients had higher primary tumor volume shrinkage compared to HPV-positive patients; however, this result is most likely due to having very low numbers in each branch.
The overall goal for the use of decision trees is to identify patients who are more likely to have significant tumor volume reduction during chemoradiotherapy. These volumetric changes can cause potential anatomical shifts during treatment and thus can alter the actual dose delivered to the target and OARs from the pretreatment planned course. Schwartz et al prospectively studied 24 patients with oropharyngeal squamous cell carcinoma. 3 All patients underwent daily in-room CT scan prior to treatment. By monitoring volumetric changes in the tumor and OAR and using the information from the scan to replan, the investigators were able to reduce mean ipsilateral and contralateral parotid dose by 3.9% and 2.8%, respectively. 3 Another prospective study reported on 20 patients treated with either postoperative or definitive chemoradiotherapy. 36 All 20 patients underwent ART using repeat CT scan at fraction number 15. A new adapted plan incorporating the volumetric changes was implemented at fraction number 20. The adapted plan resulted in an increase in PTV coverage of the primary tumor and a decrease in maximum dose to spinal cord and mean parotid dose. 36
The information obtained from the decision tree predicting for tumor volume reduction can also have prognostic implications. Yang et al performed adaptive planning on 76 patients with advanced oropharyngeal and hypopharyngeal cancers. 37 All patients underwent reimaging and adaptive replanning CT between weeks 4 and 5. In a multivariate analysis, primary GTV ≥30 mL and volume reduction less than 50% were prognostic for poor local control. 37
Our study is not intended to address the optimal timing of repeat imaging and replanning. The vast majority of patients were rescanned during the fourth week of treatment, which correlated with a median dose of 37.8 Gy. Several studies have hypothesized that repeat imaging approximately in the fourth or fifth week would allow adequate time for significant tumor reduction and anatomic changes to be clinically relevant. 37
The factors taken into consideration that may affect changes in tumor volume were limited to the ones that we could find in this retrospective setting. Although the number of patients included in this study was 48, the accuracies of predicting the tumor shrinkage based on these trees were very high (each 88%). A valid criticism can be raised concerning the lack of testing of the 2 decision tree algorithms. The high prediction accuracy of both decision trees (88%) represents a measure of goodness-of-fit statistic rather than results based on test instances. Thus, one does not necessarily need to test the decision tree on a select group as the prediction accuracy using decision tree algorithm can be interpreted similarly to root mean squared error or R2 metrics used in multivariate regression models. The prediction accuracy is a measure based on the existing data set only, which in turn, is a goodness of fit of the model to the whole data set. We could have tested the validity of the decision tree algorithm by using half (n = 24) of the original data set for test purposes. However, this would most likely have decreased the high prediction accuracy for both the decision trees in our study: even 1 (1 of 24) incorrect prediction would decrease prediction accuracy by 4%. Therefore in our analysis, all instances were used to develop the decision trees. The 2 models were able to predict the H/L tumor volume reduction for 42 of the 48 instances and were statistically significant.
Adaptive radiotherapy has been shown to improve clinical outcomes in patients with H&N cancer. 3,12 However, it is a time and resource demanding process, and not all patients will benefit from ART. A more prudent approach would be to selectively identify, in the pretreatment setting, patients who are likely to have high tumor volume reduction during RT. Our study demonstrates that decision trees predicting for tumor volume reduction during H&N RT can achieve this purpose. Our study is the first to date to implement an algorithm to identify the subset of patients based on pretreatment factors. However, a prospective trial is needed to validate the findings of our decision trees.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.