
Abstract
The objective of this study is to compare the new and conventional tomotherapy treatment techniques and to evaluate dosimetric differences between them. A dosimetric analysis was performed by comparing planning target volume (PTV) median dose, 95% of PTV dose coverage, Paddick conformity index (CI), homogeneity index (HI), whole-body integral dose, and OAR median doses. The beam on time (BOT) and the effect of different jaw sizes and pitch values was studied. The study results indicated that the PTV dose coverage for all the techniques was comparable. Treatment plans using dynamic jaw reduced OAR doses to structures located at the treatment field edge compared to fixed jaw plans. The HT-3DCRT plans resulted in higher OAR doses to kidney, liver, and lung compared to the other techniques, and TD-IMRT provided the best dose sparing to liver compared to other techniques. Whole-body integral dose differences were found to be insignificant among the techniques. BOT was found to be higher for fixed jaw treatment plan compared to dynamic jaw plan and comparable between all treatment techniques with 5-cm dynamic jaw. In studying effect of jaw size, better OAR sparing and HI were found for 2.5-cm jaw but at the expense of doubling of BOT as compared to 5-cm jaw. There was no significant improvement found in OAR sparing when the pitch value was increased. Increasing the pitch from 0.2 to 0.43, the CI was improved, HI improved only for 5-cm jaw size, and BOT decreased to approximately half of its original time.
Introduction
Craniospinal irradiation (CSI) is usually a component in the treatment of medulloblastoma and other central nervous system tumors that have a propensity to spread throughout the cerebrospinal fluid. The CSI target is a large and complex-shaped target; hence, the biggest challenge is achieving satisfactory target volume coverage while maintaining the dose homogeneity inside the target volume and minimizing the toxicity by reducing the dose to the normal structures. 1,2 The conventional treatment technique used for CSI patients has been 3-dimensional conformal treatment technique (3DCRT) using a linear accelerator; however, issues with junction doses between the cranial and spinal fields still pose a problem. 3 Proton therapy has the potential advantage of decreased integral dose to pediatric patients, but the degree of clinically meaningful benefit from proton CSI from a toxicity standpoint is subject to uncertainty because of the absence of convincing clinical evidence with appropriate follow-up to determine both tumor control and toxicity. 4,5
Helical tomotherapy (HT) allows treatment of large volumes (40 × 160 cm2) and also offers clear advantages for CSI patients over treatment with conventional 3DCRT, in particular the superior dose deposition patterns in the avoidance of organs at risk (OARs) and minimization of the junction problems that are inherent to conventional 3DCRT. 6 However, the trade-offs using HT are longer beam on time (BOT) and increased integral dose. 6 –8 The conventional tomotherapy treatment mode is called helical mode, which delivers treatment with 360° gantry rotation while the patient table is translating. In its original versions, HT could only deliver the treatment with intensity-modulated radiation therapy (IMRT) technique with selected fixed binary jaws (HF-IMRT). Subsequently, helical tomotherapy 3DCRT technique mode was added to the tomotherapy system (HT-3DCRT), which delivers the treatment with 3DCRT technique. Most recently, a new mode called TomoDirect (TD) was added to the tomotherapy system. The TD technique allows the delivery of radiation at predetermined fixed gantry angles and it can deliver the treatment with IMRT (TomoDirect IMRT with dynamic jaws (TD-IMRT) or 3DCRT (TD-3DCRT) techniques. In the latest TomoHDA V2.0 system, the fixed jaw has been replaced by a dynamic jaw, which uses smaller jaw size in the craniocaudal direction of each target to improve the superior and inferior dose penumbra. In summary, currently the new TomoHDA V2.0 system (Accuracy Inc, Sunnyvale, California) has 2 delivery modes, TomoHelical and TomoDirect, and each of these delivery modes has 2 options of plan mode: IMRT and 3DCRT. The treatment plans have 2 options to choose: dynamic jaw or the fixed jaw. In this study, only the original HF-IMRT technique used fixed jaw; whereas, other treatment techniques used dynamic jaw.
The newly released treatment modes enable the tomotherapy system to treat patients with additional treatment options; however, the reported clinical available data related to TomoDirect and HT-3DCRT modes are very limited, especially for CSI patients. In this article, a comparison study was performed between HF-IMRT, helical tomotherapy IMRT with dynamic jaws (HD-IMRT), TD-IMRT, and HT-3DCRT techniques. A dosimetric comparison was performed to investigate the differences between different treatment techniques on target coverage, dose homogeneity within the target, and normal tissue sparing. The BOT and integral dose were also evaluated and compared between all the available techniques to investigate the potential issues of longer treatment time and larger integral dose for tomotherapy treatments.
Methods
Ten CSI patients treated previously with HF-IMRT in our department were selected for this study. The same CT image data sets were used to replan the patients using other currently available treatment techniques such as HT-3DCRT, HD-IMRT, and TD-IMRT. The original HF-IMRT treatment plans were generated using tomotherapy Hi-Art version 4.0.4 TPS (Accuracy Inc) with a fix jaw size of 5 cm, a pitch of 0.287, and a modulation factor of 2.0. The delineation of targets, OARs, prescription, and optimization parameters were described elsewhere. 9 Briefly, planning target volume (PTV)-brain and PTV-spine were combined to create the treatment PTV (brain plus spine), and the patient was prescribed with 23.4 Gy to 95% of the PTV in 13 treatment fractions. For the comparison purposes, all patients in this study were replanned with the same prescription and fraction doses.
The HD-IMRT plans were retrospectively created using tomotherapy Hi-Art version 5.0 TPS (Accuracy Inc) with the same optimization parameters as HF-IMRT plans with the exception of using dynamic jaws rather than fixed jaws. The TD-IMRT and HT-3DCRT plans were also created on the same 5.0 TPS with the same pitch, modulation factor, and 5-cm dynamic jaws. The TD-IMRT plans were generated with 6 beam angles placed at 0°, 95.5°, 132.8°, 180°, 225.0°, and 260.5°. The same 10 patients were used to investigate the effect of jaw size by regenerating HT-3DCRT plans with 2.5-cm dynamic jaw (HT-3DCRT-2.5cm). Similarly, new HT-3DCRT plans with pitch values of 0.2, 0.3, and 0.43 were generated for only 1 CSI patient to study the effect of different pitch values. Directional blocks were placed in the direction of lenses and arm structures in TD-IMRT and HT-3DCRT plans. Tissue inhomogeneity correction was turned on for dose calculation in all the plans.
The quantitative evaluation of PTV dose distribution was performed by median dose to PTV (D
median), the lowest PTV dose received by at least 95% of the volume (D
95), Paddick conformity index (CI), and homogeneity index (HI). Conformity index was defined by the following equation
10
:

where TV is the target volume, TVPIV is the target volume covered by the prescription isodose volume, and VPIV is the total prescription isodose volume. Since TVPIV and VPIV could not obtained directly from HT treatment planning station, the patient contours and doses were then transferred to MIM software (MIM Software Inc, Cleveland, Ohio), and these parameters were obtained from the dose–volume histogram calculated by MIM software. Homogeneity index was defined by the following equation
3
:

where Dx is the dose to the x% of the target volume. According to International Commission on Radiation Units and Measurements report 62, 11 D 98% is near the minimum dose and D 2% is near the maximum dose. Plan evaluation parameters for OARs included the maximum dose for lens, and median dose of bilateral lung, bilateral kidney, heart, liver, rectum, and bladder. Beam on time was also evaluated in this study. An analysis of variance (ANOVA) Scheffe multigroup statistical study was performed to compare the differences among these treatment techniques as well as differences among individual specific treatment techniques. A Student t test was also used for the field size comparison between 5- and 2.5-cm jaw. Values of P ≤ .05 were considered significant.
Results
Planning Target Volume Dose Coverage (5-cm Jaw)
Median values and ranges of PTV D median, D 95, CI, HI, and BOT for 10 patients using different tomotherapy treatment techniques are listed in Table 1. For 5-cm jaw plans, the ANOVA Scheffe multigroup statistic study showed that there was slightly statistically significant difference (P = .024) for PTV D median between different treatment techniques. However, the difference existed only between HF-IMRT and TD-IMRT techniques (P = .035). Table 1 also shows that the ratio of D 95 and the prescription dose (23.4 Gy) was very close to 1, indicating that the PTV coverage satisfied the prescription requirement for all the techniques with no statistically significant difference (P = .983). Considering CI and HI, the results showed no statistically significant differences for CI (P = .101) and HI (P = .323) between different treatment techniques. For the BOT comparison, HF-IMRT technique had longer BOT compared to HD-IMRT, TD-IMRT, and HT-3DCRT techniques. All the plans with 5-cm dynamic jaw had comparable BOT.
Median and Range for PTV D median, D 95, CI, HI, and BOT for 10 Patients Using Different Techniques With 5-cm Jaw.a

Abbreviations: ANOVA, analysis of variance; BOT, beam on time; CI, conformity index; HD-IMRT, helical tomotherapy IMRT with dynamic jaws; HF-IMRT, helical tomotherapy IMRT with fixed jaws; HT-3DCRT, helical tomotherapy 3DCRT technique; HI, homogeneity index; IMRT, intensity-modulated radiation therapy; PTV, planning target volume; TD-IMRT, TomoDirect IMRT with dynamic jaws; 3DCRT, 3-dimensional conformal treatment technique.
a P value is the statistical comparison results from ANOVA Scheffe multigroup test.
Normal Tissue Sparing (5-cm Jaw)
The median values and ranges of OAR median doses for 10 patients using different treatment techniques with 5-cm jaw are listed in Table 2. The results showed slightly significant differences for doses to bladder (P < .023); however, the individual comparison between each specific technique showed no significant differences. For dose to rectum, the ANOVA test showed statistically significant difference (P < .0001) between different treatment techniques. More specifically, HF-IMRT gave the highest rectum dose compared to HD-IMRT, TD-IMRT, and HT-3DCRT techniques with dynamic jaw. This indicated that the plans using dynamic jaw technique had increased OAR dose sparing in the superior and inferior directions of the target compared to fixed jaw technique (Figure 1).

Rectum median doses for HF-IMRT, HD-IMRT, TD-IMRT, and HT-3DCRT techniques. IMRT indicates intensity-modulated radiation therapy; HF-IMRT, helical tomotherapy IMRT with fixed jaws; HD-IMRT, helical tomotherapy IMRT with dynamic jaws; TD-IMRT, TomoDirect IMRT with dynamic jaws; HT-3DCRT, helical tomotherapy 3DCRT technique.
Median and Range for OAR D median for 10 Patients Using Different Treatment Techniques With 5-cm Jaw.a

Abbreviations: ANOVA, analysis of variance; HD-IMRT, helical tomotherapy IMRT with dynamic jaws; HF-IMRT, helical tomotherapy IMRT with fixed jaws; HT-3DCRT, helical tomotherapy 3DCRT technique; IMRT, intensity-modulated radiation therapy; OAR, organ at risk; TD-IMRT, TomoDirect IMRT with dynamic jaws; 3DCRT, 3-dimensional conformal treatment technique.
a P value is the statistical comparison results from ANOVA Scheffe multigroup test.
The results also showed statistically significant differences for doses to liver (P < .001), kidney (P < .001), lung (P < .001), and heart (P < .001) between different treatment techniques with 5-cm jaw. To compare the differences between any 2 specific treatment techniques, the result showed that TD-IMRT gave best liver dose sparing among all the techniques; both TD-IMRT and HT-3DCRT delivered higher heart dose than HF-IMRT and HD-IMRT; HT-3DCRT plans gave higher kidney, liver, and lung doses compared to other 3 treatment techniques. Nevertheless, in all cases, OAR doses were well below the clinically accepted tolerance level recommended by RTOG 0615. 11
The whole-body integral dose was also studied, and the results are listed in Table 2. The median integral dose comparison showed no statistically significant difference (P = .1592) between different treatment techniques; hence, the CSI patients received comparable integral dose from all the available tomotherapy treatment techniques.
Effect of Jaw Size (5- vs 2.5-cm Jaw)
The effect of jaw size was studied using HT-3DCRT technique, and median values and ranges of PTV D median, D95 , CI, HI, and BOT for 10 patients for jaw size of 5 and 2.5 cm are shown in Table 3.
Median and Range for PTV D median, D 95, CI, HI, and BOT for 10 Patients Using HT-3DCRT Technique With 5- Versus 2.5-cm Jaw.a

Abbreviations: BOT, beam on time; CI, conformity index; HT-3DCRT, helical tomotherapy 3DCRT technique; HI, homogeneity index; PTV, planning target volume; 3DCRT, 3-dimensional conformal treatment technique.
a P value is the statistical comparison results from Student t test.
Student t test was performed for comparing the effect of jaw size. The result showed statistically significant difference for PTV D median between 5- versus 2.5-cm jaw plans (P < .001). However, it was not clinically significant, as the median dose difference between them was less than 1%. The results also showed no statistically significant differences for D 95 (P = .1823) and CI (P = .2752) and statistically significant difference for HI (P = .0003) between 5- and 2.5-cm jaw plans. The plan with 2.5-cm jaw provided better dose homogeneity while requiring twice the BOT compared to 5-cm jaw plan. The median values and ranges for OAR median doses for 10 patients for 5- and 2.5-cm jaw plan using HT-3DCRT technique are shown in Table 4.
Median and Range for OAR D median for 10 Patients Using HT-3DCRT Technique With 5- Versus 2.5-cm Jaw.a

Abbreviations: HT-3DCRT, helical tomotherapy 3DCRT technique; OAR, organ at risk; 3DCRT, 3-dimensional conformal treatment technique.
a P value is the statistical comparison results from Student t test.
There were statistically significant differences between 5- and 2.5-cm jaw plans for all the OARs doses (P < .001) except for the lens doses. The treatment plans with 2.5-cm jaw were found to spare more OAR doses.
Effect of Pitch Value
The dosimetric differences for different pitch values were studied, and the PTV D median, D 95, CI, HI, and BOT for 5- and 2.5-cm jaw are listed in Table 5.
The PTV D median, CI, HI, and BOT for Different Pitch Values Using HT-3DCRT Technique.
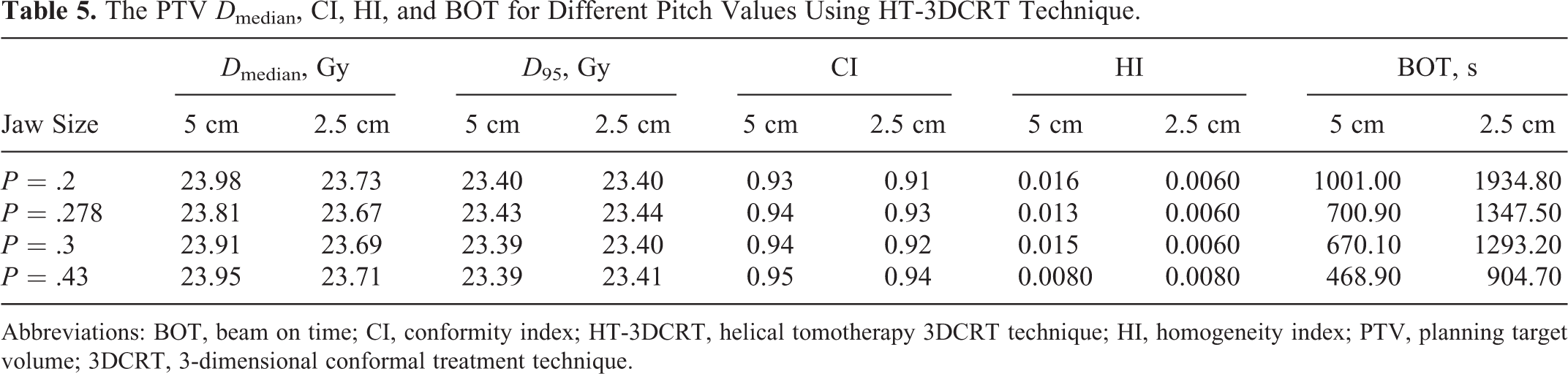
Abbreviations: BOT, beam on time; CI, conformity index; HT-3DCRT, helical tomotherapy 3DCRT technique; HI, homogeneity index; PTV, planning target volume; 3DCRT, 3-dimensional conformal treatment technique.
Table 5 shows that the PTV dose coverage was not significantly changed with different pitch values. The CI was worse, HI was improved, and the BOT was almost doubled when changing the jaw from 5- to 2.5-cm for all different pitch values. When pitch values was increased from 0.2 to 0.43, CI increased for all jaw sizes, and HI improved only for 5-cm jaw while the HI did not significantly changed for 2.5-cm jaw. Beam on time was increased to almost twice when decreasing pitch from 0.43 to 0.2.
The OAR median doses corresponding to different pitch values are listed in Table 6. The OAR doses did not significantly change when pitch values were changed from 0.43 to 0.2 for both the 5- and 2.5-cm jaw plans. When the jaw size was changed from 5 to 2.5 cm, the OAR doses decreased correspondingly.
The OAR Median Doses for Different Pitch Values Using HT-3DCRT Technique.
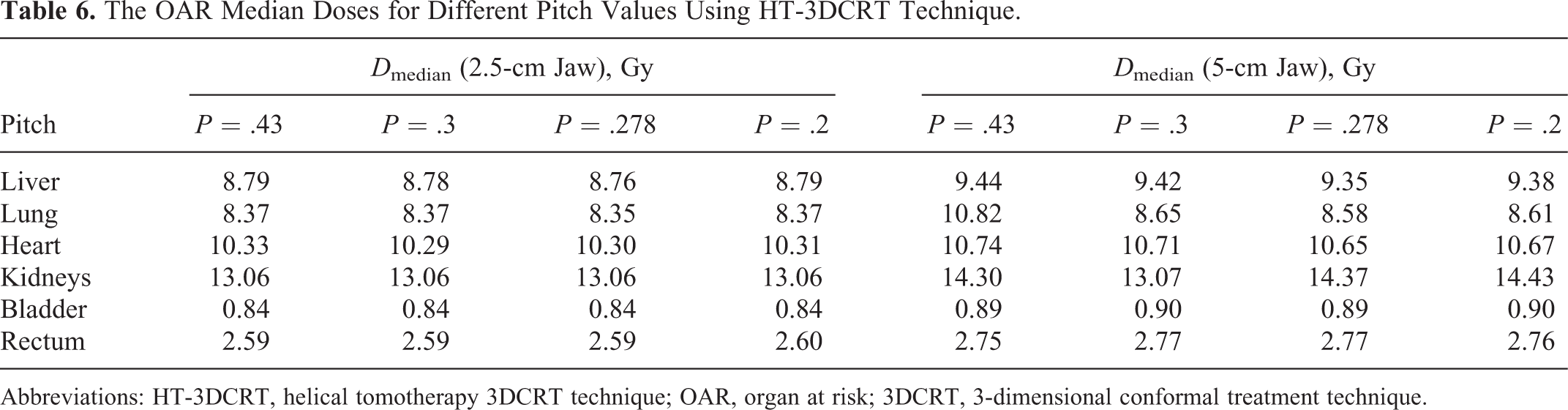
Abbreviations: HT-3DCRT, helical tomotherapy 3DCRT technique; OAR, organ at risk; 3DCRT, 3-dimensional conformal treatment technique.
Discussion
Ten previously treated CSI patients were selected and replanned to investigate the dosimetric differences between currently available tomotherapy treatment techniques. The CSI patient treatment plans were generated using HF-IMRT, HD-IMRT, TD-IMRT, and HT-3DCRT treatment techniques. The PTV dose coverage, CI, and HI for all the techniques were found to be similar. The key differences between these techniques were found in dose to OAR structures.
Techniques with dynamic jaw effectively reduced the OAR doses for rectum compared to fixed jaw techniques, which can be explained by the fact that dynamic jaw technique used smaller jaw sizes in the craniocaudal direction of the target volume where the rectum was contiguous to the target volume. The same explanation could be applied for changing the jaw size from 5 to 2.5 cm.
The TD treatment technique is relatively new, and several published studies have already investigated the possibility of decreasing the treatment time and OAR doses using TD technique. 12,13 As demonstrated in this study, TD technique plans spared more liver dose than other treatment techniques, which was in close agreement with the report published by Murai et al. In this article, they examined TD technique in treatment of prostate, lung, and thoracic wall tumors. The main reason TD technique spared more liver dose than other helical mode techniques is that TD technique has the capability to avoid beam going through liver by manipulating the beam angles. They also reported that TD technique spared more lung dose as well. In our study, the ANOVA Scheffe multigroup statistical study showed that only HT-3DCRT technique received significantly more lung dose than the other 3 IMRT techniques. There were not any statistical significant differences found between any IMRT techniques. The OAR dose could be further reduced by optimizing the beam angles in order to avoid certain anatomical sites, such as lens. Hence, TD might be an efficient technique to deliver radiation at static angles while avoiding the radiation beam traversing through critical structures.
The BOT was found to be similar between all 5-cm dynamic jaw plans. This was also consistent with the report published by Murai et al, 12 in which it was reported that TD technique did not reduce total treatment time. Langner et al 14 reported that TD technique plans could be delivered with comparable treatment time as conventional 3DCRT plans, and in shorter times than a helical mode tomotherapy plan. However, in that study, TD-3DCRT mode was used, whereas in the current study, TD-IMRT treatment technique was used. Traditionally, CSI treatment used conventional linear accelerator-based 3DCRT technique to deliver 2 lateral (90° and 270° angle) beams to the cranial area, and 1 to 2 posterior beams to the spinal area. To mimic the conventional linear accelerator beam arrangement using TD-3DCRT technique, virtual blocks would be needed to block the brain and spine area individually. Our initial investigation showed that PTV dose homogeneity and conformity were inferior to those generated by HF-IMRT planning, which was found to be consistent with the Langner et al study. Therefore, the TD-3DCRT technique was replaced by the TD-IMRT treatment techniques in the current study, which allowed for more beam angles and optimization similar to HF-IMRT plans.
The HT-3DCRT treatment technique is still a relatively new mode in the Hi-Art tomotherapy system. It is easier and faster to generate a treatment plan compared to other treatment technique plans. For all the HT-3DCRT treatment plans, the PTV dose coverage satisfied the prescription requirements; however, HT-3DCRT plans received higher OAR doses compared to any other IMRT treatment plan. The lens dose needs to be paid more attention since HT-3DCRT technique does not have the option to optimize the lens dose. According to RTOG 0615, the maximum lens dose tolerance is 25 Gy. However, the OAR dose tolerance levels from RTOG 0615 are for adult patients and caution should be used when extrapolated to young adult and pediatric patients. We optimized the lens dose to much lower dose than the RTOG 0615 requirement, and the average dose was around 11 Gy or less. Blocking the lens directionally or completely would directly affect the PTV dose coverage due to the proximity of the lens to the PTV. Therefore, for some CSI patients, HT-3DCRT is not a treatment option.
We studied the effect of different jaw sizes and pitch value using only HT-3DCRT technique, because this mode provides limited number of variables that can be changed prior to dose calculation. However, for HF-IMRT, HD-IMRT, and TD-IMRT techniques, the dose to each OAR structure can be optimized with flexibility of changing a large number of variables. Therefore, these techniques can provide different optimal solutions for the same plan. This may not be a fair comparison. Hence, HT-3DCRT technique was used as the only technique to study the jaw size and pitch value effect. No improvement in PTV dose coverage was found by changing the field size from 5- to 2.5-cm jaw. However, better OAR dose sparing and HI improvement were achieved for the jaw size of 2.5 cm but at the expense of doubling of BOT which ultimately can lead to an increase in intrafraction motion and whole-body integral dose. Increasing the pitch values from 0.2 to 0.43 did not significantly improve the PTV coverage or OAR sparing; however, the CI and HI were improved, and the BOT decreased.
Previous studies reported 6 –8 that integral dose was higher for HT techniques compared to conventional Linac-based 3DCRT techniques. In this study, we also evaluated the integral dose between different tomotherapy techniques. No significant difference in integral dose was found between all the available tomotherapy techniques.
Conclusion
The newly available HT-3DCRT, HD-IMRT, and TD-IMRT techniques can all be used in tomotherapy treatment plans for CSI patients in addition to previously treated treatment plans with HF-IMRT technique. They all provided comparable PTV dose coverage; however, these new techniques possess individual unique characteristics. Plans using dynamic jaw were found to be superior to fixed jaw in terms of OAR sparing in the superior and inferior directions of field edge. The TD-IMRT technique can be used preferentially to treat patients who have critical organs that are very difficult to spare by other techniques. The TD-IMRT could be used to further reduce the OAR doses by selecting certain beam angles that could avoid the beam going directly through the OAR structures of interest. Moreover, TD-IMRT technique did not reduce the BOT for CSI treatment. The HT-3DCRT can be used as a simple and fast technique for CSI treatments; however, HT-3DCRT plans received higher OAR doses compared to other IMRT treatment plans. Changing the jaw size from 5 to 2.5 cm, OAR doses were better spared, and HI was also improved but at the expense of doubling of BOT. Increasing the pitch values from 0.2 to 0.43 produced insignificant improvements in PTV coverage and OAR dose sparing; however, CI and HI were improved and significantly reduced the BOT.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.