
Abstract
Introduction
This study aimed to retrospectively evaluate and compare the accuracy, complication rate, and feasibility of computed tomography (CT)-guided introducer-assisted percutaneous lung biopsy with those of freehand percutaneous lung biopsy for the diagnosis of pulmonary nodules ≤ 2 cm.
Methods
We retrospectively analysed clinical data of 307 patients with pulmonary nodules ≤ 2 cm who underwent percutaneous lung biopsy between January 2015 and August 2024. The patients were divided into two groups: A, 153 patients undergoing freehand puncture, and B, 154 patients in whom the procedure was assisted by a guidance device. A statistical analysis was performed to assess the success rate, diagnostic accuracy, and complication rate of the two techniques and to evaluate the feasibility of using a guide device-assisted puncture biopsy for small pulmonary nodules.
Results
All 307 patients successfully completed the percutaneous biopsy procedure (100% technical success rate). Diagnostic accuracy was 95.4% and 96.8% in Groups A and B, respectively (p = .161). Groups A and B required an average of 9.04 ± 2.58 and 8.14 ± 1.72 intraoperative CT scans, respectively (p < .001). Mean procedural durations for Groups A and B were 12.77 ± 4.51 and 10.83 ± 2.51 min, respectively (p < .001). In Groups A and B, the immediate need for closed thoracic drainage was 4.6% (7/153) and 1.9% (3/154), respectively (p = .165), and incidence of haemoptysis was 10.5% (16/153) and 9.7% (15/154), respectively (p = .492). Neither group experienced complications such as air embolism or needle tract seeding metastasis.
Conclusion
Both CT-guided needle biopsy performed using a guidance device and freehand biopsy demonstrated high diagnostic accuracy for pulmonary nodules ≤ 2 cm. Procedures conducted with a guidance device contributed to shorter operation times, fewer CT scans, and lower radiation exposure.
Introduction
The detection rate of early-stage lung cancer presenting as small pulmonary nodules has markedly increased with advancements in computed tomography (CT) technology. 1 In a trial utilising low-dose CT for lung cancer screening, 98% of positive findings and 86% of detected lung cancers were characterised by small (≤ 20 mm) pulmonary nodules.1,2
Determining whether pulmonary nodules are benign or malignant remains a challenge for clinicians. Although percutaneous lung biopsies are widely recognised as safe and reliable diagnostic procedures, numerous studies have reported that the diagnostic accuracy of freehand CT-guided percutaneous transthoracic needle biopsy for small pulmonary nodules (≤ 20 mm) ranging from 75% to 90%.3–6
Although the varying outcomes may partially stem from considerable differences in nodule characteristics across studies, these discrepancies can also be attributed to the high dependence of freehand biopsy based on the operator's expertise. This procedure requires that physicians possess extensive experience and strong spatial perception skills, as they rely on tactile sensation and clinical experience to control critical factors such as puncture force and angle. Physicians with limited experience may require additional time and repeated procedures for accumulating necessary proficiency.7,8
CT-guided puncture biopsy, 9 when assisted by a guidance device, can accurately control the needle angle and direction. In conjunction with CT imaging, this method enhances precision, reduces procedural duration, improves technique standardisation, and a shortens learning curve.9–11
In this study, we conducted a comparative analysis on 307 patients with ≤ 2 cm pulmonary nodules who underwent either freehand or guide device-assisted lung puncture to evaluate the application value of the guide device. In this study, we aimed to compare the accuracy, complication rate, surgical success rate, operative time, and number of CT scans between the methods.
Materials and Methods
Patients
A total of 307 patients with pulmonary nodules measuring ≤ 2 cm underwent percutaneous lung biopsy between January 2015 and August 2024 in our department. The cohort comprised 166 male and 141 female patients, with a mean age of 61 (range, 19-87) years. The pulmonary nodules comprised 81 and 226 lesions ranging from 1 to 10 mm and 11 to 20 mm, respectively. The patients were stratified into two groups: Group A, comprising 153 patients who underwent freehand puncture, and Group B, comprising 154 patients in whom the procedure was assisted by a guidance device. The study was approved by the local institutional review board (No. 2018-Ethics Review-08).
Inclusion Criteria
(1) Pulmonary nodules with a diameter of ≤ 20 mm as measured on CT lung window images, which exhibited clinical and radiological features suggestive of malignancy; (2) nodules in patients with a history of malignant tumours who are in prolonged remission or have multiple primary malignancies; (3) persistent pulmonary nodules; (4) platelet count > 50,000/μL and international normalised ratio (INR) of prothrombin time < 1.5; and (5) cases underwent multidisciplinary team review and patients provided informed consent for surgical intervention.
Exclusion Criteria
(1) Irreversible coagulation disorders; (2) severe chronic obstructive pulmonary disease, emphysema, or pulmonary fibrosis precluding surgical intervention; (3) severe cardiopulmonary insufficiency; (4) significant pulmonary hypertension; and (5) acute psychiatric episodes.
Before the procedure, comprehensive auxiliary examinations, including complete blood count, coagulation function test, liver and kidney function analyses, and electrocardiography, were conducted. Patients were required to fast for 4–6 h before surgery. During the procedure, continuous monitoring of vital signs, such as the heart rate, blood pressure, and blood oxygen saturation, was ensured. An intravenous line was established preoperatively, and patients were administered oral cough suppressants and sedatives. Preoperative respiratory training was provided to the patients. All procedures were performed by operators with >10 years of experience in lung biopsy diagnosis and treatment.
In the manual puncture group, the patients were positioned according to the nodule locations identified on preoperative enhanced chest CT scans for achieving optimal puncture pathways. Routine CT scans with a 3-mm slice thickness were conducted, and thin-layer reconstructions (1.0 mm) were performed in the regions of interest. Puncture entry points and paths were determined, marked on the skin, disinfected, and prepared. Local anaesthesia was administered using 6–10 mL 1% lidocaine. A 17-G coaxial trocar needle (Argon Medical Devices, USA) was inserted in a stepwise manner along a predetermined path until the parietal pleura was reached. Subsequent CT confirmed that the needle tip was accurately positioned at the proximal end of the lesion. The needle core was then removed, and an 18-G semi-automatic biopsy gun (Argon Medical Devices, USA) was used to obtain 2–3 pathological tissue samples. Following sample collection, the coaxial trocar needle was withdrawn, and a full lung scan was performed at the end of the procedure. Postoperatively, the patients were monitored for 24–48 h to promptly identify and manage any complications (Figure 1).
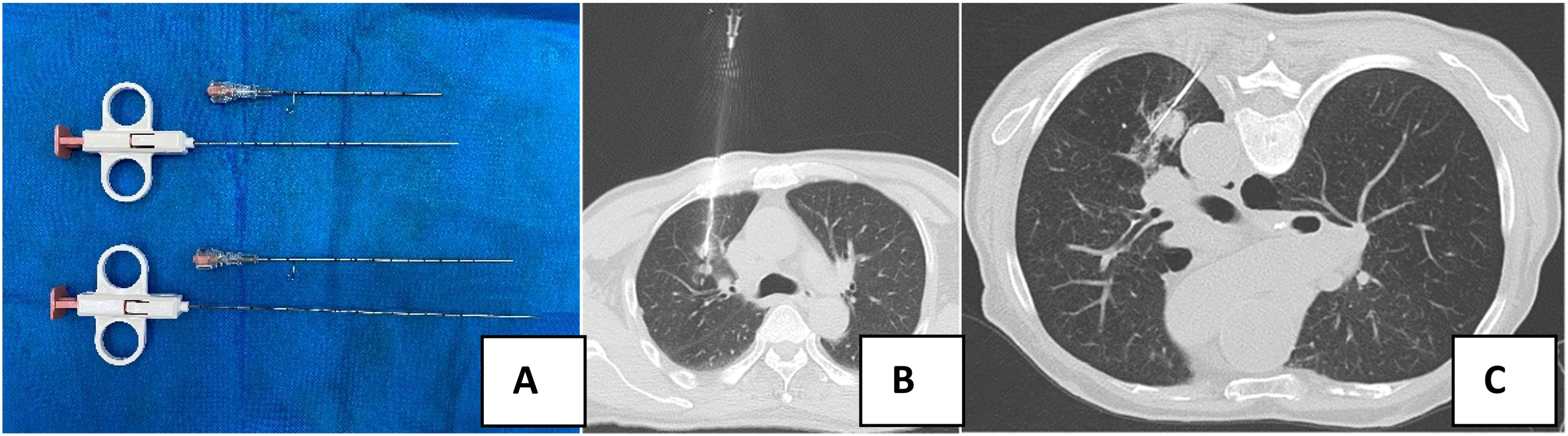
Biopsy puncture instruments and procedures (A) instruments used: 17-G coaxial trocar and 18-G biopsy needle, (B) solid nodule in the anterior segment of the right upper lobe (0.8 × 0.9 × 1.0 cm) and the corresponding biopsy procedure, and (C) Solid nodule in the posterior segment of the left lower lobe (1.8 × 1.7 × 1.8 cm) and the corresponding biopsy procedure.
For the guided puncture group, we used the same 17-G coaxial puncture needle and 18-G semi-automatic biopsy gun as the manual puncture group. After CT scanning, the puncture entry point, angle, and depth were determined and marked on the patient's skin surface. A disposable guide (Nanon-I, China) was attached to the matching adjustable metal rod, and the guide level was calibrated to zero. The guide was adjusted based on the puncture angle measured from the CT scan images. The puncture needle was then advanced to the skin surface along the guided trajectory. CT was performed to observe the puncture angle, with fine adjustments made as needed. Subsequently, a 17-G cannula was gradually advanced along the predetermined trajectory until it reached the proximal end of the nodule, ensuring accurate positioning at the proximal end of the nodule. Two to three cutting biopsies were obtained using the 18-G biopsy gun. The procedure was concluded after acquiring satisfactory samples, followed by a complete lung scan for monitoring immediate complications (Figure 2).

Guide-assisted biopsy procedure (A) the disposable guide is connected to the fixed frame, which possesses both rigidity and flexibility. The guide can be fixed near the puncture point by adjusting the metal rod. (B) Solid nodule in the lower lobe of the right lung (1.9 × 1.4 × 1.5 cm). A 17-G coaxial biopsy needle is advanced into the subcutaneous tissue under the guidance of a guide device. and (C) Needle placement and biopsy: the guide angle is adjusted as needed, positioning the coaxial trocar at the proximal end of the lesion. An 18-G biopsy needle is then used to complete the cutting biopsy.
Statistical Analysis
Data processing was performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). Continuous variables were assessed for normality; they are presented as mean ± standard deviation. Categorical variables are reported as frequency and percentage. Continuous variables were compared between the groups using independent t-tests, whereas chi-square tests were used for categorical variables. Statistical significance was set at p < .05.
Results
Clinical Data
A total of 307 pulmonary nodules from patients meeting the inclusion criteria were analysed, with nodule dimensions ranging from 0.5 to 2.0 cm in diameter. In Group A (freehand technique), 153 patients had a total of 153 pulmonary nodules, with a mean age of 62.54 ± 10.53 years. This group comprised 42 and 111 cases with 1–10- and 11–20-mm nodules, respectively. In Group B (assisted by a guidance device), 154 patients had a total of 154 pulmonary nodules, with a mean age of 59.84 ± 11.23 years. This group comprised 39 cases with 1–10-mm nodules and 115 cases with 11–20-mm nodules. Given the statistically significant differences in the nature of the nodules and age between the two groups, we conducted a multivariate logistic regression analysis to adjust for the potential impact of baseline imbalance on the primary outcome measures (especially diagnostic accuracy). We included the grouping variable (freehand vs guided device) as the main independent variable and incorporated baseline variables with statistically significant differences as covariates in the model, primarily the nature of the nodules and patient age. Multivariate logistic regression analysis revealed that no independent significant correlation was found between the biopsy technique (guided device vs freehand) and diagnostic accuracy (95% confidence interval [CI]: 0.17-1.96, p = .387) after adjusting for the effects of the nature of the nodules and age (Table 1).
Baseline Clinical Characteristics of the two Patient Groups.

SD: standard deviation, pGGO: pure ground-glass opacity, mGGO: mixed ground-glass opacity.
Surgical Procedures, Imaging Parameters, and Quantities of Biopsy Samples
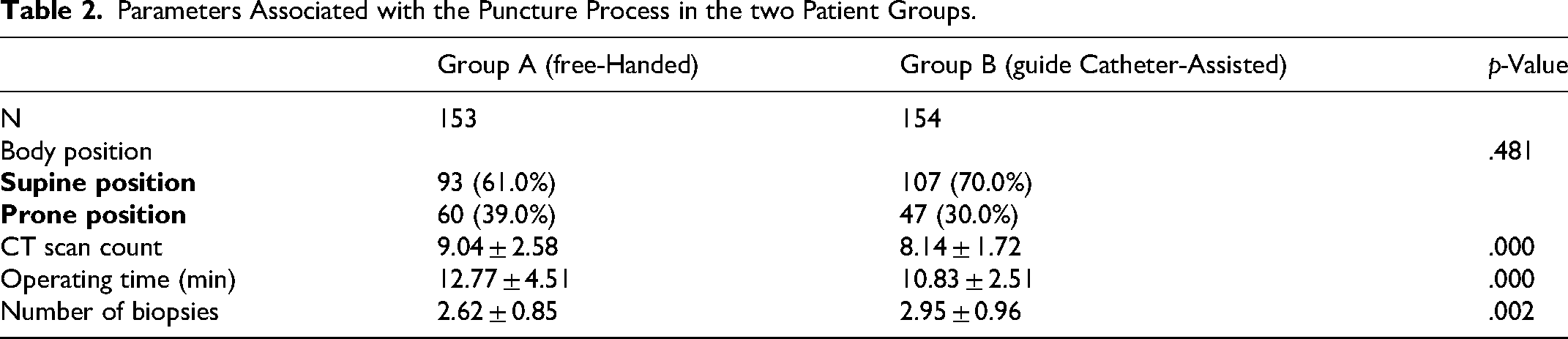
All patients were placed in either supine or prone position. In Group A, 93 patients (61%) were placed in the supine position and 60 patients (39%) in the prone position; in Group B, 107 patients (70%) were positioned supine and 47 patients (30%) were positioned prone (p = .481). The mean number of CT scans was 9.04 ± 2.58 in Group A, compared with 8.14 ± 1.72 in Group B (p < .001). The operation time in Group A averaged 12.77 ± 4.51 min, whereas that in Group B was 10.83 ± 2.51 min (p < .001). The mean number of biopsies performed in Group A was 2.62 ± 0.85, whereas that in Group B was 2.95 ± 0.96 (p = .002; Table 2).
Parameters Associated with the Puncture Process in the two Patient Groups.
Pathology Results
The diagnosis of the target nodule was evaluated using the following three approaches. (1) If the patient subsequently underwent surgical resection, a definitive diagnosis was established based on the pathological report. (2) A definitive diagnosis was considered if biopsy confirmed malignancy or specific benign conditions, such as hamartoma, pulmonary tuberculosis, and cryptococcosis. (3) For non-specific benign pathologies (negative for malignancy and chronic inflammation), follow-up CT scans could help determine whether the lesion is truly benign or pseudo-benign. A reduction in the lesion diameter by ≥20% indicate a final diagnosis of a benign condition.12,13 In this study, 50 patients in Group A subsequently received surgical treatment, accounting for 32.6% of the group. The concordance between postoperative pathology and preoperative puncture was 98%. A total of 55 patients received microwave ablation treatment. In Group B, 56 patients subsequently received surgical treatment, accounting for 36.3% of the group. The consistency between postoperative pathology and preoperative puncture was 98.2%. A total of 49 patients received microwave ablation treatment. Other treatments included radiotherapy, follow-up observation, anti-infection treatment, and chemotherapy.
Among the 307 nodules, 215 were pathologically confirmed as malignant. In Group A, 110 cases were diagnosed as malignant, comprising 18, 14, 58, 9, 1, 10, and 43 cases of adenocarcinoma in situ (AIS), minimally invasive adenocarcinoma (MIA), invasive adenocarcinoma (IA), primary lung squamous cell carcinoma, small cell lung cancer, metastatic lung cancer, and other conditions (including inflammation, tuberculosis, fungal infection, and non-neoplastic lung tissue), respectively. In Group B, 105 cases were diagnosed as malignant, including 24, 8, 43, 18, 10, 2, and 49 cases of AIS, MIA, IA, primary lung squamous cell carcinoma, metastatic lung cancer, small cell lung cancer, and other conditions, respectively. Based on the pathological results, the diagnostic accuracy for Group A was 95.4%, whereas that for Group B was 96.8%. No significant difference was observed between the groups (p = .160; Table 3).
Pathological Findings from Biopsies of the two Patient Groups.
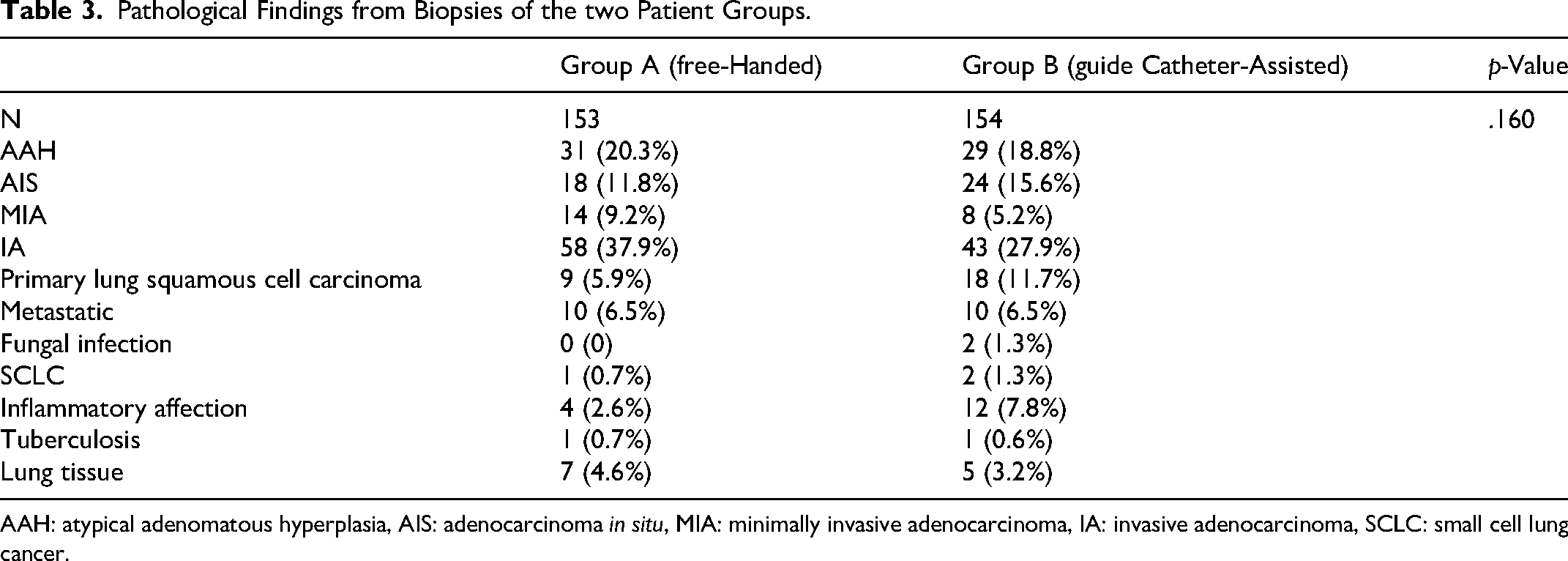
AAH: atypical adenomatous hyperplasia, AIS: adenocarcinoma in situ, MIA: minimally invasive adenocarcinoma, IA: invasive adenocarcinoma, SCLC: small cell lung cancer.
Technical Success Rates and Associated Complications
All patients who underwent biopsy at this centre were admitted for a 24-h observation period to monitor potential complications. A 100% technical success rate in completing the biopsy procedure was achieved in both groups. The primary complications included pneumothorax, bleeding along the biopsy needle tract, minor haemoptysis, and subcutaneous emphysema. Specifically, the incidence of pneumothorax requiring thoracic drainage was 6.5% (10/153) in Group A and 4.5% (7/154) in Group B (p = .307). Patients with mild pneumothorax were conservatively managed without drainage. The incidence of haemoptysis was 10.5% (16/153) in Group A and 9.7% (15/154) in Group B (p = .492). All cases of haemoptysis in both groups were classified as minor (≤ 10 mL). The incidence of bleeding along the biopsy needle tract was 29.4% (45/153) in Group A and 30.5% (47/154) in Group B (p = .465). Subcutaneous emphysema occurred in 3.3% (5/153) of patients in Group A and 3.9% (6/154) in Group B (p = .504). Notably, there were no instances of air embolism or needle tract-seeding metastasis in either group (Table 4).
Incidence of Postoperative Complications in the two Patient Groups.

Discussion
For pulmonary nodules measuring less than 2 cm, a biopsy is essential for achieving a definitive diagnosis.14,15 In terms of diagnostic accuracy, biopsy provides precise pathological confirmation, differentiating between benign conditions (inflammatory nodules or hamartomas) and malignant lesions (lung cancer). This distinction is critical for formulating subsequent treatment strategies. Biopsy can prevent unnecessary surgical interventions and excessive treatments for benign nodules, whereas for malignant nodules, it enables clinicians to determine the specific pathological subtype, thereby facilitating the selection of appropriate therapeutic approaches, such as surgery, chemotherapy, targeted therapy, and immunotherapy.14,16
CT-guided lung nodule puncture-assisted techniques encompass electromagnetic navigation and 3D printing template-assisted puncture technology. These methods effectively reduce the frequency of CT scans, consequently lowering the radiation exposure of patients.17,18 However, these methods impose stringent requirements on operators and involve complex and time-consuming preparation and operational procedures. This study introduced a disposable guide as an alternative approach for achieving comparable reductions in the CT scan frequency and patient radiation exposure. Moreover, this method is characterised by its simplicity and ease of use, making it particularly beneficial for less experienced physicians performing manual punctures. This shortens the learning curve and enhances the precision of the puncture and biopsy procedures. 19 Although technologies, such as electromagnetic navigation, laser guidance, or three-dimensionally printed templates, are highly accurate, they possess significant barriers to implementation. They are characterised by high costs, complex operational procedures, and time-consuming preparation processes. These systems have a steep learning curve for operators and are typically only available in large medical centres equipped with specialised hardware and technical support. In contrast, the ‘one-time guide plate’ that we used is a purely mechanical device. Its single-use cost is much lower than the amortised cost of technology-intensive systems. It can be used immediately after simple calibration upon opening, with almost no additional preparation time. For less experienced physicians, it provides precise angle control through physical constraints, transforming the ‘freehand’ operation that relies on the surgeon's spatial imagination and sense of touch into a more standardised and repeatable process without the need for learning complex software interfaces.
This study demonstrated that the number of CT scans required for puncture biopsy using a guidance device was significantly lower (8.14 ± 1.72) than that with freehand puncture (9.04 ± 2.58, p = .000). Additionally, the operation time was 10.83 ± 2.51 min for the guidance device group, compared with 12.77 ± 4.51 min for the freehand group (p = .000), indicating that the use of a guidance device enhances procedural precision, thereby reducing both operation time and patient radiation exposure. Regarding biopsy accuracy, no significant difference was observed between the guidance device group (96.8%) and freehand group (95.4%; p = .161), which aligns with the findings of previous studies on CBCT-guided puncture.4,20 All surgeons involved in this study had more than 10 years of experience in lung nodule puncture, and no significant difference in the diagnostic accuracy was observed between the groups. However, for less experienced surgeons or beginners, a guidance device can be recommended owing to its ability to precisely control the angle and depth of the coaxial needle in the craniocaudal and anteroposterior directions. The operation can be conducted in a standardised manner, facilitating both learning and clinical practice, provided that patients are adequately trained in breathing control during the procedure.21,22
Regarding the complications associated with percutaneous needle biopsy (PCNB), previous studies have reported an incidence of pneumothorax ranging from 25% to 40% and haemoptysis occurring in 5%–10% of cases.23,24 However, in our study, the incidence of patients requiring thoracic puncture and catheterisation was 4.5% in the guide device-assisted group and 6.5% in the manual group. The incidence of haemoptysis was 9.7% and 10.5%, respectively, whereas the incidence of biopsy needle tract bleeding was 30.5% and 29.4%, respectively, in the guide device-assisted group and manual group. Notably, the incidence of pneumothorax requiring closed drainage was approximately 5% in both groups, with all instances of haemoptysis being minor, and no cases of massive haemoptysis observed. These findings are consistent with those previously reported. 23 The overall complication rate in this study was relatively low, particularly for pneumothorax and haemoptysis. This may be attributed to the enhanced safety and precision of the puncture route and needle insertion angle provided by the guidance device during PCNB. Additionally, the coaxial needle technique plays a crucial role in minimising complications by preventing repeated pleural punctures and reducing the risk of pneumothorax.
Our study had certain limitations. This retrospective study may not have fully captured the advantages of the two techniques. Further prospective studies are warranted to comprehensively compare the strengths and weaknesses of these methods. Furthermore, while the surgeons performing the procedures in both groups had over a decade of experience in lung puncture, it is important to note that for less experienced practitioners, freehand puncture might not yield high biopsy accuracy or low complication rates. However, this observation necessitates further rigorous prospective validation studies. Additionally, some patients in this study had follow-up periods shorter than 2 years, which could potentially affect the accuracy of the biopsy results.
In conclusion, both CT-guided needle biopsy utilising a guidance device and freehand biopsy demonstrated high diagnostic accuracy for pulmonary nodules ≤ 2 cm, with minimal complication rates. The procedure employing a guidance device requires less operative time and fewer CT scans and consequently exposes patients to reduced radiation levels.
Footnotes
Abbreviations
Ethical Considerations
The study adhered to the principles outlined in the Declaration of Helsinki (2013 revision) and was approved by the local institutional review board (No. 2018-Ethics Review-08).
Consent to Participate
The requirement for individual patient consent was waived owing to the retrospective nature of the study.
Consent for Publication
Not applicable.
Author Contributions
Kaixian Zhang conceived and designed the study. Miaomiao Hu conducted the experiments, collected the data, and drafted the manuscript. Peishun Li and Chao Xing and Wanying Yang contributed to data interpretation. Sen Yang and Baohu Wang and Minghui Lv assisted with the investigation and formal analysis of data. Kaixian Zhang approved the final version of the manuscript. Xusheng Zhang and Qianqian Yuan verified all raw data for authenticity. All authors have read and approved the final manuscript.
Funding
This study was funded by Zaozhuang Science and Technology Development Program Project (project number: 2025NS59) and the Shandong Provincial Medical and Health Science and Technology Development Program (Grant No. 2017WS591).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article :Analysis of the Accuracy and Complications of Computed Tomography-Guided Steerable Needle Assisted Lung Biopsy (≤2 cm) versus Freehand Biopsy for the Diagnosis of Pulmonary Nodules.