
Abstract
Introduction
Lung particle therapy using pencil beam scanning achieves high dose conformity but remains vulnerable to geometric uncertainties from suboptimal initial setup. Surface-guided radiotherapy (SGRT) improves setup reproducibility in photon workflows, yet evidence in lung particle therapy remains limited. This study evaluates the clinical value of SGRT in improving six degrees of freedom (6-DOF) setup reproducibility in lung cancer particle therapy.
Methods
This retrospective cohort study analyzed 63 lung cancer patients receiving 1277 treatment fractions at our center from February 2023 to January 2024. Comparisons were made between conventional laser-based positioning, which included 983 fractions, and SGRT workflows, which included 294 fractions. Following patient positioning, therapists manually registered orthogonal kilovoltage (kV) x-ray images with planning digitally reconstructed radiographs (DRRs) to calculate 6-DOF correction parameters, including translational (lateral, longitudinal, vertical) and rotational (pitch, roll, yaw) components, and to quantify the pre-correction setup error . Absolute 6-DOF displacements and three-dimensional vector magnitudes (MAG) were measured. The analysis included 36 supine patients with 739 treatment fractions and 27 prone patients with 538 fractions.
Results
The SGRT group exhibited statistically significant reductions in median shifts for lateral (0.25 cm to 0.21 cm, p = 0.021), longitudinal (0.25 cm to 0.21 cm, p = 0.014), pitch (1.0° to 0.8°, p = 0.001), and MAG (0.59 cm to 0.53 cm, p = 0.002) compared to conventional methods. These improvements in median values were more pronounced in supine-positioned patients, while no significant differences were observed in prone-positioned patients. Furthermore, substantial reductions were achieved in ninth decile deviations (1.09 cm to 1.03 cm), and the third quartile deviations (0.83 cm to 0.74 cm) in the overall cohort.
Conclusion
SGRT enhances setup precision for proton and carbon ion lung cancer radiotherapy, reduces pre-correction setup error, and provides clinical support for patient setup reproducibility.
Keywords
Introduction
Lung cancer persists as the principal contributor to global cancer burden, with the highest incidence and mortality rates worldwide. 1 Radiotherapy constitutes a cornerstone of lung cancer therapeutic management, 2 where proton and carbon ion therapy are increasingly adopted for their advantages of physical dose distribution and relative biological effectiveness.3,4 Pencil beam scanning exploits the Bragg peak phenomenon to optimize tumor dose conformity while minimizing exposure to normal tissues.4,5 However, it is also more sensitive to geometric uncertainties. Factors such as positioning errors, posture reproducibility, anatomical structural variations, respiratory motion, and thoracic morphological changes may lead to mismatches between the delivered and planned dose distributions.6,7
Conventional particle therapy workflows rely on external lasers and skin markers for initial alignment, followed by position verification and adjustments using orthogonal radiographic imaging or cone-beam CT (CBCT) prior to treatment delivery. 8 The accuracy of initial positioning heavily depends on the therapists’ positioning skills and subjective judgment, potentially leading to significant positioning deviations that may even be challenging to correct through imaging techniques, especially for complex anatomical sites such as the thorax.
Surface-guided radiotherapy (SGRT) employs real-time visible light surface imaging technology to provide continuous three-dimensional (3D) surface monitoring in the treatment room, based on reference surface contours acquired from CT scans or treatment-room surface imaging. This 3D surface information, requiring no additional x-ray exposure, can be utilized not only for real-time monitoring of intra-fractional motion during treatment, but also provides corrective references for body posture during the patient setup phase.9–11 SGRT has thus been recognized for its potential to enhance patient setup accuracy and reproducibility, especially in scenarios where conventional setup references are insufficient.
Current clinical research on SGRT in lung cancer treatment remains relatively limited, particularly regarding its application in fixed-beam particle therapy, where diverse positioning approaches are required for lung cancer patients. A comparison between conventional laser-alignment protocols and SGRT in clinical particle therapy settings for supine cases is essential. This study aims to conduct a retrospective analysis of lung cancer patients set up with SGRT system assistance at our institution, quantitatively comparing inter-fractional errors between SGRT-assisted and conventional setup methods. The findings will evaluate the clinical value of SGRT in enhancing inter-fractional setup accuracy for lung cancer patients and provide clinical evidence for optimizing setup reproducibility using SGRT technology in thoracic-abdominal particle therapy.
Methods
Study Design and Patient Enrollment
This retrospective cohort study enrolled lung cancer patients undergoing particle radiotherapy at our institution between February 2023 and January 2024. Eligible patients met the following inclusion criteria:
Pathologically or radiologically confirmed lung cancer, including non-small cell lung cancer and small cell lung cancer, receiving radical radiotherapy; Ability to maintain stable prone or supine positioning during treatment; Utilization of the institution's SGRT system during treatment sessions.
The final cohort included 63 patients who underwent a total of 1277 treatment fractions, with 36 patients treated in supine position completing 739 fractions and 27 prone-positioned patients completing 538 fractions. Treatment fractions were assigned to the SGRT-assisted group based on system availability during treatment cycles, while the remaining fractions were included in the non-SGRT group according to standard clinical workflow. In total, 294 fractions were analyzed in the SGRT-assisted group and 983 fractions in the non-SGRT group. The sample size was determined by the total number of consecutive eligible patients treated during the predefined study period in this retrospective analysis.
The study was approved by the Institutional Review Board of our institution (ethics approval No. 250724EXP-01), Registration date: July 29, 2025, with a waiver of informed consent due to its retrospective nature. All patient data were de-identified and anonymized prior to analysis. All methods were performed in accordance with relevant guidelines and regulations, and the reporting of this study conforms to the STROBE guidelines. 12 All procedures complied with the ethical standards of the Helsinki Declaration of 1975, as revised in 2024.
Simulation and Setup Strategy
All patients were immobilized in supine or prone positions using a head-and-neck board (Klarity Medical, Guangzhou, China), head holder and thorax thermoplastic mask, or an abdomen board (Klarity Medical, Guangzhou, China), head holder, vacuum cushion and thorax thermoplastic mask. CT simulation was obtained through SOMATOM Definition AS (Siemens Healthineers, Erlangen, Germany) in spiral scanning mode with a thickness of 3 mm. Thermoplastic masks ensured positional consistency during CT scanning and subsequent treatments.
SGRT-assisted patient setup and postural adjustments were implemented before securing the thermoplastic immobilization mask to the patient. However, the securing of thermoplastic masks alters surface morphological characteristics while simultaneously blocking the optical system's direct observation of the skin adjacent to the target area, thereby hindering the acquisition of valid setup reference surface from planning CT. The representative surface contours and the mask-induced morphological deformations in both supine and prone positions are visualized in Figure 1. To address this technical limitation, our institution implemented a supplementary workflow wherein a mask-free CT scan was acquired prior to planning CT acquisition and thermoplastic mask immobilization. This mask-free imaging served to establish the reference surface contours for the SGRT system.

Visual demonstration of immobilization setups for lung cancer patients in supine and prone positions, and changes in body surface contours before and after mask fixation. Representative surface images are shown for prone (A) mask-free; (B) immobilized and supine (C) mask-free; (D) immobilized positions. The mask-free surfaces (A, C) serve as the regions of interest (ROIs) for initial surface-guided setup. (E) Comparison of surface contours illustrating mask-induced deformation. The upper panel displays the mask-free scan, whereas the lower panel shows the planning CT acquired under thermoplastic mask immobilization. The pink contour represents the reference body surface acquired prior to immobilization. A significant deviation is evident in the planning CT between the body contour and the pink reference contour, demonstrating that the surface geometry altered by the mask is unsuitable for initial surface-guided setup.
The SGRT system employed in this study was the Catalyst HD (C-RAD AB, Sweden). The Catalyst HD system is an optical surface imaging-based SGRT platform that projects structured light patterns, including approximately 528 nm green and 624 nm red wavelengths, onto the patient's surface via a projector and captures reflected light through cameras. The system reconstructs three-dimensional surface images of the patient based on optical triangulation principles. During registration, Catalyst HD employs a modified non-rigid iterative closest point (ICP) algorithm to perform six degrees of freedom (6-DOF) alignment by calculating real-time deviations between the patient's current surface and reference surface contour, while generating real-time three-dimensional discrepancy maps. 13
The respiratory gating was implemented in this study to monitor all patients, utilizing a belt sensor (Anzai Medical, Tokyo, Japan) to acquire respiratory waveforms. The four-dimensional computed tomography (4DCT) simulator was employed to acquire planning CT images by three CT phases within 20% of maximum respiratory amplitude around the end-exhalation phase. Image reconstruction was performed by calculating the mean Hounsfield unit (HU) values of these images. 14 Reference surface contours were delineated on mask-free CT imaging using the Whole Body Contour tool in MIM software (MIM, Cleveland, USA). These regions of interest (ROIs) were subsequently transferred to planning CT through rigid registration based on couch coordinate positions, thereby establishing the reference surface for SGRT system alignment during patient setup. The reference surface encompassed anatomical range extending from the nasal tip to 5 cm below the diaphragm, ensuring full-surface data acquisition including upper extremities, head-neck region, and thoracoabdominal areas.
Comparison of Patient Positioning Workflows
The positioning procedures were performed by a rotating team of 22 radiation therapists, with a median professional experience of 9 years at our institution.
Non-SGRT Group: After patient placement, therapists determined couch positions by referencing the first-treatment or simulation room couch values and vacuum cushion alignment marks. Patient posture was adjusted to align surface markers with external lasers. Orthogonal x-ray images were acquired for positional verification after thermoplastic masks were secured.
SGRT-assisted Group: Following patient lying down, therapists used the same initial couch positioning method as the non-SGRT group. The Catalyst HD system was then utilized to obtain real-time 6-DOF couch correction parameters and 3D surface discrepancy maps, which were displayed on the in-room screen. Based on this information, therapists adjusted patient posture to align thoracic, head-neck, and arm positions with the reference surface. Initial positioning was deemed complete when surface isocenter deviations fell within 3 mm/3°, with no significant surface discrepancy zones. Thermoplastic masks were subsequently secured, and orthogonal x-ray images were acquired for positional verification.
Data Acquisition and Parameter Definitions
By matching bony landmarks and tumor imaging characteristics, orthogonal x-ray images were registered with digitally reconstructed radiographs (DRRs) to obtain 6-DOF couch shift parameters: lateral (LAT), longitudinal (LNG), vertical (VRT), PITCH, ROLL, and YAW. The 3D vector magnitude (MAG) was calculated using the following formula:

Therapists executed 6-DOF couch shifts based on x-ray registration results to complete pre-treatment positional corrections. The 6-DOF displacement values from each treatment session were recorded and analyzed. Smaller absolute values of these parameters indicated lower deviations between the initial patient positioning and the treatment plan, reflecting higher initial positioning accuracy. This study compared the absolute 6-DOF couch shift values and MAG between SGRT-assisted and non-SGRT fractions, with subgroup stratification by supine/prone to evaluate differences between the two positioning methods. The positioning and verification procedures for both workflows are illustrated in Figure 2.

Schematic workflow of patient positioning and verification procedures for surface-guided radiotherapy-assisted and non-surface-guided radiotherapy groups.
Statistical Analysis
Given sample sizes below 5000 cases, normality was first assessed using the Shapiro-Wilk (S-W) test. The S-W test yielded p < 0.001 for all parameters, rejecting the null hypothesis of normal distribution. Consequently, the Mann-Whitney U test for independent samples was employed to compare the medians of positioning accuracy between SGRT-assisted and non-SGRT fractions. The interquartile range, defined by the first quartiles (Q1) and third quartiles (Q3), was used to characterize the error distribution. Additionally, the 90th percentile (D9) was calculated to quantify the large setup deviations. The significance level was uniformly set at p < 0.05.
Results
Table 1 demonstrates that SGRT-assisted setup significantly reduced couch shifts in LAT, LNG, and MAG. Compared to conventional laser-based setup, the median shifts in LAT and LNG directions decreased by 16% from 0.25 cm to 0.21 cm (p = 0.021) and 18% from 0.25 cm to 0.21 cm (p = 0.014), respectively, while MAG decreased by 10% from 0.59 cm to 0.53 cm (p = 0.002). For rotational shifts, the median rotation in PITCH decreased by 20% from 1.0° to 0.8° (p < 0.001), whereas no significant differences were observed in YAW or ROLL (p > 0.05).
Comparison of Six Degrees of Freedom Setup Errors and Three-Dimensional Vector Magnitude in Lung Cancer Patients with and Without Surface-Guided Radiotherapy Assistance.

Note: *p < 0.05, **p < 0.01. lateral [LAT], longitudinal [LNG], vertical [VRT], 3D vector magnitude [MAG], rotational [YAW, PITCH, ROLL]. 75th percentile [Q3], 90th percentile [D9].
SGRT implementation also led to a marked decrease in extreme setup deviations, with the D9 values for LAT, LNG, and VRT decreased from 0.62 cm to 0.51 cm, 0.70 cm to 0.59 cm, and 0.73 cm to 0.69 cm, respectively, while the MAG declined from 1.09 cm to 1.03 cm. Consistent reductions were also observed for rotational errors at D9, with YAW decreasing from 1.6° to 1.5°, PITCH from 2.2° to 2.0°, and ROLL from 1.9° to 1.6°. Similar trends were observed at Q3, with LAT, LNG, VRT and MAG reducing from 0.42 cm to 0.38 cm, 0.47 cm to 0.40 cm, 0.48 cm to 0.46 cm, and 0.83 cm to 0.74 cm, respectively. These findings indicate that SGRT enhances both the central tendency and the control of outlier deviations in patient setup, ensuring greater overall positioning precision.
Figure 3 illustrates the distribution of MAG with and without SGRT assistance. In the non-SGRT group, 62.9% of fractions exhibited MAG exceeding 0.5 cm, whereas this proportion dropped to 55.4% with SGRT assistance. Similarly, the proportion of displacements exceeding 1.0 cm fell from 13.9% to 11.6%. Furthermore, the maximum values of 6-DOF couch shifts and MAG in the SGRT-assisted setup group were lower than those in the non-SGRT group, demonstrating a reduction in the frequency and magnitude of extreme setup deviations.
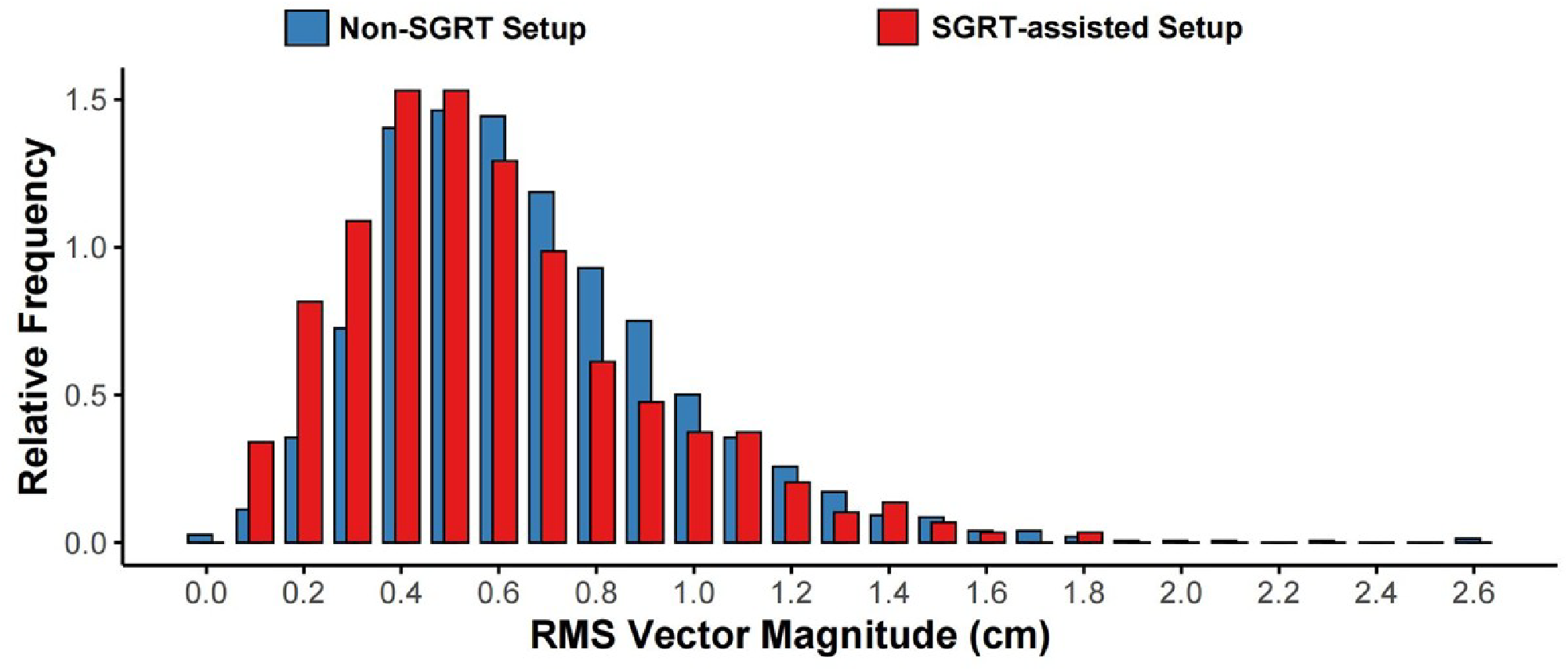
Cumulative histogram comparison of three-dimensional vector magnitude between surface-guided radiotherapy-assisted and non-surface-guided radiotherapy setup in lung cancer patients.
Table 2 shows that for supine-positioned lung cancer patients, SGRT-assisted setup significantly reduced the median shift in the VRT from 0.30 cm to 0.22 cm (p = 0.009) and MAG from 0.55 cm to 0.49 cm (p = 0.002). The median shift in the LNG remained at 0.20 cm, but statistical significance was observed (p = 0.046) due to a decrease in the first quartile from 0.10 cm to 0.07 cm and in the third quartile from 0.39 cm to 0.32 cm, indicating improved consistency. For rotational axes, the median PITCH decreased from 1.0° to 0.7° (p < 0.001). Reductions in extreme deviations were also observed. Specifically, maximum, D9, and Q3 values for all 6-DOF parameters and MAG showed notable decreases. These results indicate that SGRT implementation in supine patients improves both the median and extreme values of setup accuracy in translational and rotational dimensions.
Comparison of Six Degrees of Freedom Setup Errors and Three-Dimensional Vector Magnitude in Supine-Positioned Lung Cancer Patients with and Without Surface-Guided Radiotherapy Assistance.

Note: *p < 0.05, **p < 0.01. lateral [LAT], longitudinal [LNG], vertical [VRT], 3D vector magnitude [MAG], rotational [YAW, PITCH, ROLL]. 75th percentile [Q3], 90th percentile [D9].
In contrast, Table 3 shows that in prone-positioned lung cancer patients, SGRT-assisted positioning did not result in significant reductions in the median values of 6-DOF shifts or MAG (all p > 0.05). However, SGRT was associated with reductions in extreme deviations, with maximum errors in LAT, LNG, VRT, and MAG consistently lower in the SGRT group compared to controls, as well as reductions at both D9 and Q3. The data indicate that, although improvements in median setup accuracy were not significant for prone-positioned patients, SGRT was effective in decreasing the magnitude of extreme setup deviations.
Comparison of Six Degrees of Freedom Setup Errors and Three-Dimensional Vector Magnitude in Prone-Positioned Lung Cancer Patients with and Without Surface-Guided Radiotherapy Assistance.

Note: *p < 0.05, **p < 0.01. lateral [LAT], longitudinal [LNG], vertical [VRT], 3D vector magnitude [MAG], rotational [YAW, PITCH, ROLL]. 75th percentile [Q3], 90th percentile [D9].
Figure 4 compares the 3D vector magnitude between SGRT-assisted and non-SGRT setup groups for supine and prone postures. The results demonstrate that in both positions, the SGRT group exhibited lower maximum values, Q3, median, and D9 in 3D vector magnitude compared to the non-SGRT group.

Box plots with scatter points comparison of three-dimensional vector magnitude between surface-guided radiotherapy-assisted and non-surface-guided radiotherapy setup groups for supine and prone-positioned lung cancer patients.
Discussion
This study presents an assessment of SGRT for enhancing initial setup accuracy in lung cancer patients undergoing proton and carbon ion therapy, including both supine and prone positions. Particle therapy exhibits a significantly higher sensitivity to anatomical variations compared to photon radiotherapy, requiring a rigorous assessment of range uncertainties for each beam orientation during the treatment planning process. For lung tumors located near the posterior thoracic wall or the posterior mediastinum, posterior or posterior-oblique beam angles are typically preferred to minimize the path length through lung and mitigate associated range uncertainties. Furthermore, the sharp distal dose fall-off characteristic of particle beams is strategically utilized to provide superior protection for critical organs at risk such as the heart. 15 To our knowledge, this work is the first to systematically evaluate SGRT-assisted setup in prone-positioned lung cancer patients, hence addressing a previously unstudied area within the context of particle therapy using fixed-beam nozzles. By filling this gap, our findings extend the evidence base for SGRT applications in complex thoracic-abdominal cases.
SGRT offers significant advantages over conventional laser-based alignment by enabling non-contact, ionizing radiation-free real-time surface monitoring, providing enhanced setup reference information for thoracic-abdominal patients compared to traditional laser-based alignment.16,17 This technology addresses several limitations of conventional setup, particularly the lack of capability to verify arm and shoulder positioning, thereby improving reproducibility in complex thoraco-abdominal cases.18,19
It is important to clarify the scope and intent of the present study. This work does not evaluate SGRT as a replacement for radiographic image guidance, but rather focuses on a posture-correction–oriented SGRT workflow based on mask-free CT reference surfaces. Within this workflow, surface guidance is used to assist therapists in correcting patient posture prior to rigid x-ray–guided couch adjustment. Consequently, the reduction in setup errors observed on orthogonal x-ray–based positioning reflects the effectiveness of this workflow and highlights the role of SGRT in mitigating non-rigid setup discrepancies that cannot be addressed by couch shifts alone.
The SGRT-assisted group exhibited consistently lower maximum errors in all six degrees of freedom, as well as reduced 3D vector magnitude, compared to the non-SGRT group in both supine and prone positions. Particularly for the worst 10% of fractions (D9), SGRT reduced pre-correction setup error by 0.05–0.20 cm in translational directions and 0.1°–0.5° in rotational axes. Such extreme errors are more likely to induce patient deformation, which cannot be corrected through rigid x-ray–guided couch corrections, highlighting SGRT's potential to enhance treatment precision.
Further analysis showed that the SGRT-assisted group achieved median shift reductions of 16%, 18%, and 10% in lateral, longitudinal, and 3D vector magnitude respectively, along with a 20% reduction in pitch shifts compared to the non-SGRT group. These improvements are primarily attributed to the higher postural stability of supine-positioned patients, in whom SGRT significantly optimized longitudinal, vertical, pitch shifts, and 3D vector magnitude. These findings align with trends observed in breast cancer studies reporting SGRT-mediated error reductions across all directions. 20 However, the lack of significant improvement in the vertical direction may relate to inter-fraction and intra-fraction variations in respiratory baselines, a phenomenon also investigated in studies by Takao et al. 21 and Jensen et al. 22
Despite these advantages in supine positioning, our analysis indicates that SGRT provides only limited improvements for prone-positioned patients. Although the SGRT cohort exhibited reduced D9, Q3, and maximum values for 3D vector magnitude compared to controls, no statistically significant reduction was observed in the median values of setup errors across translational or rotational axes, including 3D vector magnitude. This limitation likely stems from the use of individualized vacuum cushions in prone positioning, which restricted therapists’ capacity for postural modifications despite SGRT guidance. Enhancing positioning reproducibility for prone-positioned patients remains a critical area for future investigation.
Several limitations of this study warrant consideration. First, the application of SGRT in lung radiotherapy is predicated on a coupling between surface topography and internal anatomical structures. Although this study confirms that SGRT improves global setup reproducibility, it remains unclear whether alignment of the external surface concurrently ensures reproducible positional relationships between key local anatomical structures—such as the scapula, spine and the tumor target. Future research should move beyond global setup residual analysis by attempting to quantify the relative positions of multiple ROIs, thereby further clarifying the unique value of SGRT in mitigating postural deformations. Furthermore, improvements in setup reproducibility should ultimately lead to better preservation of target dose coverage. In particle therapy, even small anatomical variations along the beam path can affect dose coverage, and optimized initial positioning may help reduce dose degradation that cannot be corrected by rigid couch shifts. This interpretation is supported by Gorgisyan et al, who showed that dose degradation in proton therapy for non-small cell lung cancer is associated with both breath variability and setup reproducibility. 23 Therefore, future prospective studies using CT-on-rail imaging and dose recalculation are needed to directly evaluate the dosimetric impact of SGRT-assisted setup. Finally, the operational efficiency of the clinical workflow is limited by both algorithmic settings and simulation protocols. In the treatment room, the Catalyst system defaults to a 6 s temporal averaging window when calculating 6-DOF couch shifts to mitigate the impact of respiratory motion on positioning. Reducing this averaging interval to 4 s or 0 s, could accelerate patient setup. During simulation, an additional mask-free scan is currently required to generate valid reference surfaces. Future optimization could involve phantom studies to determine whether low-dose CT sequences provide equivalent surface contours, thereby reducing radiation exposure. Alternatively, installing multi-camera optical surface imaging systems directly in the CT simulator may enable rapid acquisition of complete optical surface references.
Conclusion
In this analysis of 1277 treatment fractions, SGRT-assisted initial setup reduced the magnitude of extreme positioning deviations in proton and carbon ion lung cancer radiotherapy for both supine and prone positions. Significant reductions in couch shift were observed in the lateral, longitudinal, pitch, and 3D vector magnitude, with the greatest improvements in supine cases. These findings support the clinical adoption of SGRT to enhance the reproducibility and accuracy of patient setup in particle therapy.
Footnotes
Abbreviations
Acknowledgements
We thank Xinyue Zhang from the Institute of Neuroscience, Chinese Academy of Sciences, for her contribution to the preparation of the figures in this study.
Ethics Approval Statement
This study was approved by the Institutional Review Board of Shanghai Proton and Heavy Ion Center (ethics approval No. 250724EXP-01). The committee reviewed and approved the study protocol on July 30, 2025, ensuring that the secondary analysis of de-identified electronic health records was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2024. This approval is valid from July 2025 to July 2026. All methods were performed following the relevant national guidelines, including China's Good Clinical Practice (GCP) and the Measures for Ethical Review of Life Sciences and Medical Research Involving Humans.
Informed Consent Statement
The requirement for informed consent was waived by the Institutional Review Board of Shanghai Proton and Heavy Ion Center because of the retrospective nature of the study.
Author Contributions Statement
All authors have made significant contributions to this study and meet the established criteria for authorship.
Funding
The study was supported by Noncommunicable Chronic Diseases-National Science and Technology Major Project (2024ZD0519900, 2024ZD0519901); Shanghai Municipal Health Commission (2024ZZ2054).
The funders had no role in the study design, sample selection, data collection, data analysis, data interpretation, manuscript preparation, or the decision to submit.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets analyzed during the current study are available from the corresponding author on reasonable request.