
Abstract
Intensity-modulated radiotherapy (IMRT) potentially leads to a more favorite dose distribution compared to 3-dimensional or conventional tangential radiotherapy (RT) for breast cancer after conservative surgery or mastectomy. The aim of this study was to compare dosimetric parameters of the planning target volume (PTV) and organs at risk (OARs) among helical tomotherapy (HT), inverse-planned IMRT (IP-IMRT), and forward-planned field in field (FP-FIF) IMRT techniques after breast-conserving surgery. Computed tomography scans from 20 patients (12 left sided and 8 right sided) previously treated with T1N0 carcinoma were selected for this dosimetric planning study. We designed HT, IP-IMRT, and FP-FIF plans for each patient. Plans were compared according to dose–volume histogram analysis in terms of PTV homogeneity and conformity indices (HI and CI) as well as OARs dose and volume parameters. Both HI and CI of the PTV showed statistically significant difference among IP-IMRT, FP-FIF, and HT with those of HT were best (P < .05). Compared to FP-FIF, IP-IMRT showed smaller exposed volumes of ipsilateral lung, heart, contralateral lung, and breast, while HT indicated smaller exposed volumes of ipsilateral lung but larger exposed volumes of contralateral lung and breast as well as heart. In addition, HT demonstrated an increase in exposed volume of ipsilateral lung (except for fraction of lung volume receiving >30 Gy and 20 Gy), heart, contralateral lung, and breast compared with IP-IMRT. For breast cancer radiotherapy (RT) after conservative surgery, HT provides better dose homogeneity and conformity of PTV compared to IP-IMRT and FP-FIF techniques, especially for patients with supraclavicular lymph nodes involved. Meanwhile, HT decreases the OAR volumes receiving higher doses with an increase in the volumes receiving low doses, which is known to lead to an increased rate of radiation-induced secondary malignancies. Hence, composite factors including dosimetric advantage, clinical effect, and economic burden should be taken into comprehensive consideration when choosing an RT technique in clinical practice.
Keywords
Introduction
Breast cancer is the most common cancer in females worldwide, and radiotherapy (RT) is a vital component in breast cancer management. 1,2 Conventionally, 2 tangential beams are used to treat the breast and chest wall tissue. Additional abutting megavoltage photon and electron fields are often added to treat the supraclavicular (SCV), axillary, and internal mammary lymph nodes. 3,4 Implementation of these complex treatments often results in heterogeneous dose distributions, particularly in the radiation field junctions, in which systematic increases in dose might result in fibrosis. 5 During the past 20 years, as external beam radiation therapy evolved from conventional wedged tangential radiation therapy (CR) into 3-dimensional conformal radiation therapy (3DCRT) and intensity-modulated radiation therapy (IMRT), treatment planning and delivery improved greatly. Up to date, there have been many literatures showing that IMRT including helical tomotherapy (HT), inverse-planned IMRT (IP-IMRT), and forward-planned field in field (FP-FIF) IMRT potentially leads to a more favorite dose distribution compared to 3DCRT or CR for the RT of breast cancer after breast-conserving surgery or mastectomy, 6 –19 but as for comparison of FP-FIF, IP-IMRT, and HT, the results of some published studies are contradictory. 7,9,14,18,20 –23 Therefore, the dosimetric superiority of HT over conventional IMRT for breast cancer remains questionable. In this study, we retrospectively analyzed the dosimetric and technical differences among HT, IP-IMRT, and FP-FIF in 20 patients with breast cancer who received conservative surgery and were previously irradiated with 3DCRT (4 cases with SCV regional lymph node involvement) on a comprehensive basis. We quantitatively compared the quality of treatment plans according to dose uniformity and conformity in breast volume and dose to the surrounding normal tissues of ipsilateral lung, heart contralateral breast, and lung.
Materials and Methods
Patient Selection, Positioning, and Computed Tomography Scanning
Computed tomography scans from 20 patients (12 left sided and 8 right sided) previously treated with T1N0 carcinoma at our hospital between July 2007 and May 2012 were analyzed. The inclusion of patients was not consecutive but based on logistics availability. The median age was 51.5 (range: 38-68) years. Patients were placed in the supine position on a breast board (Med Tec, Orange City, Iowa) with both arms raised above the head and sternum parallel to the couch. Lead wires were placed to locate breast, scar, and skin marks on the CT images. Patients were scanned from the level of the larynx to the level of the upper abdomen, including left and right lungs, with a 5-mm slice thickness and slice separations.
Target Volumes
The delineation of target and critical structures for all patients was done by a single radiation oncologist with extensive experiences in the treatment of breast cancer. For 16 cases without regional lymph node involvement, the clinical target volumes included breast defined as the glandular tissue apparent on CT scan and planning target volumes (PTV) included the breast parenchyma with a 3-mm rim of the skin removed. The retraction of the breast contour 3 mm from the skin surface was to account for dose buildup during dose calculation. For 4 cases with SCV lymph nodes, the whole PTVs consisted of the following 2 parts: PTV_up and PTV_down, PTV_up target volume meaning SCV nodes while PTV_down meaning the entire breast.
Critical Structures
The critical structures included the left and right lungs, the heart, and the contralateral breast. The esophagus, thyroid, and humeral head, although not mentioned in the following dose distribution analysis in this work, were also delineated.
Treatment Planning
All IP-IMRT and FP-FIF plans were designed using 6-MV photon beams of Elekta Precise accelerator (Elekta Precise, Elekta Oncology systems, West Sussex, United Kingdom) on the ADAC Pinnacle 3 planning system (version 9.2; Philips Radiation Oncology systems, Madison, Wisconsin), while HT planning was conducted on the Hi-Art4.1.2 (Version 4.1.2; TomoTherapy Inc., Madison, Wisconsin) treatment planning system. For each case, 3 IP-IMRT plans were created using alternative beam arrangement, including 2 standard tangential fields (2F), 4 fields (4F) with an additional 2 fields 20° to 30° posterior to the 2F technique, and 6 fields (6F) by adding 20° to 30° posterior to the 4F technique. To minimize the number of segments (NS) required per patient and reduce delivery times, the maximum NS in total, the minimum segment area (MSA) per segment, and the minimum number of monitor unit (MU) per segment were limited to ≤40, ≤4 cm2, and >4MU, respectively. The intensity modulation was achieved using the direct machine parameter optimization technique. In terms of FP-FIF, the tangential fields were used and 4- to 8-segment FIF modulation was used to homogenize the breast dose for each field. 24 For cases with SCV lymph node involvement, PTV_down was irradiated with the tangential fields with subsegments as mentioned earlier while PTV_up was treated using an additional single photon beam. For HT, the parameters affecting dose conformity and treatment times are the field width (FW), pitch, and modulation factor (MF). 25 The FW is defined by the fan beam width in the longitudinal direction. The pitch is defined as the ratio of the couch travel per gantry rotation to the FW and is required to be <1.0. The MF is defined as the intensity ratio between the most intense beamlet and the average of all the beamlets. Our study utilized a 2.5-cm FW, a pitch of 0.287 or 0.43, and an MF of 2.5. The prescribed dose to the PTV was 50 Gy in 2 Gy daily fractions. The dose–volume constraints used for the targets and critical structures are listed in Table 1, which were based on clinical experience in our clinic and kept the same for all plans.
Dose–Volume Constraints for Targets and Critical Structures.

Abbreviation: PTV, planning target volume.
Plan Comparisons
Dosimetric comparisons of plans were done based on the following parameters extracted from dose–volume histogram (DVH): homogeneity index (HI), conformity index (CI), Dmax, Dmin, and Dmean of PTV (Dmax: dose received by ≤2% volume of PTV, Dmin: dose received by ≥98% volume of PTV), 26 V30, V20, V10, and V5 of lung (fraction of lung volume receiving >30 Gy, 20 Gy, 10 Gy, and 5 Gy), V5 of heart (fraction of heart volume receiving >5 Gy), and V3 of contralateral breast (fraction of contralateral breast receiving >3 Gy). The HI was used to analyze the dose uniformity and defined as D5/D95 (the minimum dose in 5% of the PTV divided by the minimum dose in 95% of the PTV). The lower the HI, the better the dose homogeneity. The CI measured the degree of conformity and was calculated as follows 27 : CI = cover factor × spill factor, where the cover factor was defined as the percentage of the PTV receiving at least the prescribed dose and the spill factor as the volume of the PTV receiving at least the prescription dose relative to the total prescription dose volume. The closer the CI value is to 1, the better the dose conformity. Figure 1 shows the isodose distributions on a transverse plane of the 5 RT modalities for a typical patient.

Isodose distributions of HT and 3 types of IP-IMRT and FP-FIF plans are shown for a typical patient. IP-IMRT indicates inverse-planned intensity-modulated radiotherapy; FP-FIF, forward-planned field in field; HT, helical tomotherapy.
Statistical Analysis
Statistical analysis was performed using SPSS software (version 18.0, SPSS Inc, Chicago, Illinois). Quantitative data were expressed in the form of mean ± standard deviation (
Results
Comparison of HI, CI, Dmax, Dmin, and Dmean for Different Techniques
Dose–volume histogram plot of the 5 modalities for a typical patient for PTV was exported into the commercial software of MIM6.0.2 (MIMVista corp, Cleveland, Ohio) and is illustrated in Figure 2. The HI, CI, Dmax, Dmin, and Dmean that were explained earlier are presented for comparison of the 5 techniques in Table 2. In 1-way ANOVA, significant differences for HI were found (P = .000); further LSD test indicated that there were no significant differences between FP-FIF and 2F-IP-IMRT (P = .729), 2F-IP-IMRT and 4F-IP-IMRT (P = .944), and 4F-IP-IMRT and 6F-IP-IMRT (P = .513), while HT provided significantly better uniformity than any other techniques (P = .000, P = .000, P = .000, and P = .000). For CI, differences among the 5 techniques were statistically significant (P = .000); further LSD test showed that HT yielded superior CI compared with 3 types of IP-IMRT and FP-FIF (P = .000, P = .000, P = .000, and P = .000); meanwhile, significant difference was observed between IP-IMRT and FP-FIF (P = .001, P = .000, and P = .000). For Dmax, difference among the 5 techniques was statistically significant (P = .000); further LSD test showed that HT yielded smaller values than IP-IMRT and FP-FIF (P = .000, P = .000, P = .000, and P = .000), and no significant difference between IP-IMRT and FP-FIF was observed (P = .759, P = .844, P = .273). For Dmin, difference among the 5 techniques was statistically significant (P = .000), and further LSD test showed that HT yielded significantly larger values than IP-IMRT (P = .000, P = .002, P = .012), but no significant difference was observed between HT and FP-FIF (P = .128). It should be pointed out that 2F-IP-IMRT showed the smaller value compared with other 4 techniques (P = .011, P = .002, P = .000, and P = .000). For Dmean, significant differences were found among the 5 modalities (P = .000), and then LSD test showed that HT yielded smaller value than IP-IMRT and FP-FIF (P = .000, P = .000, P = .000, P = .000) and no significant difference was observed between IP-IMRT and FP-FIF (P = .626, P = .899, and P = .528).
Comparison of HI, CI, Dmax, Dmin, and Dmean for IP-IMRT, FP-FIF, and HT.

Abbreviations: CI, conformity index; FP-FIF, forward-planned field in field; HI, homogeneity index; HT, helical tomotherapy; IP-IMRT, inverse-planned intensity-modulated radiotherapy; Dmax, dose received by ≤2% volume of PTV; Dmin, dose received by ≥98% volume of PTV; PTV, planning target volume.

Dose–volume histograms of the 5 modalities for a typical patient are shown for planning target volume.
Comparison of Dosimetric Paramers of OARs for Different Techniques
Dosimetric parameters of organs at risk (OARs) including V5, V10, V20, and V30 of ipsilateral lung, V5 of heart, and V3 of contralateral breast and lung are listed in Table 3. The DVH plots for OARs of the 5 modalities were exported into MIM6.0.2 and are depicted in Figure 3.

Dose–volume histograms of the 5 modalities for a typical patient are shown for (A) ipsilateral lung, (B) contralateral lung, (C) contralateral breast, and (D) heart.
Comparison of Dosimetric Parameters of OARs for Different Techniques.
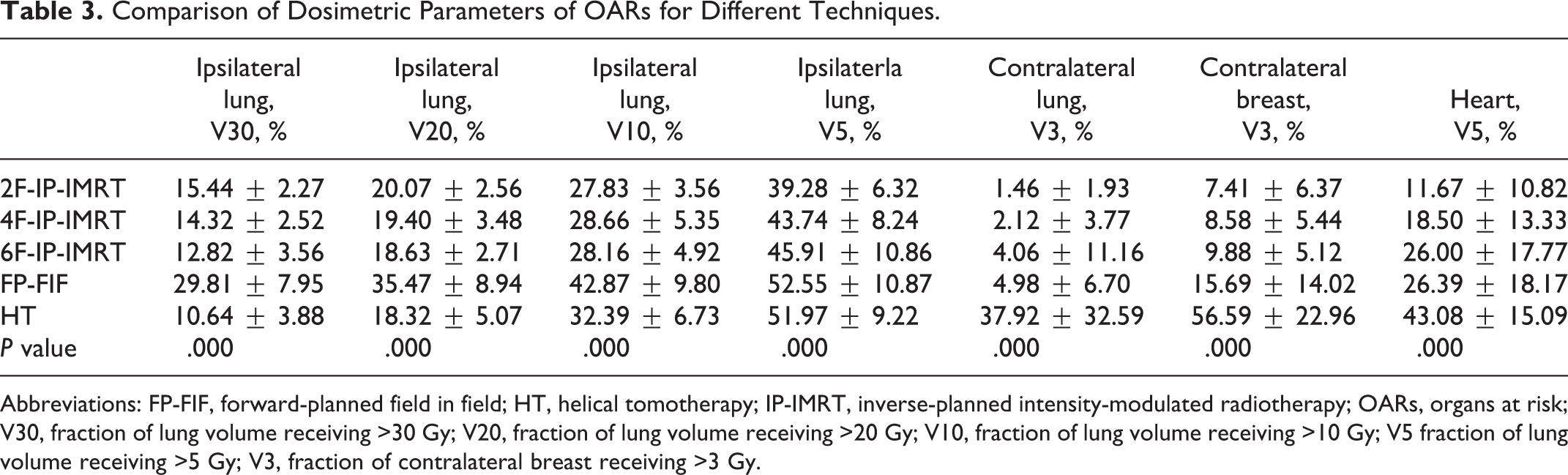
Abbreviations: FP-FIF, forward-planned field in field; HT, helical tomotherapy; IP-IMRT, inverse-planned intensity-modulated radiotherapy; OARs, organs at risk; V30, fraction of lung volume receiving >30 Gy; V20, fraction of lung volume receiving >20 Gy; V10, fraction of lung volume receiving >10 Gy; V5 fraction of lung volume receiving >5 Gy; V3, fraction of contralateral breast receiving >3 Gy.
V5 of heart, V30, V20, V10, and V5 of ipsilateral lung, and V3 of contralateral breast and lung all yielded significant differences (P = .000, P = .000, P = .000, P = .000, P = .000, P = .000, and P = .000) in 1-way ANOVA. Then, LSD test was used to analyze each parameter. For ipsilateral lung, (1) V30: IP-IMRT and HT spared more lung volumes than FP-FIF (P = .000, P = .000, P = .000, and P = .000), and the difference among 2F-IP-IMRT, 4F-IP-IMRT, and 6F-IP-IMRT was not significant (P = .434, P = .299, and P = .070). Specifically, no significant difference existed between 6F-IP-IMRT and HT (P = .130), while HT showed superiority to 2F-IP-IMRT and 4F-IP-IMRT (P = .001 and P = .012) in lung sparing; (2) V20: IP-IMRT and HT spared more lung volumes than FP-FIF (P = .000, P = .000, P = .000, and P = .000), and no significant differences were found between any 2 IP-IMRT techniques (P = .680, P = .631, and P = .373). Although the difference was not statistically significant, HT scored relatively smaller value than 3 IP-IMRT modalities (P = .281, P = .504, and P = .850); (3) V10: The values of IP-IMRT and HT were significantly smaller than FP-FIF (P = .000, P = .000, P = .000, and P = .000). There existed no significant difference between any 2 IP-IMRT modalities (P = .683, P = .807, and P = .869). The value of HT was significantly larger than that of 2F-IP-IMRT and 6F-IP-IMRT (P = .027 and P = .040) and relatively larger than that of 4F-IP-IMRT (P = .070); and (4) V5: IP-IMRT yielded significantly smaller value than FP-FIF and HT (P = .000, P = .003, and P = .026; P = .000, P = .006, and P = .041). No difference was found between FP-FIF and HT (P = .842). For V3 of contralateral breast, HT covered significantly larger volume than IP-IMRT and FP-FIF, respectively (P = .000, P = .000, P = .000, and P = .000), and no significant difference existed between any 2 IP-IMRT modalities (P = .773, P = .748, and P = .543) while 2F-IP-IMRT covered significantly smaller volume than FP-FIF (P = .044) and other 2 IP-IMRT techniques covered relatively smaller volume than FP-FIF (P = .082 and P = .155). For V3 of contralateral lung, HT covered significantly larger volume than any other technique (P = .000, P = .000, P = .000, and P = .000). For V5 of heart, HT involved significantly larger volume than IP-IMRT and FP-FIF (P = .000, P = .000, P = .001, and P = .001) while 2F-IP-IMRT involved smaller volume than 6F-IP-IMRT and FP-FIF (P = .004 and P = .003) and relatively smaller volume than 4F-IP-IMRT (P = .161).
Treatment Delivery Efficiency
The treatment time estimates for all plans are shown in Table 4. The HT MUs are on the average 84%, 74%, 63%, and 87%, greater than 2F-IP-IMRT, 4F-IP-IMRT, 6F-IP-IMRT, and FP-FIF, respectively. It is clear that the delivery time is dependent on the MUs in the plan.
Number of MU and Treatment Time Estimates for Each Planning Modality.

Abbreviations: FP-FIF, forward-planned field in field; HT, helical tomotherapy; IP-IMRT, inverse-planned intensity-modulated radiotherapy; MU, monitor unit; min, minutes.
Discussion
Before 2010, the routine technique for the patients receiving breast-conserving surgery is conventional parallel-opposed tangential RT technique in our clinic. In case of SCV lymph node involvement, a single anterior oblique beam will be added. Advantages of IMRT have been discussed by some studies, 12,28 –30 but the results are contradictory. For example, a study by Dogan et al 30 found that 4-field IMRT achieved better sparing of ipsilateral lung and contralateral breast than 2-field IMRT while studies by Fong et al, 12 Landau et al, 28 and Thilmann et al 31 indicated that 4-field IMRT or multi-field increased dose to ipsilateral lung and contralateral breast compared with 2-field IMRT, respectively. The studies of Caudrelier et al, 7 Hijal et al, 20 and Qiu et al 23 demonstrated that V5, V10, and V20 of ipsilateral lung and V5 of heart in HT were lower than those in FP-FIF, while the study by Goddu et al 22 showed that V5 of ipsilateral lung for HT was higher than that in FP-FIF. Moreover, an analysis by Schubert et al 21 indicated that V5, V10, and V20 of ipsilateral lung and V5 of heart in HT were higher than those in IP-IMRT and FP-FIF. In our study, we observed a superiority in both uniformity and conformity of breast dose with HT compared to both IP-IMRT and FP-FIF. The mean HI decreases from 1.18 for FP-FIF to 1.13 for HT, while the mean CI increases from 0.51 for FP-FIF to 0.74 for HT. Furthermore, compared with IP-IMRT and FP-FIF, HT exposed smaller volumes of ipsilateral lung at dose level higher than 20 Gy; however, HT demonstrated an increase in irradiated volumes to ipsilateral lung at dose levels lower than 10 Gy compared with any of the 3 IP-IMRT techniques, while FP-FIF covered largest volume at this dose level. In addition, IP-IMRT and FP-FIF exposed smaller volumes of contralateral lung, breast, and heart than HT in low-dose area. Treatment planning time and effort for FP-FIF and HT plans were significantly greater than those for IP-IMRT (approximately 60-90 minutes for FP-FIF, 120-240 minutes for HT, and approximately 25-40 minutes for IP-IMRT). The FP-FIF plans require planners with advanced treatment planning skills to try different combinations of collimator angles and weights of open field and subsegment in order to get clinically accepted plans. In designing HT plans, planner needs to try different combination of FW, pitch, and MF and beamlet calculation, and following optimization process is time consuming while IP-IMRT plans can be generated in less time in a more automated fashion. The CI values appear low, especially in FP-FIF and 2F-IP-IMRT, but we have defined a complex PTV, which includes not only the whole breast but also the SCV nodes in several patients, which is similar to the results of published studies. 7,32,33
Breast radiation oncology has been, in the past decades, evolving with 2 main goals, improving target coverage and subsequent disease control while sparing normal tissue and reducing patient toxicity. The IMRT technique has been used to meet the requirement and avoid late toxicity such as pneumonitis, lung fibrosis, and coronary heart disease which has been reported by several trials. 34 –36 However, the excellent target coverage is achieved at the expense of a low-dose exposure to ipsilateral lung and contralateral breast and lung. This low-dose effect is known to lead to an increased rate of radiation-induced secondary malignancies. 37 –42 In our study, for the protection of OARs, HT yielded lower percentage of irradiated volume than IP-IMRT and FP-FIF in high-dose area, but higher percentage in low-dose area, which was probably caused by increased beam angles from HT. It should be pointed out that all dosimetric parameters of ipsilateral lung and contralateral breast and lung as well as heart in FP-FIF were higher than those in IP-IMRT even in low-dose area although the MUs of FP-FIF was the lowest, which is in contrast to the common opinion that the leakage and scatter dose to nontarget tissues of the patients will be proportional to the number of MUs used. 19,43 Lesser degree of modulation of FP-FIF and complexity of the target may be the reason. Up to now, only skin reactions from several techniques are reported to be different which is significant to the cosmetic effects, 44 and clinical trials and long-term follow-up may be required to evaluate the clinical significance of the dosimetric characteristics with HT.
One issue to be considered is patient motion. Inter- and intrafraction motion is taken into account with standard tangential fields by the use of flash and adequate margins. 45 For FP-FIF, the majority of the dose is delivered by the open field, so flash is assumed to still be effective. For IP-IMRT and HT, however, flash is not straightforward to achieve, so the accuracy of setup in IP-IMRT and HT should be paid more attention, which can be improved by means of breath gating and imaging guidance techniques. The impact of breathing motion on plan delivery is currently under investigation using 4-dimensional computed tomography and breath control device in our department. Other considerations such as increased economic burden of more sophisticated techniques remain unaddressed.
Conclusions
For breast cancer RT after conservative surgery, HT provides better dose homogeneity and conformity of PTV compared with 3 modalities of IP-IMRT techniques and FP-FIF technique. It should be emphatically pointed out that for patients with SCV lymph nodes involved, HT demonstrated uncomparable advantage over IP-IMRT and FP-FIF in target coverage. On the other hand, HT decreases the OAR volumes receiving higher doses with an increase in the volumes receiving low doses probably due to more scattered irradiation, which is known to lead to an increased rate of radiation-induced secondary malignancies such as cancer of contralateral breast and lung. Hence, composite factors including dosimetric advantage, clinical effect, and economic burden should be taken into comprehensive consideration when choosing an RT technique in clinical practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Military Medical Metrology Foundation (No.2011-JL2-005).