
Abstract
Introduction
Image-guided radiotherapy (IGRT), with various types of pretreatment image guidance, is essential for reducing geometric uncertainties that can affect not only the clinical target volume-planning target volume (CTV-PTV) margin (tumor control probability) but also the normal tissue complication probability.1–3 Therefore, studies have shown that an effective immobilization device can reduce setup errors and lead to better treatment outcomes.4–8 Six-dimensional (6D) setup errors, including 3 translations (vertical, longitudinal, and lateral) and 3 rotations (roll, yaw, and pitch), can be detected by cone beam computed tomography (CBCT) and corrected by 6D couches. As we all know, most modern linear accelerators (LINACs) have 6D couches available as an option, and all modern proton systems utilize 6D couch corrections. However, some LINACs not equipped with 6D couches ignore roll and pitch corrections, which may affect the translational setup errors during registration. To our knowledge, only a few studies have investigated the impact of rotational corrections on translational shifts.9,10 This study aims to quantitatively compare the 6D setup errors of different immobilization systems for 6 body regions based on CBCT with a particular focus on rotational setup errors. Furthermore, for the region and immobilization device which was significantly affected by rotational setup errors, the impact on radiotherapy dose distribution was analyzed by using an adult anthropomorphic phantom.
Materials and Methods
The reporting of this study conformed to STROBE guidelines. 11 This study was approved by the Ethics Committee of our institute (SDTHEC2022001033). Two hundred ninety patients with pretreatment CBCT images from 3835 fractions were retrospectively analyzed for brain, head & neck, chest, abdomen, pelvis, and breast cases. All patient details were de-identified. The detailed immobilization and imaging strategies are shown in Table 1. For each patient, the CBCT image of the radiation region was scanned and matched with the corresponding kV planning CT on a TrueBeamTM or VitalBeamTM (Varian Medical Systems) IGRT workstation. The scanning scheme was once before each of the first 3 radiotherapy fractions and 1 or 2 times per week depending on the immobilization reproducibility in the first 3 fractions. CBCT was performed before each stereotactic body radiotherapy (SBRT) and breast cancer radiotherapy fraction. The breast CBCT images were automatically registered by a grayscale protocol to the planning CT images, and a bone protocol was used for the other body regions. Then, experienced radiation oncology physicians performed a manual adjustment to strictly match the tumor target. When image registration was completed, the 6D setup errors for each fraction of each patient were recorded before any correction was applied. The means and standard deviations were calculated using the absolute values for the translational and rotational errors of each immobilization device for every patient. All parameters were compared between the different immobilization devices for the chest, abdomen, pelvis, and breast regions.
Case Distribution and Pretreatment CBCT Fractions Grouped by Immobilization Device for Each Body Region.

Abbreviation: CBCT, cone beam computed tomography.
The kV fan beam planning CT images of an anthropomorphic adult phantom (ATOM, Computerized Imaging Reference System Inc.) were acquired on a Philips Brilliance Big Bore CT and reconstructed at a 3 mm slice thickness, which simulated the shape as well as specific internal organs of an adult man. To investigate the impact of rotational errors on translational shifts, the phantom was set up on the couch of the Varian VitalBeamTM system, and CBCT images were collected for registration with the planning CT images. Figure 1 shows the anthropomorphic adult phantom lying on the 6D couch and the translational and rotational axes. The artificial rotational setup errors of the phantom were simulated by tilting the treatment couch in the pitch and roll directions by ±2° and ±3°, respectively, and rotating the couch in the yaw direction by ±2°, ±3°, ±4°, and ±5°. After CBCT images were obtained at each simulated position, they were matched with the kV planning CT by rigid 6D and 3-dimensional (3D) registration. Therefore, 2 groups of translational errors from both the 6D and 3D registration and one group of rotational errors from the 6D registration were acquired. The difference between the 2 groups of translational errors was compared.

The anthropomorphic adult phantom on the couch of the radiotherapy system marked with translational coordinate axis and rotational modes.
Considering that the target reproducibility of radiotherapy after breast-conserving surgery was sensitive to setup accuracy12,13 and that the errors from the supine breast bracket were substantial,14,15 an anthropomorphic adult phantom with artificial breasts was generated and simulated with different rotational errors on the Siemens SOMATOM Drive CT system (Figure 2). Pitch rotations were artificially simulated by quantitatively adjusting the angles of the supine breast bracket by −2.5° and +2.5°. During the plan design period, yaw and roll rotations were simulated by rotating the couch and gantry of the medical LINAC by ±3.0°, respectively. A left breast irradiation treatment plan was designed on a Varian EclipseTM treatment planning system based on phantom CT images. The fixed-field intensity-modulated radiotherapy (IMRT) plan for 6 MV x-ray was designed with the PTV as the target. The prescription dose was 50 Gy/25 f for routine segmentation. The plan objectives were PTV-V50 Gy ≥ 95%, PTV Dmax < 107%, both lungs V5 Gy < 20%, V20 Gy < 10%, heart Dmean < 6 Gy and V30 Gy < 46%. The IMRT plans used 4 coplanar fixed fields to adjust the intensity, and the field angles were 115°, 130°, 150°, and 304°. Although maintaining plan parameters such as the isocenter position, the field angle, and the multileaf grating subfield sequence, the plan was transplanted into the CT images space with different axial rotations, and the dose was recalculated to simulate the real dose distribution received by the patients with the rotational errors caused by radiotherapy positioning. Dosimetry comparisons on the PTV and organs at risk (OARs) were performed between the simulated rotational plans and the original plan without rotations by using dose-volume histogram (DVH) curves. Target volume coverage was assessed as the volume of the PTV receiving 50 Gy (V50 Gy).

The anthropomorphic phantom with the breasts lying on the couch for CT simulation and immobilized by a supine breast bracket.
Statistical Analysis
Statistical analysis was performed using commercially available statistical software (IBM SPSS Statistics, version 26.0). Continuous variables were presented as the mean ± standard deviations and illustrated with a box plot. We used the Kolmogorov-Smirnov test and determined that the variables were nonnormally distributed (P < .05). In this way, we proceeded with a nonparametric approach using the Wilcoxon test for comparing the errors between different immobilization devices for the chest, abdomen, pelvis, and breast regions; the Mann-Whitney U test or the Kruskal-Wallis test and then the Dunn test (with P values adjusted using the Benjamini-Hochberg method) were applied for multiple comparisons. The level of significance was defined as P < .05.
Results
6D Setup Errors
The statistical means and standard deviations of the setup errors for different regions and immobilization devices are shown in Table 2. Almost all the mean translational setup errors were <5 mm, and all of the mean rotational setup errors were <2°. The box plots of the distributions of the translational and rotational deviations and statistical analyses regarding the difference comparison of error values obtained for each direction from different immobilization devices in the chest, abdomen, pelvis, and breast regions are shown in Figure 3 and Figure 4, respectively.

Box plots and P value representations. The distributions of translational deviation values among the different immobilization devices for the chest (a), abdomen (b), pelvis (c), and breast (d) regions. Box plots show the means, medians, and 25th and 75th percentiles; the whiskers represent the maximum and minimum values.
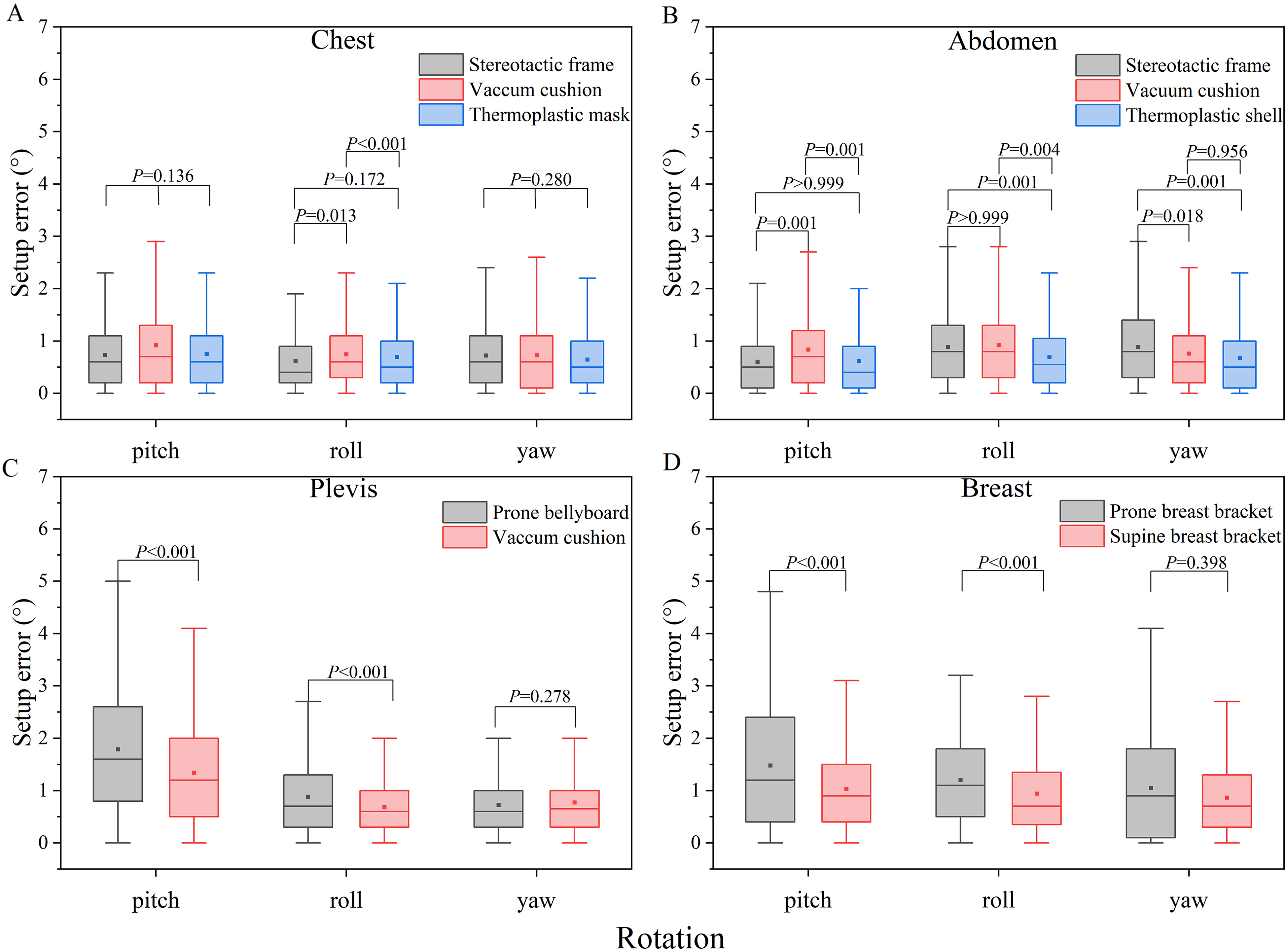
Box plots and P value representations. The distributions of rotational deviations values among the different immobilization systems for the chest (a), abdomen (b), pelvis (c), and breast (d) regions. Box plots show the means, medians, and 25th and 75th percentiles; the whiskers represent the maximum and minimum values.
Means and Standard Deviations of the Setup Errors for Different Regions and Immobilization Devices.a
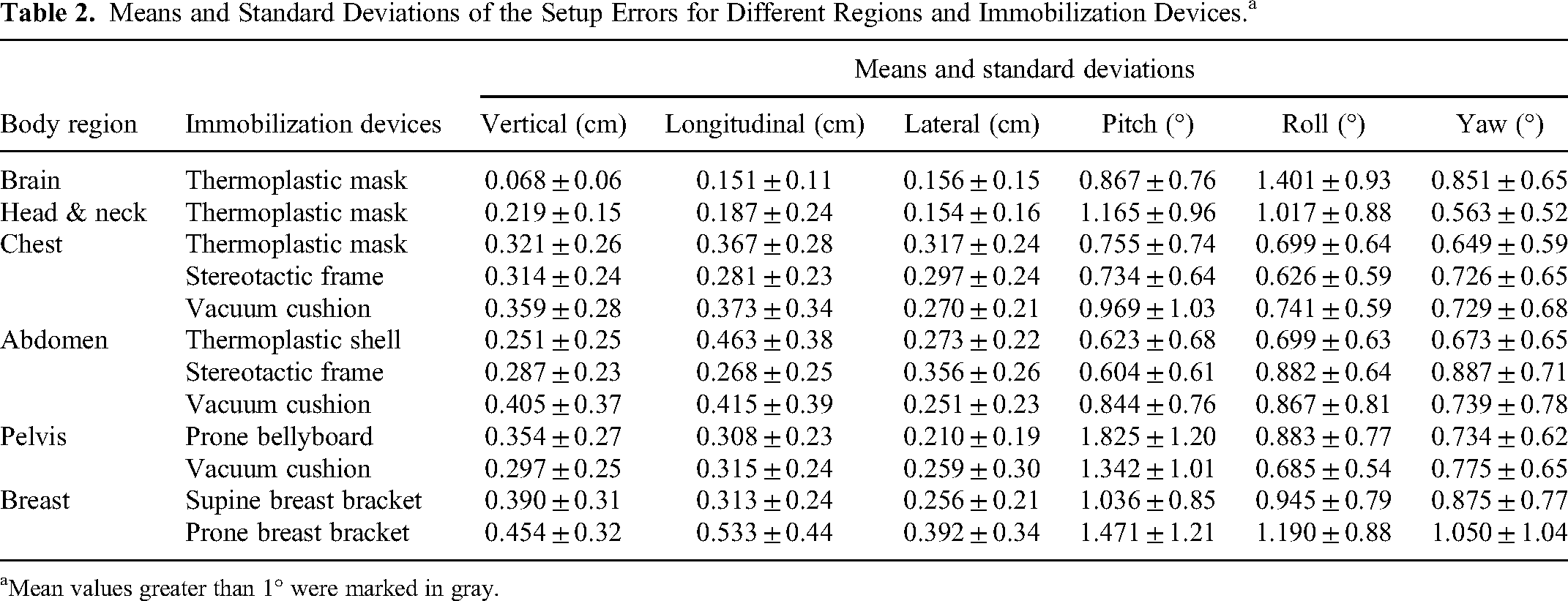
Mean values greater than 1° were marked in gray.
In the chest region, the errors of the stereotactic frame in the longitudinal direction were smaller than those of the vacuum cushion and thermoplastic mask. The errors of the vacuum cushion were greater than those of the stereotactic frame and thermoplastic mask in the roll direction. The differences in the remainder of the directions did not show a significant difference. In the abdomen region, the differences in all directions reached significance. For the pelvic tumor cases, the errors were significantly different between the 2 groups in the vertical, pitch, and roll directions, in which the errors of the prone bellyboard were greater than those of the vacuum cushion. For the breast region, all of the errors were greater in the prone breast bracket, and all the differences reached significance except for those in the yaw direction.
Impact of Rotational Errors on Translational Shifts
The results of the difference between the 2 groups of translational errors are shown in Figure 5. Uncorrected pitch mainly caused changes in the anteroposterior (z-axis) and cephalocaudal (y-axis) directions. Uncorrected yaw mainly caused changes in the cephalocaudal (y-axis) and mediolateral (x-axis) directions. The single uncorrected roll rotations of 2° and 3° caused the smallest difference in the translational errors (0.1-0.9 mm). The single uncorrected yaw rotations of 2° and 3° caused the largest difference in the translational errors (0.1-2.9 mm). The changes in translational shifts in the longitudinal direction of 3.3 mm and 4.1 mm were caused by the single uncorrected yaw of 4° and 5°, respectively.

The histogram shows the difference between the 2 groups of translational errors with and without rotational corrections in the vertical, longitudinal, and lateral directions.
Impact of Rotational Errors on Dose Distribution of the Breast Target and OARs
Eight angle combinations were generated from artificial rotations for the breast phantom. A total of 9 DVH curves were, therefore, assessed for the PTV, left lung, and heart. Dosimetry comparisons on the PTV and OARs for the DVHs are shown in Figure 6.

Dose-volume histograms (DVHs) show dosimetry comparisons with or without rotations in 3 roll axes at the same time on the planning target volume (PTV) (A and B) and organs at risk (OARs) with the left lung (A) and heart (B). The rotational errors in the roll and yaw directions were the 4 paired combinations of 3° and −3°.
The original value of PTV-V50 Gy was 98.10%. When the pitch rotations were −2.5° and 2.5° and the roll and yaw were both 3°, the reductions in PTV-V50 Gy were 20.07% and 29.58% of the original value, respectively. In the pitch direction, the values of PTV-V50 Gy for a rotation error of −2.5° were greater than those for a rotation error of 2.5°, with reductions of 18.17% to 21.76% and 29.52% to 35.82% of the original value, respectively. The different orientations of roll and yaw for 3° changed the PTV-V50 Gy values by nearly 4% to 6%.
Larger hot and cold regions in the dose distribution were found in the PTV than in the original plan. When the rotation error in the pitch direction was −2.5°, the dose in the cephalic direction and the nipple area of the breast were insufficient, and larger hot regions appeared in the chest wall of the targets. Furthermore, when the rotation error of the pitch direction was +2.5°, the doses in the caudal direction of the targets were insufficient.
The original values of the left lung V5 Gy and heart Dmean were 7.27% and 132.0 Gy, respectively. When the pitch rotation was −2.5°, the left lung V5 Gy and heart Dmean were 5.70% and 57.33 Gy smaller, respectively, than those of the original plan. When the pitch rotation was +2.5°, the left lung V5 Gy and heart Dmean were 7.49% and 165.76 Gy larger, respectively, than those of the original plan.
Discussion
Setup Errors for Different Immobilization Devices
In our retrospective patient image study, the overall setup accuracy achieved by the different immobilization devices for various regions was satisfactory. Previous studies have reported no obvious correlation between the magnitudes of translational and rotational setup errors.16,17 In addition, we found that there was no clear relationship between positional reproducibility and treatment fraction in agreement with a previous report, 18 suggesting that each rotational correction is useful throughout treatment.
In the abdomen region, the errors of the stereotactic frame were larger than those of the vacuum cushion and thermoplastic mask, among which the differences in the lateral, roll, and yaw directions were significant. The possible reason is that the compression plates incorporated by the SBRT immobilization system inhibit respiration while causing deformation of the abdomen in the x-axis direction. Patients may rotate in the direction of the y-axis or z-axis owing to uncomfortable compression.
In general, pitch deviations were greater than yaw and roll deviations in pelvic tumor patients, in agreement with previous reports.19,20 A possible explanation is the increased effects of couch sag.21,22 Another possible reason is that pitch positioning using skin markers may be inaccurate for pelvic tumor patients. Moreover, a study reported that patients were uncomfortable on the prone bellyboard when they had a full bladder and tended to adjust their position to relieve pressure. 23
For the breast region, we agree with the findings of a study showing that the poorer accuracy in the prone breast bracket was due to the tendency of oncologists to select larger breasts using prone breast brackets for patients. This could make it more difficult to achieve high accuracy and reproducibility due to the more mobile treatment region in larger breasts. 22
Translational Shifts With or Without Rotational Correction
Previous research has shown that translational corrections can be optimized to compensate for rotational setup errors. The setup errors due to uncorrected rotations can be reduced with additional translational corrections. 9 In addition, one study reported that the differences in translational corrections between 6D registration and 3D registration can be large. If rotational corrections cannot be employed, then the image registration can be reexecuted to include only translational parameters. 10
In our anthropomorphic adult phantom study comparing the 2 groups of translational errors, the possible reason that the 6D registration yielded smaller translational shifts than the 3D registration for a single rotation is that a portion of the translational shifts may be compensated by rotational corrections. However, this does not seem to be absolute in the registration process for radiotherapy because of the interactions of random combinations of multidirectional rotations.
The translational errors shown by the registration system during IGRT may be caused by translations and/or rotations. If the 6D parameters are not used for registration, then rotational deviations may not be found. This suggests that if the LINAC is not equipped with a 6D couch, then registration can be carried out in 3 dimensions rather than 6 dimensions.
The single uncorrected yaw rotations of 3° and 4° caused 2.9 mm and 3.3 mm shift changes in the longitudinal direction, respectively, which may lead to a misalignment of the beam to the target, causing the radiation doses to be delivered outside the target. This means that organs are at risk of receiving unnecessary and incorrect radiation doses. According to our above data, there were no changes greater than 3° in the yaw direction, except in the breast region. However, during clinical practice, the rotational angles encompass random directions and values in 3 directions simultaneously. Therefore, the influence of the rotation corrections on the change in the translational shifts becomes more complicated.
Dosimetry Variations for the Breast Target and OARs With or Without Rotational Errors
Overview of dosimetry changes
Extensive studies have focused on the impact of translational setup errors and roll or yaw rotations on the dose distribution in breast cancer radiotherapy.12,24,25 Therefore, the rotational setup errors in 3 directions were simulated simultaneously in this study. In dosimetry comparisons of the PTV, a 5% change in the dosimetry was judged as acceptable variation. 26 In this study, the dosimetric changes were all more than 5%, which is considered unacceptable.
Reasons for dose distribution changes
The dosimetry changes caused by a positive rotation in the pitch direction were greater than those caused by a negative rotation. This may be related to the target volumes and shapes; that is, the targets in the caudal direction of the breast region are larger than those in the cephalad direction. The different directions of yaw and roll affected the PTV dose coverage. The reason may be that although the targets rotate in opposite directions, the irradiated dose volumes are asymmetrical and different. The rotational errors in the pitch direction had a great impact on the dose distribution of the breast region. A possible reason is that the changes in dose may be related to the thickness of radiation passing through human tissue.
Methods for limiting breast errors
There are some strategies for limiting errors in the breast region. First, tracking systems via optical surface-guided radiotherapy can be considered for evaluating breast position and shape in real time without an additional irradiation dose to the patients. In addition, it can also be combined with the gating technique via free-breath or breath-hold to achieve a static breast target for more accurate radiotherapy.27,28 Second, an auxiliary positioning line can be added, and the fixation device of the breast bracket can be selected in combination with a thermoplastic shell. Third, radiation physicists and technologists should pay more attention to possible rotational setup errors in the pitch direction, such as quality control of the breast bracket and couch sag. IGRT and 6D couches may be required for each treatment fraction of breast cancer patients to ensure treatment quality.
Breast deformation
In the whole process of radiotherapy for breast cancer patients, deformation (due to breast shrinkage, hardening, swelling, and other causes) is challenging and should not be ignored, and the influence of deformation errors should be avoided or reduced as much as possible. A study evaluated the effect of breast deformation on the accuracy of the setup correction in surface-guided radiotherapy systems. They found that the magnitude of deformation of the breast surface affects the positioning accuracy and that the deformation occurs more in translation than in rotation. 29 In turn, rotational setup errors may have an impact on the shape and volume of the target and OARs during the treatment of breast cancer patients. Deformation was not included in our study, while only a rigid anthropomorphic phantom was used to investigate the dosimetry effect from rotational setup errors. The reason was to specifically present the effect of setup errors rather than the mixed errors from both setup and deformation. The dosimetry effects from breast deformation will be investigated in a future study by our team.
Limitations of This Study
There are several limitations to the current study. First, to compare the magnitude of 6D setup errors, the absolute values were used for statistical analysis, and thus the directionality was ignored. Second, pitch rotations were simulated by adjusting the angles of the breast bracket, but this method does not allow the simulation of angles less than 2.5°. Third, breast deformation during radiotherapy was not considered in the calculations in this study. Fourth, there were not enough data for statistical analysis in the phantom experiments.
Conclusion
Rotational corrections may affect translational errors and improve patient setup accuracy. The rotational setup errors of breast cancer patients during radiotherapy are relatively large in magnitude and are likely to significantly affect PTV coverage and OAR doses.
Footnotes
Abbreviations
Authors’ Note
This study was approved by the Ethics Committee of Shandong Cancer Hospital and Institute (SDTHEC2022001033).
Author Contributions
Conceived and designed the study: Jian Zhu, Min Fu, and Zhen Cui. Analyzed and interpreted data for the study: Min Fu, Yanhua Cui, Wenlong Qiu, Yan Zhang, and Dandan Wang. Drafted and/or revised the manuscript: Min Fu, Jian Zhu, Shaojie Yan, Zengjing Zhao, and Yungang Wang. Approved the version to be published: Jian Zhu. Agreed to be accountable for all aspects of the work: Jian Zhu and Min Fu.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant numbers 82172072); the Shandong Provincial Natural Science Foundation (ZR2020LZL001); and the Foundation of Taishan Scholars Program of Shandong Province (Young Taishan Scholars, No. tsqn201909140).