
Abstract
Introduction
Low-dose CT (low-dose computed tomography, LDCT) has unique advantages for the detection of small pulmonary nodules; 1 therefore, the detection rate of pulmonary nodules has increased and is reported to be 8% to 51%2,3 according to related studies. The Fleischner Society defines pulmonary nodules as dense, spherical or irregular, and clear or unclear lesions with a diameter of ≤3 cm scanned by low-dose CT. 3 CT-guided percutaneous core needle biopsy (CNB) can directly obtain lesion tissue, which is an important mean for the diagnosis of pulmonary nodules. 4 However, the small pulmonary nodules are small in size and shift with respiratory movement; thus, traditional CT-guided percutaneous CNB lacks certain advantages. Huang et al 5 and Kothary et al 6 reported that the biopsy results of small lesions were less accurate than those of large lesions, and studies reported a diagnostic accuracy of 87% during CNBs of nodules smaller than 20 mm. 7
Therefore, the yield of traditional CT-guided percutaneous CNB for small lung nodules is also worth studying. Recently, the use of a 3D-printed navigational template for the localization of small peripheral lung nodules showed good efficacy and safety. 8
However, there are few reports on 3D-PCT-assisted CT-guided percutaneous CNBs of pulmonary nodules. Although Ji et al 9 summarized the process and technical characteristics of 3D-PCT-assisted CT-guided percutaneous CNBs, there was no control group, and no comparative study was performed to assess the diagnostic yield, pathological examination results, and complications. To further explore the efficacy and safety of 3D-PCT-assisted CT-guided percutaneous CNB of pulmonary nodules, we conducted comparative clinical research. All patients in the 3D-PCT group and the Control group were reviewed and analyzed. We comprehensively evaluated the utility of 3D-PCT in percutaneous CNB of pulmonary nodules based on the diagnostic yield of CNB; the incidence of complications, such as pneumothorax, pulmonary hemorrhage.
Patients and Methods
Patients
This retrospective, single center study was approved by the Taihe Hospital (Shiyan, Hubei, China) Ethics Committees (2018KS027) in January 2018 and was performed in accordance with the principles of Good Clinical Practice following the Tri-Council guidelines. All patients or their substitute decision makers provided written informed consent prior to patients. Between January 2018 and January 2021, 372 patients were included in the study due to solitary or multiple pulmonary nodules. Inclusion criteria: ①Isolated nodules or multiple nodules that need a clear nature; ②Bronchoscopy, sputum or bronchoalveolar lavage fluid cytological examination, sputum culture cannot clearly diagnose the disease; ③Suspected of malignant ground glass nodules; ④Known malignant nodules but need to clarify histological type or molecular pathological type (re-biopsy); ⑤Lung nodules are < or =30 mm in size (follow-up and regular re-examination for lesions smaller than 8 mm). Exclusion criteria: ①Severe cardiopulmonary insufficiency (such as severe pulmonary hypertension); ②Uncorrectable coagulation dysfunction; ③Anatomically or functionally isolated lung; ④There are obvious infectious lesions on the puncture path; ⑤Bullae, chronic obstructive pulmonary disease, emphysema, pulmonary fibrosis; and ⑥Mechanically ventilated patients; ⑦Patients who lost follow-up. Flow diagram of the included patients was shown in Figure 1. Finally, 210 of the 372 patients who underwent CT-guided percutaneous CNB provided written informed consent before the procedure. Patient demographics and nodule characteristics, including the proportions of ground-glass opacity (GGOs) and solid nodules, lesion size, pleura-to-lesion distance, target location, and number of specimens obtained, of the two groups were recorded and analyzed. Patient characteristics and lesion parameters are detailed in Table 1.
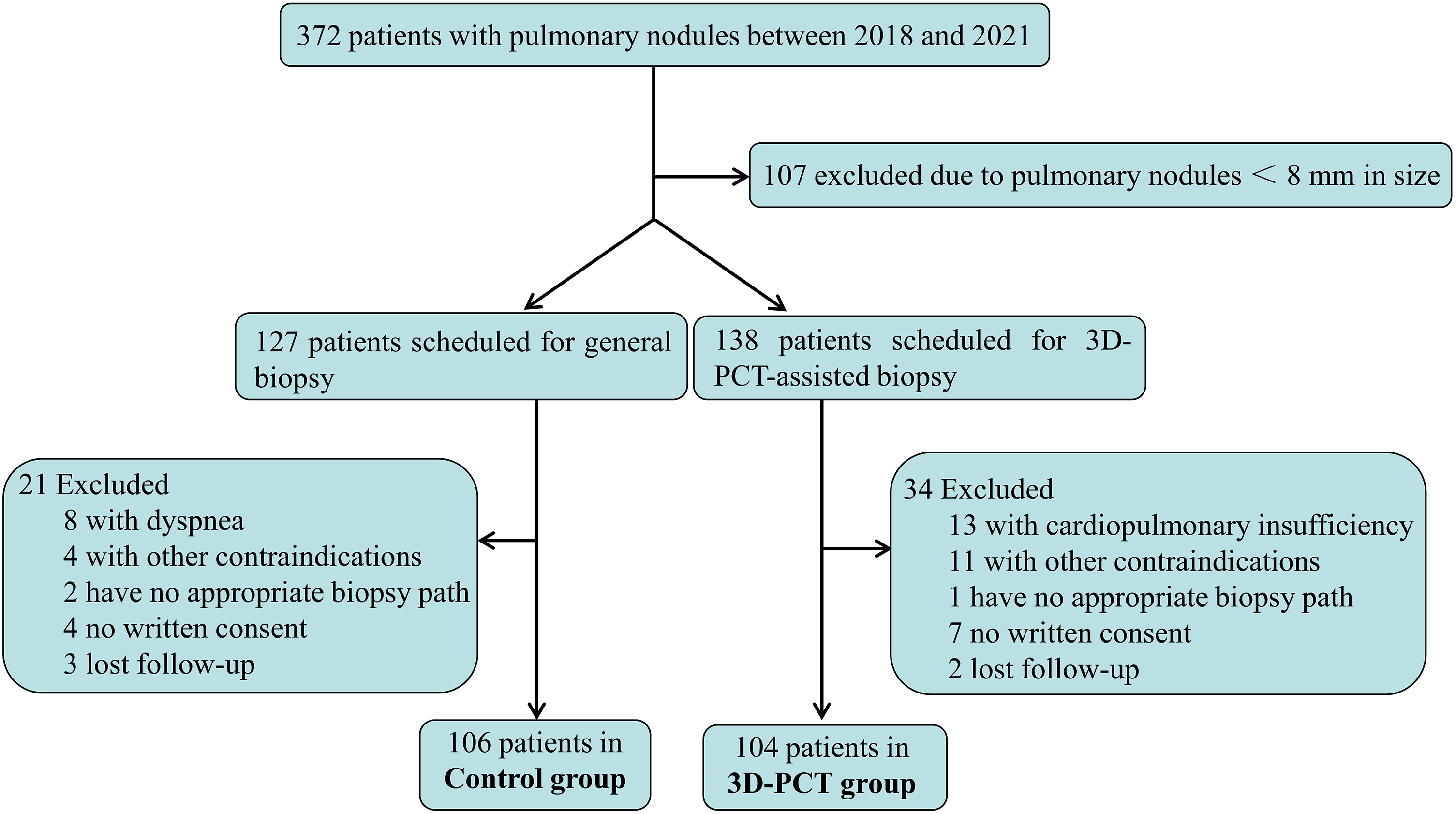
Flow diagram of the patients’ selection.
Patient Characteristics and Lesion Parameters.

arepresents the t value of Independent-Samples t Test; brepresents χ2 value of Chi-square test.
GGO indicates ground-glass opacity.
Equipment
Sixteen multislice spiral computed tomography (Philips Co. Ltd) disposable 17-gauge coaxial biopsy needles (C1816B, BARD Medical Devices Inc, USA) were used, which allowed multiple biopsies once the lesion was targeted. A disposable 18-gauge core biopsy needle (MN1816, BARD Medical Devices Inc, USA) was used to collect samples. The 3D-printed coplanar puncture template, three-axis coordinate navigation frame, angle-measuring instrument (Tangshan Tongrenhe Technology Co. Ltd), and negative pressure position fixing pad (Philips Co. Ltd) were used in the process (Figure S1). The following items were also used: a disposable 17-gauge coaxial introducer needle (MCXS1820BP, Argon Medical Devices, Inc., USA); BioPinceTM full core biopsy instrument (360-2080-01, Argon Medical Devices, Inc., USA).
Patient Position and Fixation
Patients were admitted to the interventional radiology department on the same day of the procedure, the procedure strictly follows the BTS guidelines. 10 According to the patient's recent imaging data, the approximate puncture path was determined, and the appropriate patient position was selected based on facilitating access to the target lesion and avoiding target lesion motion. In addition, the patient was kept in a comfortable and relaxed position. For patients in the 3D-PCT group, a negative pressure vacuum bag was used to fix their positions.
Location of Puncture Point
For patients in both groups, the prepuncture point was scanned first, and images of 3-mm slice thickness with a standard lung window were acquired during the entire procedure such that the nodules could be clearly displayed. Generally, the maximum cross-section of the nodule under the CT scan is designed for the puncture path, and the needle path from the pleura to the target lesion was also chosen to be as short as possible. The most appropriate needle insertion point is selected according to the cross point formed by the imaging point of the positioning metal grid on the patient's body surface under the CT image and the positioning laser line. The selected intersection point, that is, the prepuncture needle point, is marked, and the puncture angle and depth is recorded based on the CT image.
Installation of Navigation System and 3D-PCT
The three-axis coordinate navigation frame was installed on the same side of the lesion and connected with the angle-measuring instrument. Then, the coplanar puncture template was connected to the navigation frame, and the template was adjusted in all directions (X-, Y- and Z-axes) (Figure S2) to match the intersection line and laser positioning line on the patient's body surface (Figure S3). Finally, the template angle is adjusted to meet our demands. The above operation was only performed for patients in the 3D-PCT group, and the detailed video has been uploaded as a Supplemental material. 9
Computed Tomography-Guided CNB Procedure
After sterile preparation for all patients, 2% lidocaine was used for local anesthesia. In the 3D-PCT group, procedure flowchart is shown in Figure 2A. The biopsy needle path was accurately designed based on the CT scan layer and template coordination. A coaxial needle was inserted into the upper edge of the lesion (approximately 0.5 cm away from the lesion) through the selected template holes. A CT scan was performed again to confirm that the position was accurate, and then the biopsy was performed with a biopsy instrument. If the biopsy specimen was not satisfactory, the biopsy direction was adjusted appropriately, and another biopsy was obtained. For patients in the control group, biopsies were performed using the routine method, as shown in Figure 2B. A 17-gauge coaxial introducer needle (C1816B, BARD Medical Devices Inc, USA) was introduced to the upper edge of the lesion (approximately 0.5 cm away from the lesion) from the predesigned needle path and puncture point. Then, a CT scan was performed to confirm that the position, depth and angle of the coaxial introducer needle were completely consistent with the predesigned needle. If there was a deviation of angle or length, the needle was adjusted in real time. An 18-gauge core biopsy instrument (MN1816, BARD Medical Devices Inc., USA) was introduced through the central canal of the coaxial biopsy needle. The CT image of the two groups of patients before, during and after needle insertion and post-biopsy is shown in Figure 3.

Flow chart of biopsy procedure. A, 3D-PCT group; B, Control group.
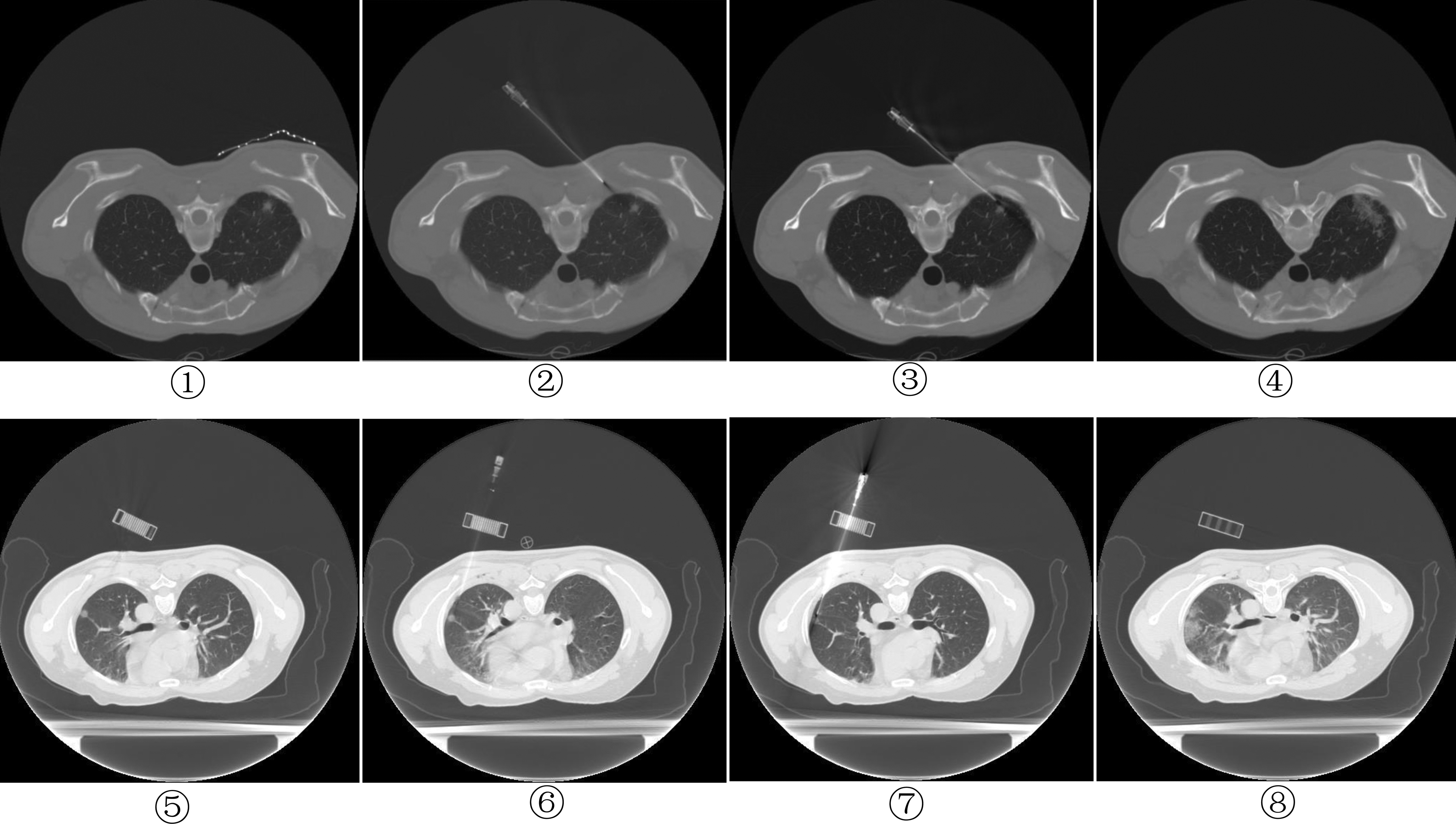
The CT image of the patients before, during and after needle insertion, and post-biopsy. ①②③④, Control group; ⑤⑥⑦⑧, 3D-PCT group.
All tissue samples obtained by CNBs were fixed with 10% formalin and embedded in paraffin for routine histopathological examination. The patient's electrocardiogram, vital signs, and blood oxygen saturation were monitored throughout the operation. After the operation was completed, a CT scan was used to observe any complications, such as pneumothorax and pulmonary hemorrhage. If the patient felt discomfort or blood oxygen levels dropped, which occurred during a major pneumothorax, a chest tube was inserted into the pleural cavity if necessary. Then, the patient was transferred to the recovery room, where oxygen (100%) was administered by nasal cannula at a rate of 3 L/min. The number of CT scans, the number of needle adjustments, frequency of biopsy, and complications of each patient were recorded. All patients were monitored closely for 4 h after the biopsy procedure.
Histopathological Diagnosis
Whether the needle biopsy is successful depends on the pathological examination or microbiology report. The needle biopsy specimens were double-blindly diagnosed by two experienced chest pathologists in the pathology department. Histopathological findings were reported as malignant tumors, sarcomas, atypical hyperplasia, tuberculosis, fungal, organizing pneumonia or nonspecific inflammation. Nonspecific inflammation cases showed no significant changes in the nodules during follow-up, indicating that the needle biopsy was successful. The pathological diagnosis report indicates that specimens with insufficient tissue or cells are considered nondiagnostic cases, and cases that are suspicious or inconclusive and cannot be clearly diagnosed are also regarded as nondiagnostic cases. Thus, negative biopsy specimens indicated that the needle biopsy failed.
Statistical Analysis
SPSS software version 17.0 was used for statistical analysis. Measurement data are expressed as the mean ± standard deviation (mean ± SD), and a t test was used. The chi-square test or Fisher's exact test was used to compare categorical data. Probability values < 5% (P < .05) were considered statistically significant. In the present study, The diagnostic yield of 3D-PCT was 95.2%, while Control was 87.7%, the sample size was estimated based on the test of variability of the independent sample rates of the two groups, where the test level α = .05, the test efficacy β = .2, the sample size ratio of 3D-PCT group and control group was 1:1, disregarding the lost visit rate, and the pearson algorithm was applied. The final calculation yields that the sample size of the two groups should be 149 respectively. In fact, as shown in Figure 1 (Flow chart of patient selection), 138 scheduled in the 3D-PCT group and 127 in the control group, when lost follow-up and others were excluded, ended up with 104 in the 3D-PCT group and 106 in the control group.
Results
A total of 104 patients were included in the 3D-PCT group, including 55 males and 49 females with a median age of 58.7 years (range, 26-77 years). In total, 106 patients were included in the control group, including 54 males and 52 females with a median age of 58.7 years (range, 13-84 years). No significant differences in age and sex were observed between 3D-PCT and control groups. The pulmonary nodules size in the 3D-PCT group and the control group was 2.0 ± 0.53 cm and 2.1 ± 0.51 cm, respectively, and no significant difference in pulmonary nodule size was noted. In the control group, there were 41 cases of lung nodules < 2 cm, accounting for 38.7%, and 65 cases of lung nodules of >or =2 cm, accounting for 61.3%; in the 3D-PCT group, there were 54 cases of lung nodules < 2 cm, with a proportion of 51.9%, and 50 cases of lung nodules of >or =2 cm, with a proportion of 48.1%. In present study, the pleura-to-lesion distance is classified into three groups: 0 to 30 mm, 30 to 60 mm and >60 mm. The number of patients with a pleura-to-lesion distance of 0 to 30 mm in the 3D-PCT group and control group is 32 (30.8%) and 33(31.1%), respectively. The number of patients with a distance of 30 to 60 mm is 53 (50.9%) and 61(57.6%), respectively, and those with >60 mm is 19(18.3%) and 12(11.3%), respectively. No significant difference was observed in the pleura-to-lesion distance between the two groups, as shown in Table 1. In the 3D-PCT group and control group, there were 22 (21.2%) and 25 (23.6%) cases of patients with pulmonary nodules in the superior lobe of left lung, respectively; 9 (8.7%) and 5 (4.7%) cases in the inferior lobe of left lung, respectively; 32 (30.8%) and 36 (34.0%) cases in the superior lobe of right lung, respectively; 14 (13.5%) and 14 (13.2%) cases in the middle lobe of right lung, respectively; and 27 (25.8%)and 26(24.5%) cases in the inferior lobe of right lung, respectively. No significant differences in nodule locations were noted between the two groups (Table 1). Nodular solid components characterized as solid, pure GGO, partly solid GGO in present study. In the 3D-PCT group, solid, pure GGO, partly solid GGO accounted for 58.7% (61/104), 25.0% (26/104), 16.3% (17/104), respectively; the control group accounted for 55.7% (59/106), 20.8% (22/106), 23.5% (25/106), no statistical difference was observed between the two groups on nodular solid components (P > .05), as detailed in Table 1. The average number of specimens obtained for each patient in the 3D-PCT group and the control group was 3.0 ± 0.87 (range, 1-4) and 3.1 ± 0.78 (range, 1-4), respectively, and no significant differences were observed.
As shown in Table 2, the incidence of pneumothorax and hemorrhage in the 3D-PCT group was 17.3% (18/104), 7.7% (8/104) respectively, which was slightly lower than that in the control group 18.9% (20/106), 9.4% (10/106) (P > .05) respectively, no significant difference was noted. Hemoptysis occurred in 1.9% (2/104) of patients in the 3D-PCT group and 1.8% (1/106) of patients in the control group, and no significant differences were observed.
Comparison of Complications, Number of Needle Adjustments, Diagnostic Yield and Time Calculation Between 3D-PCT and Control Group During Biopsy Procedure.

arepresents the t value of Independent-Samples t Test; brepresents χ2 value of Chi-square test. ★ represents the diagnostic yield of lesion size < 2 cm; ⋆ represents the diagnostic yield of lesion size >or =2 cm.
Needle adjustments in the 3D-PCT group were significantly lower than those in the control group. During the puncture procedure, the average number of needle adjustments was 1.41 ± 0.63 times (range, 1-3) in the 3D-PCT group and 2.23 ± 0.85 times in the control group (range, 1-4). The average surgical time of the 3D-PCT group was 61.36 ± 9.96 min (range, 48-110 min), which was significantly longer than that of the control group with an average time of 36.48 ± 6.55 min (range, 22-63 min).
The histopathological/microbiological findings of 210 biopsied patients are detailed in Table 3. In total, 54 (51.9%) malignant and 45 (43.3%) benign cases were noted in the 3D-PCT group; 61 (57.5%) malignant and 32 (30.2%) benign cases were noted in Control group, with an overall diagnostic yield of 95.2% (99/104) and 87.7% (93/106) in 3D-PCT group and Control group respectively. Statistical analysis revealed significant difference in diagnostic yield between the two groups, as detailed in Table 2. The diagnostic yield of CT-guided percutaneous CNB for lung nodules < 2 cm in the 3D-PCT group and the control group was 94.4% (51/54) and 80.5% (33/41), respectively, a significant difference was observed (P < .05); The diagnostic yield of CT-guided percutaneous CNB for lung nodules >or =2 cm were 96% (51/54) and 92.3% (33/41), respectively, statistical analysis revealed no significant difference (P > .05). The number of patients in the two groups that were finally diagnosed as malignant was 121, of which solid nodules, partially solid GGO, and pure GGO accounted for 84, 22, and 15 cases respectively. The remaining 89 cases are benign, of which solid nodules, partially solid GGO, and pure GGO accounted for 44, 12, and 33 cases respectively, as shown in Table 4.
Histopathology/Microbiology Findings of 210 Biopsied Lesions.

Abbreviation: AAH, Atypical adenomatous hyperplasia
aLymphomas, b1Lymphoma and 1 small cell lung carcinoma. cPatients has been followed-up for more than 1 year.
second percutaneous needle biopsy confirmed primary AdC. ● Surgical resection confirmed primary AdC. ◆ After 1 year of follow-up, 2 patients kept stable or lesion decreased, 1 patient diagnosed benign through transbronchial needle aspiration(TBNA).
4 of them diagnosed of benign through Surgical resection; 1 malignant and 1 benign confirmed through new biopsy; 2 confirmed malignant by Surgical resection; After 1 year of follow-up, 1 patient's lesion decreased.
2 confirmed benign through new biopsy; 1 diagnosed as metastatic AdC and 1 benign through Surgical resection.
Correlation Between Malignant /Benign and Nodular Consistency (2 Groups, n = 210).

Discussion
The lungs move up and down with breathing, especially the lower lung. Thus, the location of the pulmonary lesion is not fixed. Therefore, the position of the image marker during positioning may be different from the actual position after needle insertion. In addition, the lung is a loose air-containing organ with abundant internal blood vessels. In biopsy, a puncture needle is generally required to pass through normal lung tissue to reach the lesion. Pneumothorax, pulmonary hemorrhage or even air embolism may occur during repeated passages through the pleura and lung tissue. Based on these characteristics, needle biopsy for small pulmonary nodules is more difficult, and the probability of complications is increased.
Studies indicated that 3-D–printed navigational template has acceptable accuracy and safety for localization of small peripheral lung nodules,8,11,12 This revelation makes it possible to apply the 3-D-printed template to percutaneous core needle biopsy of pulmonary nodules, but only Ji, et al 9 reported the application of this technology, due to control group was not set, and their results were only compared with previous literature. Therefore, we conducted a retrospective and comparative study to further explore the clinical application value of 3D-printed coplanar puncture template-assisted CT-guided percutaneous core needle biopsy of pulmonary nodules (≤30 mm). In the present study, due to the different biopsy method, the diagnostic yield of 3D-PCT-assisted CT-guided percutaneous CNB puncture was 95.2%, which was significantly higher than 87.7% in the control CNB group (P < .05). In previous study, Ohno et al 13 reported that overall diagnostic accuracy were 77.2% for CT-guided transthoracic needle aspiration biopsy of small (< or =20 mm) solitary pulmonary nodules, and Yoshimura et al 7 reported a diagnostic accuracy of 87% during CNBs of nodules smaller than 20 mm. Li et al 14 got a highest overall diagnostic accuracy of 93.5% for small (≤20 mm) pulmonary lesions in their retrospective study, however, the diagnostic yield of pulmonary nodules (<2 cm) in 3D-PCT group in our study is higher. Actually, both the 3D-PCT group and the control group, the diagnostic yield of pulmonary nodules >or =2 cm was higher than that of pulmonary nodules <2 cm, which is consistent with the report by Kothary et al, 6 who concluded that diagnostic accuracy of CT-guided percutaneous lung biopsy of lung nodules< or =1.5 cm is slightly lower than (P < .05) that of nodules >1.5 cm. As Shimizu et al 15 reported, satisfactory diagnostic yield (>80%) was obtained by CT-guided fine needle aspiration biopsy in cases larger than 15 mm.
Pneumothorax and pulmonary hemorrhage are the most common complications during percutaneous core needle biopsy of pulmonary lesions. The incidence of pneumothorax in the previous article was generally between 15% and 62%.6,16–21 A previous study reported that risk factors for the development of biopsy-related pneumothorax include the presence of chronic obstructive pulmonary disease (COPD), 22 small lesion size,23,24 a long needle path,23,25 and technical factors, such as repeated pleural puncture 26 or a wider insertion angle of the needle. 27 We excluded COPD patients in our study, thereby avoiding patient-related risk factors for pneumothorax. According to the present research results, the incidence of pneumothorax in the 3D-PCT group was not significantly higher than that in the control group, the reason may be attributed to the fact that there is no difference in risk factors for the development of biopsy-related pneumothorax. Risk factors include lesion size, pleura-to-lesion, and the percutaneous CNB was implemented by experienced pulmonologist and radiologist (Dr Ren and Dr Wang), which excluded technically induced artificial pneumothorax.
According to reports, incidence of pulmonary hemorrhage ranges from 4% to 43%,16,24,25,28 the present study revealed intrapulmonary hemorrhage rates of 7.7% (8/104) and 9.4% (10/106) for the two groups, respectively, and showed no significant differences. The incidence of hemorrhage in two groups is consistent with previous reports. In present study, Biopsy needle adjustments require CT scans to determine whether the angle and depth are adjusted correctly, so an increased number of CT scans was associated with an increased number of needle adjustments. With the assistance of a 3D-printed coplanar puncture template, the number of biopsy needle adjustments is significantly reduced, avoiding more iatrogenic radiation CT scans for patients.
The average surgical time in the 3D-PCT group was significantly greater than that in the control group, which was due to the increased time requirement for prepuncture preparation, including installation of the navigation system and 3D-PCT, in the 3D-PCT group.
Among the 121 malignant cases in this study, solid nodules accounted for 62.8%, followed by partly solid GGO, accounting for 24.8%, and finally pure GGO, accounting for 12.4%, the malignancy rate was significantly higher for partly solid GGO than for pure GGO, it is consistent with Henschke et al statement. 29
Although all procedures were performed by two experienced pulmonologists and radiologists in present study, a limitation of our study is that its retrospective, single center nature and the sample size was not large enough, maybe lead to some imperfect in findings. Right now, a prospective study of 3D-PCT-assisted percutaneous lung biopsy is ongoing in our unit, and some of the questions may have answers in the future.
Conclusion
Our study concluded that 3D-PCT-assisted CT-guided percutaneous CNBs for pulmonary nodules can increase the diagnostic yield and reduce the number of biopsy needle adjustments; the disadvantage is that the operation time of 3D-PCT is longer, the cost is higher. Therefore, based on the improvement of diagnostic yield, it has certain clinical promotion value, especially for pulmonary nodule smaller than 2 cm.
Supplemental Material
sj-pdf-1-tct-10.1177_15330338221089940 - Supplemental material for Application of 3-Dimensionally Printed Coplanar Template Improves Diagnostic Yield of CT-Guided Percutaneous Core Needle Biopsy for Pulmonary Nodules
Supplemental material, sj-pdf-1-tct-10.1177_15330338221089940 for Application of 3-Dimensionally Printed Coplanar Template Improves Diagnostic Yield of CT-Guided Percutaneous Core Needle Biopsy for Pulmonary Nodules by Hansheng Wang, MD, Tao Ren, PhD, Peipei Chen, BD, Guoshi Luo, BD, Na Wei, BD, Yijun Tang, PhD, and Meifang Wang, PhD in Technology in Cancer Research & Treatment
Footnotes
Abbreviations
Acknowledgements
We would like to acknowledge all members of the department of Pulmonary and Critical Care Medicine, Taihe Hospital, Hubei University of Medicine.
Conflict of interest statement
The authors declare that they have no competing interests.
Funding
This work was supported by Educational Commission of Hubei Province of China (B20122414, Q20112106) and Science and Technology Research Project of Hubei Provincial Department of Education (No: D20152014)
Ethics Approval and Consent to Participate
This study was approved by the Taihe Hospital Ethics Committees (2018KS027) and was performed in accordance with the principles of Good Clinical Practice following the Tri-Council guidelines. All patients or their substitute decision makers provided written informed consent prior to patients.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.